
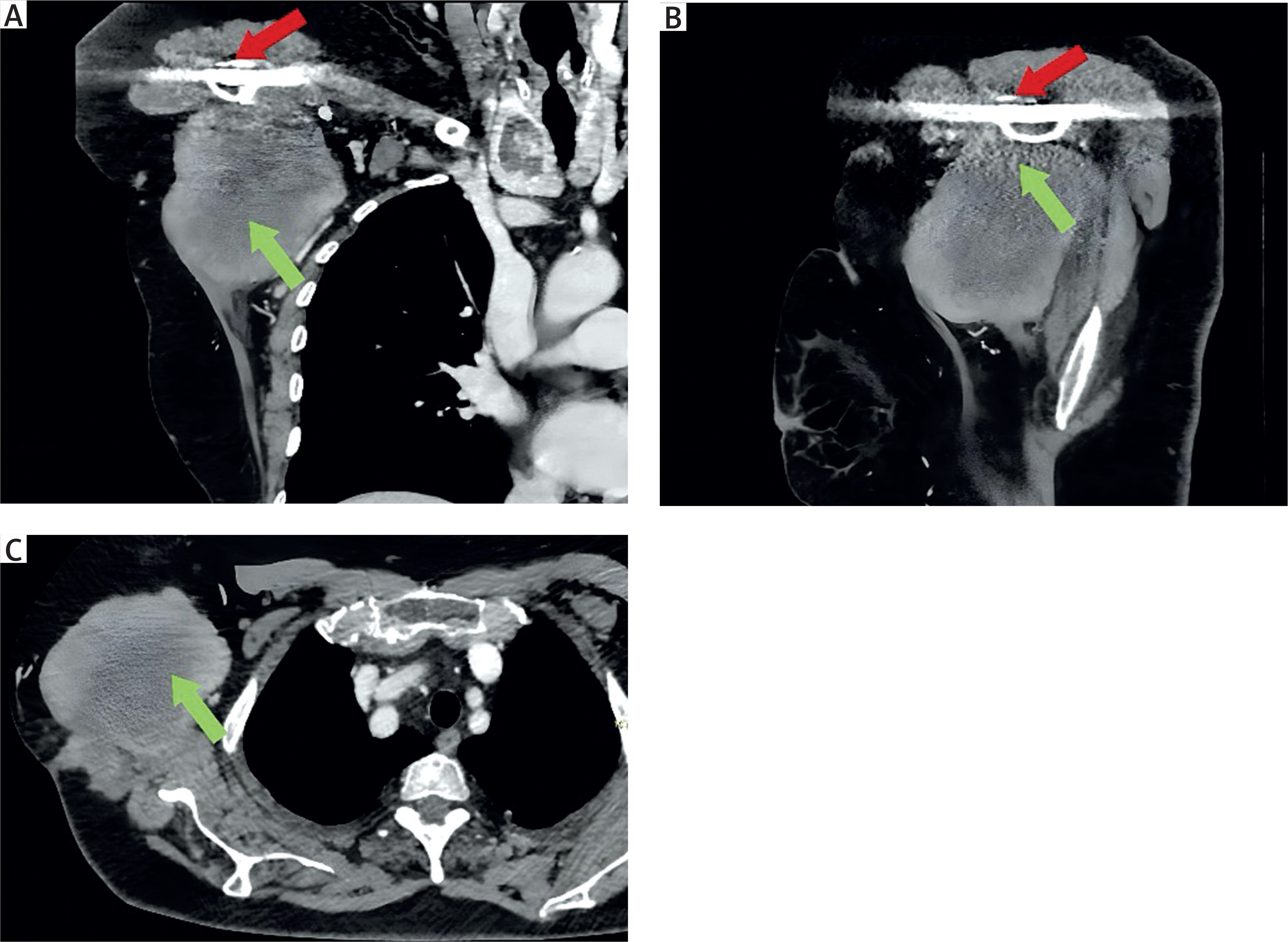
A 71-year-old woman was referred to our department due to the presence of a lesion in the right chest wall, arising from the axillary cavity, which had been increasing in size during the last 3 years. She had a history of metabolic disorders and surgical osteosynthesis of the right shoulder 4 years before, with the presence of titanium plate. Physical examination revealed a swelling approximately 10 cm in size on the right chest wall, firm and fixed to the underlying layers. This was associated with functional limitation of the right arm due to pain and mechanical limitation. The computed tomography (CT) scan with contrast showed a solid nodular mass in the right axillary cavity with finely irregular margins, heterogeneous contrast enhancement, and dimensions of approximately 10.5 × 8.3 cm (Figure 1).
Figure 1
Preoperative radiological imaging of a mass located in the right axillary cavity. A – Coronal section of computed tomography (CT) demonstrating the presence of the mass (green arrow) and a titanium plate in the shoulder (red arrow). B – Sagittal CT section highlighting the close anatomical correlation between the mass (green arrow) and the titanium plate (red arrow). C – Image of the lesion through an axial CT section (green arrow)
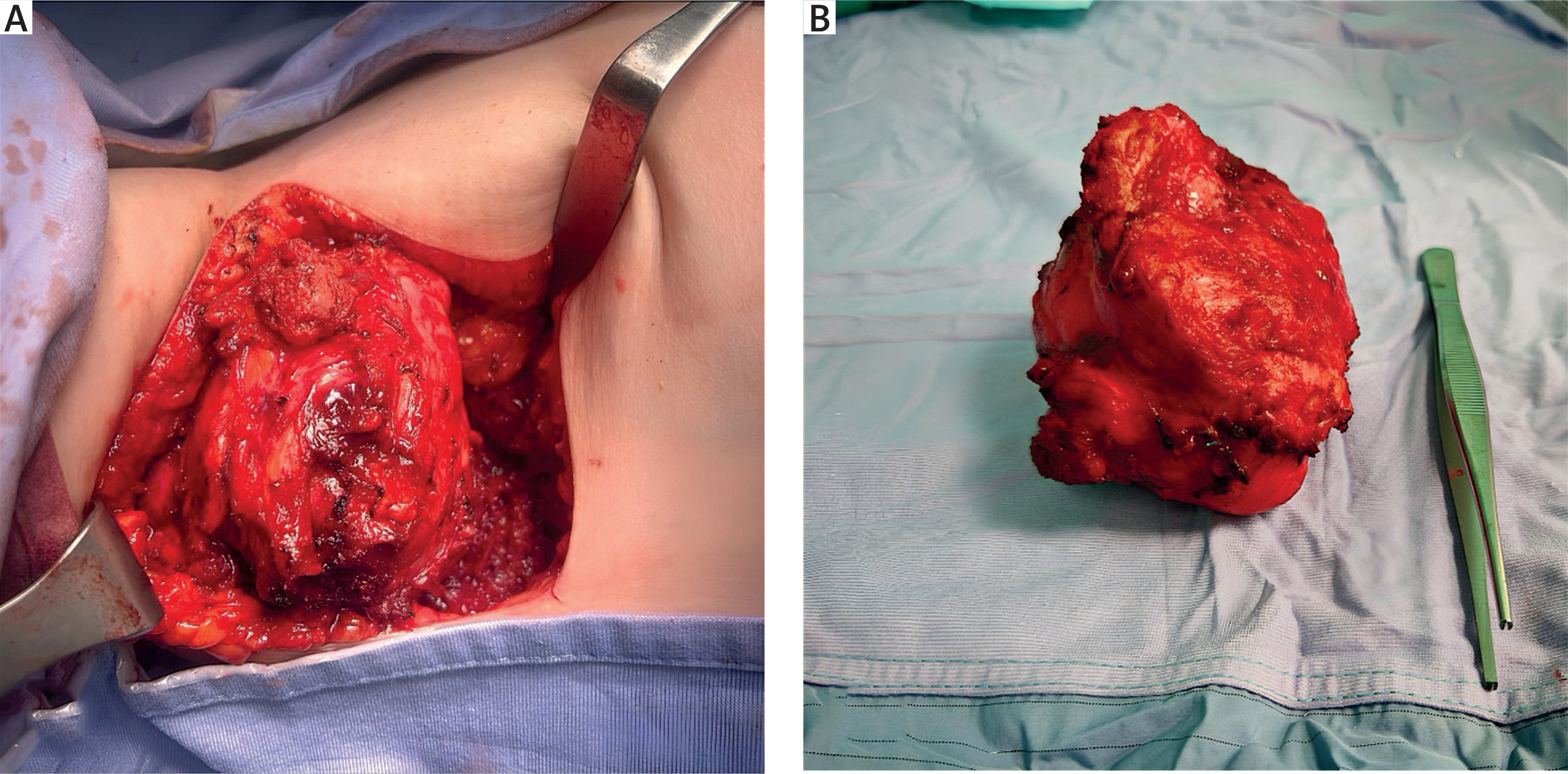
A surgical biopsy was performed, demonstrating a fibrotic lesion. Based on the imaging and histological results, surgical excision was indicated. The lesion fully occupied the axillary cavity and was firmly adherent in part to several fibers of the latissimus dorsi muscle, which were consequently sacrificed, while no vascular or nervous infiltration was detected, although the lesion presented strong adhesion to vascular and nervous structures (axillary vein and artery, brachial plexus fibers). Additionally, the lesion was closely adherent to the titanium plate of the previous orthopedic intervention, suggesting a possible origin from this event. Finally, after blunt and scalpel dissection, the lesion was completely removed with macroscopic free margins (Figure 2). The final histological examination confirmed fibromatous tumor, with a typical immunohistochemical profile: SMA (+), Caldesmon (–), cytokeratin AE1-AE2 (–), S100 (–) and low Ki-67 (3–5%).
Figure 2
Intraoperative image of a thoracic wall mass. A – Visualization of progressive dissection of the tumor from adjacent tissues during the excision phase. B – Postoperative image of the surgically resected lesion
Fibromatosis of the chest wall is a benign soft tissue tumor [1] that does not have metastatic potential but has a high rate of local-regional invasion, which is the main cause of mortality and morbidity [2]. Desmoid tumors are a type of deep fibromatosis that may arise in the abdominal wall, intra-abdominally or extra-abdominally, with an incidence of approximately 2–4 million per year. They are more common among women between the ages of 30 and 40 [3].
The histological diagnosis is based on immunohistochemical analysis and is typically made after surgery. Surgical resection with negative margins of 2 to 4 cm has historically been the treatment of choice [4]. Additional treatment options include radiotherapy, non-steroidal anti-inflammatory drugs, and conventional cancer chemotherapy [5, 6].
These tumors originate from a well-differentiated myofibroblastic proliferation attributable to a multifactorial etiology such as genetic, hormonal or traumatic causes (including surgery).
In the reported case, the origin of the tumor appears to be associated with plate osteosynthesis of a humeral fracture performed 4 years prior to presentation. The lesion may have developed after surgical treatment and exhibited a relatively high growth rate. The patient reported a recent acceleration in lesion growth, prompting pre-operative biopsy to confirm the nature of the lesion. Notably, knowledge of the timing of the traumatic event allows estimation of the growth rate, potentially providing clinical insights regarding such tumors. However, although the position presented a risk of incomplete resection and nervous or vascular injuries, complete resection was achieved with clear margins, requiring the resection of only a portion of the latissimus dorsi muscle.
In conclusion, this case illustrates that surgery can be an effective and safe option for the treatment of these uncommon tumors. It further highlights the importance of pre-operative histological confirmation to exclude other diagnoses.









