
Purpose
Brachytherapy (BRT) is a commonly used treatment modality for gynecological cancers, including cervical and endometrial carcinomas, achieving local tumor control by delivering high radiation doses to target volume while sparing adjacent healthy tissues. BRT can be applied alone or in combination with external beam radiation therapy (EBRT) [1-5]. High-dose-rate (HDR) adjuvant vaginal brachytherapy (VBRT) is used to reduce the risk of residual microscopic disease in the vaginal apex and wall after surgery for endometrial cancer. While these treatments are mostly delivered using cylindrical applicators, ovoid applicators may be preferred in some cases [6]. Interstitial BRT techniques are recommended for vaginal lesions exceeding 5 mm in depth [2].
Accumulating evidence indicate that VBRT significantly reduces the risk of vaginal recurrence in early-stage endometrial cancer, with the exception of patients with multiple risk factors [2-5, 7]. The likelihood of complete remission following adjuvant VBRT depends in part on the accurate and precise delivery of the prescribed dose to the vaginal mucosa as well as the underlying tissues, which may harbor microscopic residual disease. Studies have shown that the vaginal apex and mid-vaginal canal are the most frequent sites of recurrence within the vagina [4, 7-9]. Therefore, therapeutic objective is to ensure adequate delivery of the prescribed dose to a depth of approximately 5 mm at both the apex and vaginal wall in the defined target volume, to achieve optimal local control. Effective treatment relies on the selection of applicator that is appropriate for the patient’s vaginal anatomy to ensure optimal contact with the vaginal surface. Optimal placement minimizing air voids between the applicator and vaginal wall, enhances dose homogeneity and ensures adequate dose delivery to target tissues, thereby improving treatment efficacy.
In single-channel (SC) cylindrical applicators commonly used in VBRT, dose optimization is limited by a single catheter located in the central axis. This often leads to sub-optimal dose distribution to the target volume, resulting in doses to organs at risk (OARs) exceeding recommended limits [10]. To address this issue, multi-channel (MC) cylindrical applicators, featuring multiple catheters positioned both centrally and at equidistant peripheral points, have been developed to enable patient-specific dose optimization [11]. The use of MC applicators allows individualized dose tailoring while reducing OARs dose exposures [1, 3, 10, 12, 13]. Although dose optimization is achieved with MC applicators in VBRT, some reports indicate that increased doses may occur in the vaginal mucosa owing to contributions from peripheral catheters [13, 14].
The present study aimed to compare the target volume, OARs volumes, and the resulting dose distributions on the vaginal surface achieved with MC and SC cylindrical applicators of various diameters in patients undergoing VBRT post-hysterectomy for endometrial cancer. In addition, by comparing MC and SC applicator configurations, this study evaluated the effect of applicator diameter on small volume vaginal mucosal hot-spot doses (D0.1 cc), and presented equivalent doses in 2 Gy fractions (EQD2, calculated with an α/β ratio of 3) according to commonly used fractionation schemes. This approach provides information applicable to clinical practice beyond the conventional MC-SC dosimetric comparison.
Material and methods
This retrospective study included patients diagnosed with endometrial cancer, who underwent HDR-VBRT using MC applicator. Patients were identified from the institution’s archive according to diameter of MC applicator used for treatment. VBRT was administered either as a separate treatment or following EBRT. To ensure a homogeneous distribution of applicator diameters, patients were stratified into three groups, in which 25, 30, and 35 mm MC applicators were used; a total of 60 patients (20 in each group) were included. Each patient underwent computed tomography imaging after vaginal implant placement (Brilliance Big Bore v. 3.6; Philips Healthcare). A slice thickness of 3 mm was used according to the institution’s routine clinical imaging protocol for HDR-VBRT planning, providing adequate spatial resolution for applicator reconstruction and contouring. The acquired images were transferred to Oncentra treatment planning system (version 4.7; Elekta AB, Stockholm, Sweden). In accordance with institutional practice, an experienced radiation oncologist contoured OARs volumes, including the bladder, rectum, and sigmoid colon. Clinical target volume (CTV) was defined by an experienced medical physicist as the volume obtained by delineating a vaginal cylinder along the patient-specific upper vaginal length (CTVlength), including the vaginal apex, with a 5 mm margin, and subsequently subtracting the cylinder volume. The resulting patient-specific CTVlength values are summarized in the Results section as mean ± standard deviation. Similarly, to evaluate the dose to vaginal surface, a three-dimensional vaginal mucosal volume was defined by the same medical physicist by subtracting the cylinder volume from the volume obtained by delineating a vaginal cylinder around the vaginal apex with a 2 mm margin. The definitions of CTV and vaginal mucosal volumes are provided in Figure 1.
Fig. 1
Schematic illustration of applicators with the vaginal mucosa, reference depth (5 mm), and clinical target volume (CTV) length
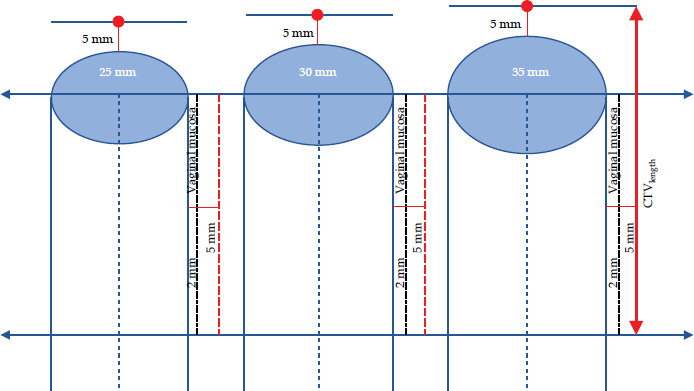
A MC applicator with 25 mm diameter (Nucletron; an Elekta Company, Elekta AB, Stockholm, Sweden) had a central axis channel and six peripheral channels, whereas the applicators with 30 and 35 mm diameters had eight peripheral channels surrounding the central axis channel. In each applicator, all peripheral channels, together with the central axis channel, were activated with a 5 mm source step size along the CTV. For dosimetric comparison, new treatment plans were generated for each patient by simulating a SC applicator through activation of only the central axis channel of a MC applicator, while maintaining identical geometric and dosimetric conditions. Applicator reconstruction was performed for all plans using a digital applicator library. In all plans, the prescribed dose to the CTV was normalized to a depth of 5 mm from the vaginal surface, aiming to deliver 90% of the dose to 90% of the CTV. In the treatment planning system, dose optimization for all plans was performed by the same medical physicist using point dose normalization and graphical optimization.
For the CTV, volumes receiving 90%, 95%, 98%, 100%, and 150% of the prescribed dose (V90, V95, V98, V100 and V150, respectively) were compared with doses received by 90%, 95%, and 98% of the target volume (D90, D95, and D98, respectively). For OARs volumes of the bladder, rectum, and sigmoid colon, doses delivered to 0.1 cc, 1.0 cc, and 2.0 cc of each volume (D0.1cc, D1.0cc, and D2.0cc, respectively) were evaluated. Furthermore, target volume length (CTVlength) and point dose at a depth of 5 mm on the central axis at the vaginal apex (Dvaginal apex+5mm) were recorded for each patient. For the vaginal mucosa, dose delivered to 0.1 cc (D0.1cc) was compared with a maximum point dose within the mucosal volume (Dmax). All values were calculated relative to the target volume dose, and the results were presented as means. Additionally, EQD2 values for 0.1 cc vaginal mucosal doses obtained with both SC and MC applicators were calculated, assuming an α/β ratio of 3 Gy.
Normality was assessed using Shapiro-Wilk test. As most parameters deviated from a normal distribution, non-parametric statistical tests were applied. Paired samples Wilcoxon signed-rank tests were employed to compare values obtained with MC and SC applicators. Additionally, Kruskal-Wallis test was used to assess differences according to applicator diameter within each group, and post-hoc tests were performed wherever appropriate. Statistical significance was set at p < 0.05, and all analyses were performed using SPSS v. 27 (IBM Analytics; Armonk, New York, USA).
Results
In this study, dose distributions were evaluated for 60 patients treated with 25, 30, and 35 mm diameter applicators. For each case, dose distributions were first calculated using the MC applicator and subsequently compared with the plans re-calculated under identical planning conditions using the SC applicator in the same patient cohort. With this approach, 120 treatment plans were analyzed.
The results of this study are presented in Table 1. The mean patient-specific upper vaginal length (CTVlength) was 5.22 cm (±0.06). For CTV dose distributions, both the volume receiving 90% of the prescribed dose (V90) and the dose delivered to 90% of the volume (D90) exceeded 90% for all MC diameters in both applicator groups. However, with the SC applicator, the D90 value was above 90% only with a 35 mm diameter. The difference between the two applicator types was statistically significant, particularly with the smallest (25 mm) diameter applicator (Supplementary Tables 1 and 2). Additional detailed results are provided in the Supplementary Tables 1-3.
Table 1
Results obtained from single-channel (SC) and multi-channel (MC) applicators with diameters of 25, 30, and 35 mm (mean ± SD, expressed as percentage of prescription dose). Volume-based parameters (0.1 cc, 1.0 cc, and 2.0 cc) represent absolute sub-volumes expressed in cubic centimeters
Table 2
Dose values received by specified volumes of the vaginal mucosa (% mean ± SD, expressed as percentage of prescription dose). Volume-based parameters (0.1 cc, 1.0 cc, and 2.0 cc) represent absolute sub-volumes expressed in cubic centimeters
Table 3
Inter-applicator comparison of dose values received by specified volumes of the bladder, rectum, and sigmoid between single-channel (SC) and multi-channel (MC) applicators for each applicator diameter (mean ± SD, expressed as percentage of prescription dose). Volume-based parameters (0.1 cc, 1.0 cc, and 2.0 cc) represent absolute sub-volumes expressed in cubic centimeters. Applicator diameters are given in millimeters (mm)
In all patients, the doses measured at the vaginal apex at a prescription depth of 5 mm were higher with 25 and 30 mm SC applicators than with MC applicators, whereas a higher dose was observed using a 35 mm diameter MC applicator. For the vaginal mucosa, there was no significant difference in D0.1cc between the 25 and 30 mm diameter MC and SC applicators, while the 35 mm diameter group showed significantly higher doses using the SC applicator (p = 0.048) (Table 2). With applicator diameters of 25 and 30 mm, higher vaginal mucosal doses were seen when using the MC applicator. An evaluation according to applicator diameter demonstrated decreasing vaginal mucosal dose with increasing applicator diameter for both the SC and MC plans (Supplementary Table 3).
Doses delivered to OARs were compared between the MC and SC plans for each applicator diameter, and the results are summarized in Table 3. No significant differences were observed between the MC and SC applicators for any of the bladder volume parameters. For rectal doses, no significant difference was noted between 25 and 30 mm diameters for either applicator type. However, significantly lower rectal doses at 1.0 cc (D1.0cc) and 2.0 cc (D2.0cc) were obtained with the 35 mm diameter applicators in favor of the MC applicators (p = 0.037 and p = 0.014, respectively). A similar trend favoring the MC applicator was also observed for the sigmoid colon dose. In applicators with diameters of 25 and 30 mm, significantly lower doses were observed with the MC applicator across all volume parameters. In contrast, no significant difference was observed between the SC and MC plans for the 35 mm diameter applicator.
Table 3 presents the inter-applicator comparisons between the MC and SC applicators for each diameter, whereas Table 4 shows the intra-applicator comparisons evaluating diameter-dependent differences within the same type of applicator. For the CTV, there was no evident difference between different diameters of the MC applicator. However, with the SC applicator, the 35 mm device yielded significantly higher doses than the 25 mm applicator at V95, V98, and V100. The dose at a depth of 5 mm from the vaginal apex tended to decrease as the SC applicator diameter increased (Table 4).
Table 4
Intra-applicator evaluation of dosimetric results according to applicator diameter for single-channel (SC) and multi-channel (MC) applicators (mean ± SD, expressed as percentage of prescription dose). Volumebased parameters (0.1 cc, 1.0 cc, and 2.0 cc) refer to absolute sub-volumes in cubic centimeters. Applicator diameters are given in millimeters (mm)
Vaginal mucosal doses did not demonstrate significant variation across different diameters within the same applicator type. However, a progressive reduction in the mucosal dose was observed with an increasing diameter for both applicator types. Evaluation of the doses to OARs volumes revealed no significant difference between the applicator diameters for the bladder. However, significant differences were observed in certain dose parameters for the rectum and sigmoid colon. Also, considerable differences were noted in the sigmoid colon doses between the narrowest and widest diameters of both SC and MC applicator types.
Discussion
Single-channel applicators are commonly used in VBRT for treatment of endometrial cancer. Conversely, MC applicators, which provide an asymmetrical dose distribution, allow prescribed dose to be achieved in target volume while offering improved OARs protection [10, 12, 15]. The present study aimed to compare the doses generated by both SC and MC applicators of different diameters within OARs volumes and on the vaginal surface.
Based on the obtained data, the prescribed target dose coverage was achieved for all MC applicator diameters. For SC applicator, the D90 value exceeded 90% only with the 35 mm diameter. However, when evaluated as per applicator diameter, a significant difference was observed for D90 only with the 25 mm diameter applicator (p = 0.001) (Supplementary Table 2). For 30 and 35 mm diameter applicators, the dose coverage in the target volume appeared comparable for both applicator types. Although identical optimization objectives were applied to both MC and SC plans, achieving D90 ≥ 90% for the CTV was not always feasible with SC applicators because of the inherent geometric limitations associated with a single-central source channel. In contrast, the additional degrees of freedom provided by peripheral channels in MC applicators allowed more effective dose shaping and target coverage under the same conditions. A phantom-based study using a SC applicator indicated that applicator diameter significantly impacted the desired dose distribution [16]. Similarly, another study conducted with a SC applicator reported that target volume coverage and dose homogeneity improved with increasing cylinder diameter [17]. The present study is among the few reporting target volume coverage according to the diameters of both MC and SC applicators. In our research, to enable a controlled dosimetric comparison, SC plans were generated by disabling the peripheral channels of MC applicator. Therefore, identical geometric conditions were maintained, and the effects of channel configuration and applicator diameter were isolated.
We acknowledge that the placement of a dedicated SC applicator in routine clinical practice may lead to minor geometric differences, thus we consider that a limitation of this controlled dosimetric study design.
The 5 mm depth point at the vaginal apex is known to be the most frequent site of vaginal recurrence following hysterectomy for endometrial cancer, and therefore, this should be used as the prescribed depth in VBRT applications [2, 3, 7]. Literature on the use of SC applicators indicates that the dose at the vaginal apex may fall below the desired level due to source anisotropy [11, 18]. The present study demonstrates that the doses measured at a 5 mm depth at the vaginal apex increased as the applicator diameter increased with the MC applicator, whereas the doses decreased significantly with the SC applicator. This difference may be attributed to the geometric structure of applicators. This observed diameter-dependent dose increase with the MC applicator is likely attributable to the contribution of peripheral channels, particularly at the vaginal apex.
In a comparison of MC and SC applicators for each diameter at a 0.1 cc (D0.1cc) vaginal mucosal dose, the MC applicator with the narrowest diameter yielded higher vaginal mucosal doses than the SC applicator, whereas the largest, 35 mm diameter applicator produced a significantly lower vaginal mucosal dose (p = 0.048). When vaginal mucosal doses were evaluated for diameter-dependent differences within the same applicator type, it was observed that with the MC applicator, doses decreased as the diameter increased; this reduction was even more significant with the 35 mm diameter (p = 0.029). However, in the SC applicator, the tendency for the dose to decrease as the diameter increased differed from that of the MC applicator. In the SC applicator, the highest vaginal mucosal dose was found with the narrowest diameter applicator (25 mm), similar to the MC. But the lowest vaginal mucosal dose was obtained with the 30 mm diameter applicator, although no significant difference was found.
Studies in this field have shown that MC applicators provide lower doses to OARs volumes while achieving higher doses in the vaginal mucosa [13, 19]. In the present study, the dose differences between the MC and SC applicators were relatively small. This finding suggests that the small volume dose parameters of vaginal mucosa are dependent not only on applicator type, but also on applicator diameter, channel geometry, and dose optimization. Peripheral channels are located closer to the applicator surface, which may contribute to higher small volume vaginal mucosal doses, particularly when smaller diameter MC applicators are used. Although the general dosimetric advantages of multi-channel over single-channel applicators have been previously reported, the present study was not intended to re-establish this known superiority. Instead, our analysis focused on how applicator diameter and channel geometry interact to influence small volume vaginal mucosal hot-spot doses (D0.1cc), an aspect that has received limited attention in previous studies. These findings highlight the importance of individualized applicator selection and planning strategies rather than reliance on channel number alone.
Given that the vaginal mucosa is a thin, superficial, and highly radiosensitive tissue, the mucosal dose is a critical determinant of both acute and late toxicities in VBRT. Studies have shown that acute and delayed vaginal toxicities are significant concerns in VBRT [16, 20, 21]. Vaginal atrophy, stenosis, and/ or shortening, particularly involving the proximal vagina, have been identified as the primary toxicity risks associated with VBRT [4]. Severe vaginal stenosis may further compromise adequate pelvic examination, thereby limiting the timely detection of disease recurrence [22]. Evidence from previous studies suggest that high-dose regions are more predictive of vaginal toxicity than mean vaginal dose values [21-25]. Given the steep dose gradient along the vaginal wall in VBRT, small volume dose parameters are commonly used as surrogate indicators of local dose exposure within the vaginal mucosa. In the current study, the vaginal mucosal volume was defined as the tissue extending from the vaginal surface to a depth of 2 mm, and the mucosal dose assessment was based on the 0.1 cc and maximum doses.
The present research is limited by its exclusive focus on dosimetric parameters and the absence of a direct correlation with clinical toxicity outcomes. Given the retrospective design, variable follow-up duration, and heterogeneity in adjuvant treatment regimens, the dosimetric findings should be interpreted as surrogate indicators of potential toxicity risk rather than direct predictors of clinical outcomes. Prospective studies incorporating standardized toxicity assessments are warranted to validate our observations.
In addition to these findings, the EQD2 (α/β = 3) values were calculated using the 0.1 cc vaginal mucosal dose for commonly used fractionation schemes (Supplementary Table 3). Consistent with the vaginal mucosal dose results, an increase in the diameter of both applicator types was associated with a decrease in the EQD2 vaginal mucosal dose. Therefore, these values should be interpreted as representative high-dose points within the vaginal wall when VBRT is delivered as a standalone treatment or in combination with EBRT, providing a practical reference for clinical use. Previous studies have reported that a most irradiated 2.0 cc EQD2 (α/β = 3) dose exceeding 68 Gy in the vagina is associated with grade 2 vaginal toxicity; however, this threshold was derived from patient cohorts treated with combined EBRT and VBRT [26]. As no universally accepted EQD2 dose constraints exist for the vaginal mucosa in sole VBRT treatment, the EQD2 values presented in this study should be considered at institutional reference levels rather than universal toxicity thresholds. In line with this perspective, recent dosimetric studies have demonstrated that the applicator diameter and prescription depth substantially influence the vaginal surface dose and EQD2 values across commonly used HDR-VBRT fractionation schemes, underscoring the clinical relevance of diameter-dependent dose evaluation [27].
Considering the limitations of the present study, further analyses with larger patient cohorts are planned, incorporating both small volume hot-spot parameters (D0.1cc) and D2.0cc metric, which represents the most irradiated 2 cm3 of the vagina.
Conclusions
This study aimed to evaluate the effects of MC and SC cylindrical applicators with different diameters on dose distribution to target volumes and OARs in VBRT. Overall, the findings indicate that the use of MC applicators with appropriate target volume dosimetry, has the potential to achieve lower dose exposure in OARs, such as the bladder, rectum, and sigmoid colon. Conversely, for small and medium diameter applicators (25 and 30 mm), higher small volume vaginal mucosal doses were observed with MC than with SC applicators. These results underscore that the vaginal mucosal dose is influenced not only by applicator type, but also by applicator diameter and dose distribution geometry. Although recent advances, such as 3D-printed applicators, offer promising opportunities for improved geometric conformity, standard SC and MC applicators remain widely used in routine clinical practice [12, 28]. Therefore, understanding diameter-dependent mucosal dose behavior with commonly available applicators remains clinically relevant, and may indicate safe adoption of newer applicator designs.
In conclusion, although MC applicators offer clear advantages in VBRT planning with respect to target coverage and OARs dosimetry, vaginal mucosal doses require careful evaluation, particularly when small diameter applicators are employed. This emphasizes that both careful optimization and diameter selection are essential to balance target coverage, OARs sparing, and vaginal mucosal safety.








