
Introduction
Although the learning curve is generally thought to be part of medical education, it is also a very important part of residency training and beyond, especially in surgical clinics. In Turkey, training for many surgical procedures is provided during the residency period. However, the duration of residency for complicated surgeries in some surgical clinics is controversial. In China, cardiac surgeons lack formal training in coronary artery anastomosis in the early stages of their careers until they can perform general cardiac procedures such as valve replacement [1]. In the United States, after a 5-year general surgery residency, they are required to complete a cardiothoracic surgery residency [2]. In the Australian system, trainees in cardiac surgery have undergone a minimum of 3 resident medical officer years in surgery following an intern year, 2 years as general surgery trainees, and then 4 trainee years in cardiac surgery [3]. In Turkey, the residency period for cardiovascular surgery is 5 years, and at the end of this period, surgeons who complete their practical and theoretical exams are given competence and responsibility for all cardiovascular operations, except for the heart transplant program, which requires certification. For congenital heart surgery, an additional 3 years of training are required.
The learning curve required for many specific operations in cardiac surgery cannot be completed within the relatively short 5-year training period. Therefore, many young surgeons usually complete their learning curves for complex surgeries after their residency. Furthermore, it is debatable whether a young surgeon is capable of taking on the entire responsibility of open-heart surgery after residency. This issue is still controversial not only in cardiac surgery but also in other surgical clinics. There are limited studies in the literature comparing junior and senior surgeons. Liang et al. reported that the learning curve for young thoracic surgeons is shorter for single-port thoracoscopic lobectomy [4]. In the study by Adegboyega et al., surgeon seniority was not associated with recurrence in patients with chronic subdural hematoma [5]. In congenital heart surgery, junior surgeons have been found to achieve outcomes comparable to senior surgeons [6]. There are also studies on adult cardiac surgery such as coronary artery bypass grafting (CABG), aortic valve replacement (AVR), and mitral valve replacement (MVR) [3, 7–11]. In most of these studies, it has been reported that junior surgeons can perform these operations safely and have acceptable results. However, one of the most important limitations of these studies is that patients operated on by junior surgeons are usually selected. To address this issue, we designed the present study.
Aim
The aim of this study was to compare the postoperative results in detail in patients who underwent isolated CABG without patient selection between junior and senior surgeons and to investigate the adequacy of the 5-year residency training provided in Turkey.
Material and methods
This study was designed as a retrospective single-center observational study with a total of 514 patients. All patients over the age of 18 who underwent isolated CABG in the Cardiovascular Surgery Clinic of “Istanbul Basaksehir Cam and Sakura City Hospital” between January 2024 and March 2025 were included in the study. All cardiac surgeries other than CABG and patients who underwent concomitant procedures with CABG were excluded from the study. Patients were divided into two groups: Group A (n = 240) treated by junior surgeons and Group B (n = 274) treated by senior surgeons.
Although cardiac surgery is often performed as a team, the surgeon who operated primarily was accepted as the responsible surgeon in this study. Those with an active cardiac surgery period of < 10 years were classified as junior surgeons, and those with ≥ 10 years were classified as senior surgeons. Our hospital was opened in April 2020, and the Cardiovascular Surgery program started at that time. Since the frequency of operations in the first years was lower than in recent years and the operations in the first years were performed more frequently by senior surgeons, patients in the first 4 years were not included in the study. In addition, to prevent the effect of risk factors of more complicated surgeries, patients undergoing CABG, which is the most frequently performed procedure in cardiac surgery, were analyzed. The operations were performed primarily by a total of 8 junior surgeons and 7 senior surgeons. Determination of whether the operating surgeon was junior or senior was also confirmed by checking the records. No selection criteria were set for the operations considering patient characteristics and comorbid diseases. Patients undergoing emergency and salvage operations, and those with low ejection fraction (EF), poor vascular structure, etc., were operated on and followed up by the responsible surgeon, regardless of whether the surgeon was junior or senior.
The medical records of all patients were reviewed, and basic demographic characteristics, medical history, transthoracic echocardiographic (TTE) findings, laboratory parameters, the European System for Cardiac Operative Risk Evaluation (EuroSCORE II), surgical procedure details, inotrope doses, amount of bleeding, blood product use, postoperative complications (postoperative exploration, cerebrovascular accident (CVA), continuous renal replacement therapy (CRRT) need, postoperative atrial fibrillation (POAF), superficial sternal wound infection (SSWI), deep sternal wound infection (DSWI), gastrointestinal bleeding, need for percutaneous coronary intervention (PCI), pleural effusion, need for intra-aortic balloon pump (IABP), need for extracorporeal membrane oxygenation (ECMO), tracheostomy, intubation time, intensive care unit (ICU) stay, hospital stay, total mortality, early mortality (< 30 days), and late mortality (≥ 30 days)) were recorded. Subsequently, comparisons were made between these two groups in terms of all these parameters. Patients who underwent dual antiplatelet surgery, those who underwent endarterectomy, and those who underwent beating heart surgery were excluded from the study, and thus new subgroups were created: Group C (n = 214) – junior surgeon subgroup; and Group D (n = 221) – senior surgeon subgroup. The postoperative outcomes were then compared again between these new subgroups.
This study was approved by the “Istanbul Basaksehir Cam and Sakura City Hospital” Ethics Committee (Decision no: 2025-136).
Statistical analysis
Data were analyzed using SPSS software version 20.0 (IBM, USA). Continuous variables in the study were presented as minimum, maximum, median, and interquartile range. Categorical variables were expressed as numbers and percentages. The normality of distribution was assessed by the Kolmogorov–Smirnov test. For numerical variables, differences between patients and controls were tested using the t test for parametric data or the Mann–Whitney U test for non-parametric data. Categorical variables were analyzed using the Pearson χ2 test and Fisher’s exact test. The level of statistical significance was set at p < 0.05.
Results
The basic demographic characteristics of the patients, comorbid diseases, TTE findings, risk scores, and operative data are shown in Table I. The mean age was 60±9.0 years, and 424 (82.5%) of the patients were male. The mean follow-up period was 211.8 ±140.4 days (median: 202, 0–449 days). There was no significant difference between the groups regarding basic demographic characteristics. Only weight and body surface area were higher in Group B. There was no difference between the groups in terms of comorbid diseases (diabetes mellitus (DM), hypertension, chronic obstructive pulmonary disease (COPD), history of CVA, chronic renal failure (CRF), history of malignancy, thyroid disorders, peripheral artery disease, rheumatic disease, atrial fibrillation). The proportion of patients operated on under dual antiplatelet therapy was higher in the junior surgeon group than in the senior surgeon group (11 (4.6%) vs. 4 (1.5%), respectively, p = 0.03). Preoperative mean EuroSCORE II was higher in the junior surgeon group than in the senior surgeon group (2.6% vs. 2.1%, respectively), although the difference was not statistically significant. Preoperative and postoperative New York Heart Association (NYHA) stages were similar between the groups. Preoperative and postoperative EF and tricuspid annular plane systolic excursion (TAPSE) values were also similar between the groups.
Table I
Comparison of patient demographics, comorbidities, and operative data between Groups A and B
There was no difference between the groups in terms of emergency operation rates. The mean number of bypass grafts was lower in the junior surgeon group than in the senior surgeon group (2.8 vs. 3.1, respectively, p = 0.001). The rate of left internal thoracic artery (LITA) use was similar between the groups. The proportion of patients who underwent beating heart surgery was higher in the senior surgeon group than in the junior surgeon group (35 (12.8%) and 11 (4.6%), respectively, p = 0.001). Proportions of those who underwent minimally invasive surgery were also similar between the groups. Cross-clamp (XCL) time and cardiopulmonary bypass (CPB) time were higher in the junior surgeon group than in the senior surgeon group (median XCL time: 86.5 vs. 67 min, p < 0.001; median CPB time: 136 vs. 115.5 min, respectively, p < 0.001).
The patients’ amount of bleeding, blood product usage, and postoperative inotrope requirements are shown in Table II. No difference was found between the groups in terms of norepinephrine levels below and above 0.1 µg/kg/min, dopamine below and above 10 µg/kg/min, and dobutamine below and above 10 µg/kg/min. No difference was found between the groups in terms of amount of bleeding on postoperative Day 1 and Day 2. No difference was found between the groups in terms of postoperative red blood cells (RBC), fresh frozen plasma (FFP), and platelet suspension usage. However, intraoperative median RBC, FFP, and platelet suspension usage were significantly higher in the junior surgeon group than in the senior surgeon group (p = 0.02, p = 0.03, and p = 0.001, respectively).
Table II
Comparison of bleeding, blood product use, and inotrope doses between Groups A and B
Comparisons of preoperative, intraoperative, postoperative day, and first postoperative month laboratory parameters between the groups are shown in Table III. No difference was found in preoperative white blood cells (WBC), hematocrit, urea, creatinine, sodium, potassium, alanine aminotransferase (ALT), aspartate aminotransferase (AST), C-reactive protein (CRP), glycated hemoglobin (HbA1c), or proBNP values. Laboratory values on the first postoperative day and at 1 month were generally similar between the groups. However, potassium and ASAT values on the postoperative first day and urea values at 1 month were higher in the junior surgeon group. While preoperative lactate values measured with arterial blood gas (ABG) were similar between the groups, lactate values measured after 30 minutes of XCL and on the postoperative first day were higher in the junior surgeon group than in the senior surgeon group (p = 0.04, p < 0.001, respectively).
Table III
Comparison of laboratory parameters between Groups A and B
A comparison of postoperative outcomes between groups is shown in Table IV. No statistically significant differences were found between the groups in terms of postoperative exploration, CVA, need for CRRT, POAF, SSWI, DSWI, gastrointestinal bleeding, need for PCI, pleural effusion, need for IABP, tracheostomy, intubation time, ICU stay, hospital stay, or total mortality, early mortality, and late mortality rates. The need for ECMO at any time during the postoperative period was found to be higher in the junior surgeon group than in the senior surgeon group (6 (2.5%) vs. 0, respectively, p = 0.01).
Table IV
Comparison of postoperative outcomes between Groups A and B
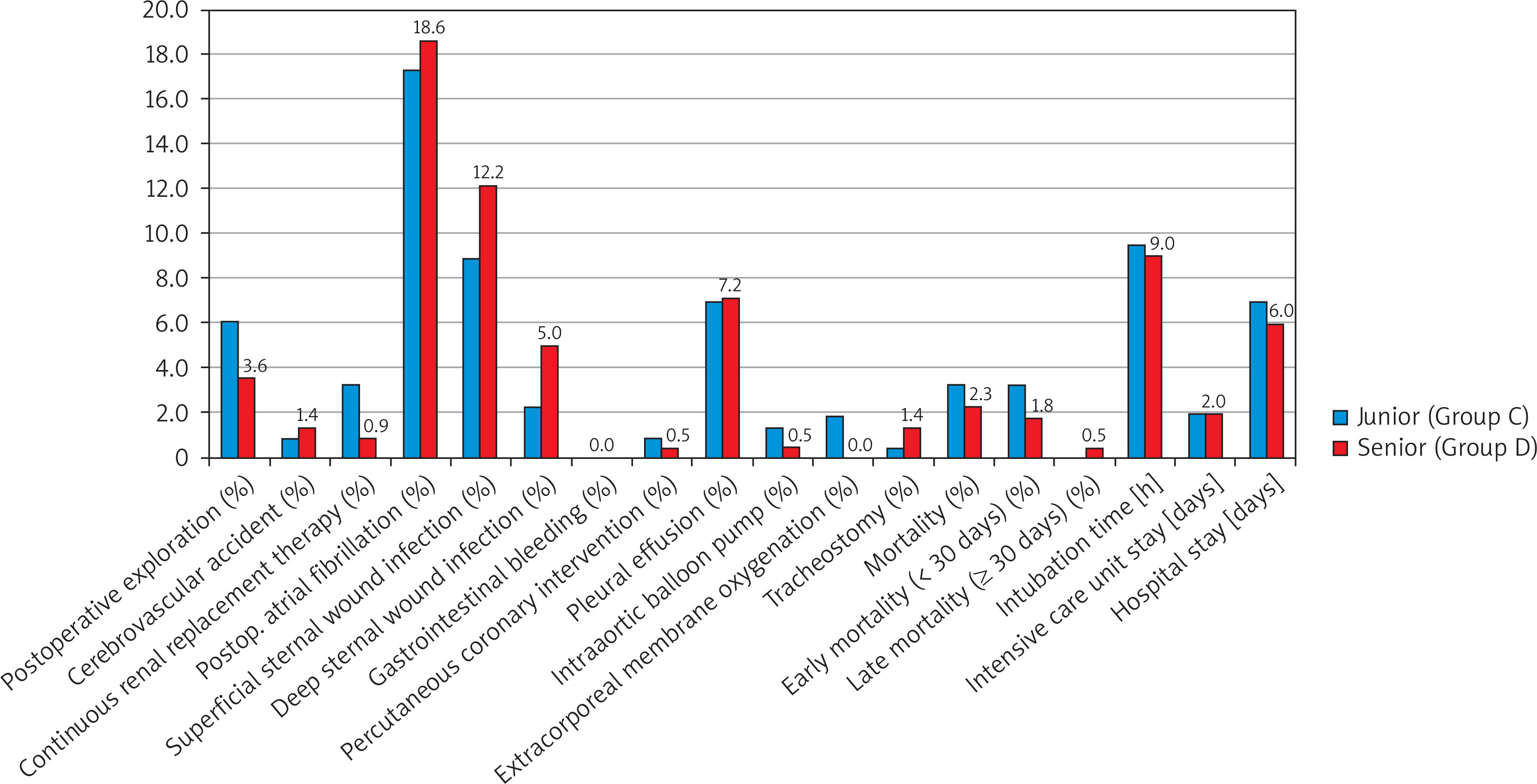
After excluding those operated on under dual antiplatelet therapy, those undergoing endarterectomy, and those undergoing beating heart surgery from the study, the subgroups were compared again for postoperative complications, and the findings are shown in Table V. Although the number of bypass grafts was lower in the junior surgeon group compared to the senior surgeon group, XCL and CPB times were higher (88 vs. 74 min, p < 0.001, and 140 vs. 121 min, p < 0.001, respectively). While intraoperative RBC and platelet suspension use were higher in the junior surgeon group, FFP usage amounts were similar. Lactate values 30 min after XCL and on the first postoperative day were also higher in the junior surgeon group. These results are also related to the longer XCL and CPB duration. However, no statistically significant difference was found between the junior and senior surgeon groups in terms of all postoperative outcomes in the primary analysis, including the need for ECMO (Figure 1).
Table V
Comparison of intraoperative data, blood product use, and postoperative outcomes between Groups C and D
Discussion
Cardiac surgery is a long-term training process that requires a master-apprentice relationship. The learning curve is extremely important for complex cardiac surgeries. Although these training stages differ between countries [1–3], it is a matter of debate whether a junior surgeon can successfully perform complex cardiac procedures as a primary surgeon shortly after residency training. Because of the importance of the learning curve, it is thought by both the public and surgeons that the outcomes of cardiac surgery for junior surgeons in their early years may not be as good as those of the senior surgeon group. It is often believed that junior surgeons are associated with higher morbidity and mortality, longer hospital stays, and increased costs. However, a study of trainees showed that hospital costs do not increase [8]. In addition, although it varies from person to person and depends on the training received, it is not certain how many years it will take to complete the learning curve. It is also not certain how many operations it will take to take on the full responsibility of CABG alone. The Royal Australasian College of Surgeons has defined the minimum operative experience in cardiothoracic surgery as trainees having assisted 400 CABGs and performed 70 CABGs [10]. In Germany, 100 cardiac operations must be performed independently under extracorporeal circulation in the last 2 years of training [12]. This discussion is held not only in cardiac surgery but also in many surgical clinics where complex operations are performed [4, 5, 13]. Burt et al. reported that in cardiac surgery, except CABG, surgeon experience is an important determinant of operative efficiency and long-term survival [14]. Although limited comparisons have been made for adult cardiac surgery, most of these studies used patient selection for young surgeons [3, 7–11, 15–18]. We believe that this is a valid reason to consider patient safety in a surgical clinic where there are significant morbidity and mortality rates, such as cardiac surgery, and where the learning curve takes years. However, the results of these studies may be biased due to patient selection. Therefore, to avoid such bias, we included all patients in this study, including those undergoing emergency procedures, patients with poor vascular structure, those with low EF, multiple comorbidities, those under dual antiplatelet therapy, those in cardiogenic shock who underwent salvage surgery, and patients with acute myocardial infarction. Therefore, the findings of this study provide valuable insights for comparing junior and senior surgeons.
The most common procedure in cardiac surgery is CABG; however, valve operations, aortic surgery, and many complex cardiac procedures are also performed. Because non-CABG cardiac procedures are performed less frequently, and given the complexity of valvular pathologies accompanying valve surgery, we included only patients who underwent isolated CABG in this study. For the definition of junior and senior surgeons, we determined the active cardiac surgery period as 10 years, independent of the academic title. Indeed, there may be surgeons who do not have an academic title but have performed active cardiac surgery for many years, and the opposite situation may also be possible. Under these criteria, we analyzed the data of 514 patients in 1 year, including the operations of 7 senior and 8 junior surgeons. As a result, we determined that there were comparable results in terms of postoperative outcomes in isolated CABG patients between junior and senior surgeon groups.
As seen in Table I, the basic demographic characteristics, comorbidities, emergency operation rates, and preoperative NYHA stages of the groups were similar. In addition, although not significant, EuroSCORE II scores were higher in the junior surgeon group than in the senior surgeon group. Preoperative laboratory parameters were also similar between the groups. With these findings, we can say that the patient groups had similar characteristics. Only the proportion of patients operated on under dual antiplatelet therapy was higher in the junior surgeon group than in the senior surgeon group. However, although the number of bypass grafts and coronary endarterectomy rates were higher in the senior surgeon group than in the junior surgeon group, XCL and CPB times were lower. However, since the bleeding risk would be higher in patients receiving dual antiplatelet therapy, and XCL and CPB times could affect the results in patients undergoing endarterectomy and beating heart surgery, we excluded these patients from the study and obtained new subgroups. As seen in Table V, as a result of our new analysis with Group C and Group D, while the number of bypassed grafts was lower in the junior surgeon group, XCL times (median 88 vs. 74 min) and CPB times (median 140 vs. 121 min) were longer. In the study by Stoica et al. comparing resident and staff cases, similar to our study, XCL times (79 vs. 70 min) and CPB times (117 vs. 107) were higher in isolated CABG [11]. This difference was an expected result due to the increasing experience over the years and the completion of the learning curve. However, we can say that this difference is comparable and acceptable and has no clinical significance. We did not detect a statistically significant difference between the groups in terms of all postoperative outcomes seen in Figure 1. We also did not detect a significant difference in the patients’ postoperative NYHA stages, or TTE findings such as EF and TAPSE.
In addition, as seen in Table II, we compared the postoperative norepinephrine, dopamine, and dobutamine usage rates between the groups as low and high-dose groups. We also did not find any difference in inotrope requirements between the groups. In the study by Baskett et al. comparing resident and staff operations in cardiac surgery, no difference was found in inotrope requirements [17]. However, unlike this and many other studies, in our study, all inotropes such as noradrenaline, dopamine, and dobutamine, which are frequently used in cardiac surgery, were compared separately with their dose ranges. This provides clearer information about inotrope requirements compared to other studies.
We compared the amount of bleeding on postoperative day 1 (400 vs. 400 ml) and day 2 (250 vs. 300 ml) separately. Although the XCL and CPB times were higher in the junior surgeon group than in the senior surgeon group, the amount of postoperative bleeding and the amount of all blood products used were similar between the groups. In the study by Ascione et al. comparing consultants and trainees in off-pump CABG patients, the median blood loss was found to be similar (777ml vs. 775 ml). They also reported that they did not find any difference in the amount of RBC, FFP, or platelet suspension used [15]. These results in our study were also similar to those reported in the literature. Despite the negative results in XCL and CPB, comparable results can be obtained in terms of bleeding amount with meticulous bleeding control. We only observed that intraoperative blood product use was significantly higher in the junior surgeon group than in the senior surgeon group. This is another important finding that has not been reported in other studies. Since there were more patients operated on under dual antiplatelet therapy in the junior group and this first comparison may not have given the correct result, we reanalyzed this in the subgroup we created. Intraoperative RBC and platelet suspension use were also higher in the junior surgeon group in the comparison of Groups C and D. This may be related to the surgical experience of senior surgeons, which we know to be better, and the associated lower intraoperative blood loss. In addition, it shows that the management of complications related to intraoperative bleeding may have been better achieved by senior surgeons, who again have more experience. However, although the duration of the operation was longer, we found that these negative results were not significantly reflected in the clinical results in the postoperative period. Indeed, postoperative hepatic and renal disorders are known to be important complications after CPB [19]. However, although we found differences in CPB and XCL times between the groups, we did not find differences in laboratory parameters on the first day and at 1 month postoperatively, as seen in Table III. These results also show that the junior and senior surgeon groups have comparable results in terms of noncardiac effects such as renal and hepatic systems after CABG. This detailed comparison we made in terms of laboratory parameters also yields important results, unlike other studies.
Table IV shows the comparison of postoperative outcomes between junior and senior surgeon groups, and we did not find any difference except in need for ECMO. Although comorbidities were generally similar, we conducted a subgroup analysis again because we thought that patients receiving dual antiplatelet therapy had a higher risk of bleeding and this could have affected the results. According to the new analysis, as can be seen in Figure 1, we did not find any statistically significant difference between junior and the senior surgeon group in terms of all postoperative outcomes (postoperative exploration, CVA, need for CRRT, POAF, SSWI, DSWI, gastrointestinal bleeding, PCI, pleural effusion, need for IABP, need for ECMO, tracheostomy, intubation time, ICU stay, hospital stay, total mortality, early mortality, and late mortality). Although XCL and CPB times, which are the basic indicators of operative time, were longer in the junior surgeon group, we believe that postoperative outcomes were at an acceptable level compared to the senior surgeon group. Similar postoperative outcomes were found in the study by Oo et al. comparing trainees and consultants [9]. In the study by Stoica et al., no difference was found except for prolonged ventilation [11]. Similarly, no difference was found in terms of early postoperative outcomes in the comparison of AVR and CABG patients by Saxena et al. [10]. However, one of the most important differences of this study is that in the junior group, some distal anastomoses were not performed. The entire operation was performed skin-to-skin by junior surgeons. Junior surgeons perform all the postoperative follow-up and take full responsibility for the patient. In addition, the most important difference is that no patient assignment was made to junior surgeons and no patient selection was made in their favor. The number of patients and patient characteristics were balanced between the groups. Even though we believe it was by chance and it was not statistically significant, EuroSCORE II was higher in the junior group than in the senior group. In the junior group, EF was between 30 and 50% in 60 (25%) patients and between 20 and 30% in 11 (4.6%) patients. Although the difference was not significant, junior surgeons performed more emergency operations (14 (5.8%)).
In addition, while the preoperative mean EuroSCORE II mortality score was 2.6% in the junior surgeon group, the total mortality was 3.3% at the end of the study. In the senior surgeon group, the preoperative mean EuroSCORE II mortality score was 2.1%, while it was 2.3% at the end of the study. We can say that these results are also within acceptable limits for junior surgeons. However, it should not be forgotten that EuroSCORE II shows the general risk status of patients and does not include many factors, such as the severity of coronary artery disease. The coronary endarterectomy rate in the senior group was significantly higher than in the junior group in our study. Since we could not make a comparison in terms of the severity of coronary artery disease, drawing definitive conclusions on this aspect is difficult. This situation may have occurred by chance. Alternatively, it may have arisen because, in patients with very critical coronary artery disease, senior surgeons tend to perform more coronary endarterectomies due to their better experience, as expected, while junior surgeons consider these anastomoses inoperable. Even among senior surgeons, there may be different opinions in clinical practice. Future studies are needed to determine which vessel should or should not be anastomosed.
The purpose of this study was not to determine whether junior or senior surgeons achieve better results. The results of this study suggest that junior surgeons can perform less complex CABG procedures with acceptable complication rates under good training and control. This study provides important findings in terms of assuring patients that junior surgeons can perform their operations. There will be no surgeons of the future without training. Although health services prioritize patient benefit and safety, it is important to distribute time and economic resources equally to both education and health services. Since even the best surgeon cannot perform operations indefinitely, it is our responsibility to safeguard not only current outcomes but also future practice.
First, the most important limitation of this study is that it is retrospective and single-centered. Second, our clinic is newly established and has a heterogeneous group consisting of many junior and senior surgeons who received training from different centers. The results may vary in different centers with different training levels. Therefore, conducting multicenter studies in the future may yield more reliable results. Third, only isolated CABG operations were included. Although the most frequently performed procedure, CABG, was evaluated, it would be useful to investigate this issue in cases such as valve operations and aortic surgery. Fourth, as in many other studies, since routine coronary angiographic follow-up was not performed after CABG, the evaluation of graft patency was insufficient except for clinical findings. In addition, since transit time flow measurement is not routinely available, a comparison could not be made. Additionally, the status of the assistant surgeon, whether junior or senior, may influence postoperative outcomes. However, this factor was not compared in the current study. It would be beneficial to include this comparison in future studies. Finally, although we defined junior and senior surgeons based on 10 years of active cardiac surgery, different results might be obtained if this limit were lowered to 5 years or less. However, despite some limitations, this study also produced important results. In particular, it evaluated the adequacy of the 5-year resident training in Turkey and demonstrated that junior surgeons have comparable results to senior surgeons in a balanced study group of all patients, including emergency procedures, without patient selection.
Conclusions
The results of this study showed that junior surgeons had acceptable postoperative early outcomes that were comparable to senior surgeons in isolated, less complex CABG patients. Although junior surgeons had longer XCL and CPB times, we did not find any significant differences in clinical outcomes. Junior surgeons in the early stages of their careers can safely perform CABG procedures.









