
Purpose
The incidence of skin cancer has been increasing over the past few decades [1], with non-melanoma skin cancers or keratinocyte carcinomas constituting majority (95%) [1]. Basal cell carcinoma (BCC) is the most frequent form of non-melanoma skin cancer (NMSC), comprising 75% of all skin cancers. Squamous cell carcinoma (SCC), although a less frequent type of cancer, is more aggressive. The standardized ratio of BCC to SCC is approximately 4 : 1.2 [2, 3]. With the increasing incidence, a robust evidence base is essential for informed treatment decisions. The overall age-adjusted rate (AAR) of NMSC in India is 6.2 in males and 3.49 in females [4].
Early-stage NMSC is usually managed by one of the following methods: surgical excision, electrodesiccation and curettage, cryosurgery, radiotherapy, photodynamic therapy, and even pharmacological agents (i.e., imiquimod) [5, 6], with Mohs micrographic surgery regarded as the best option [7]. The goal of treatment is to eradicate the tumor while maximizing cosmetic and functional outcomes. The highest overall cure rates with excellent cosmesis are achieved with Mohs micrographic surgery [7]. This practice is nowadays considered the therapeutic gold standard for all NMSCs. However, surgery may occasionally result in significant cosmetic disfigurement and functional impairment, thus in selected patients, alternative treatment modalities may be preferred.
Furthermore, the widespread application of specific approaches is limited by the lack of specialized infrastructure and trained personnel. Radiation therapy is an option to consider for patients who are not candidates for surgical procedures, or for tumors located in areas of high-risk of poor cosmetic results after surgery (i.e., pinna, nose) [8]. Radiation can also be used as an adjuvant; when delivered correctly, radiation therapy achieves tumor control rates above 90% in both BCC and SCC.
Various radiotherapy modalities and techniques have been employed to treat NMSC, with acceptable local control outcomes [9-13]. Both external beam radiotherapy and brachytherapy have been used historically for cutaneous malignancies with good clinical outcomes. Brachytherapy is often preferred for superficial skin cancers due to its sharper dose fall-off, and is most commonly delivered via shielded applicators or surface moulds (plesiotherapy). Although these techniques achieve tumoral control rates similar to those of external radiotherapy, due to frequent using of hypofractionation, concern about long-term cosmesis persists [9-13]. Herein, we presented the long-term results of control and cosmesis using customized surface mould brachytherapy in the treatment of NMSC, along with an effort to identify the factors affecting these outcomes. Ethical clearance was obtained from the Institutional Ethics Committee for this project.
Material and methods
Patient selection
Patients visiting our outpatient department from January 2012 to December 2019 were included in the study. Inclusion criteria were localized, biopsy-proven non-melanoma skin cancer, and meeting one of the following criteria: post-operative cases with an indication for adjuvant radiotherapy (positive or close surgical margins, T4 primary tumor, perineural invasion, recurrent disease, or multiple high-risk features, such as lymphovascular invasion, depth of invasion > 6 mm, tumor size > 4 cm, and high-grade histology), or patients who were unfit, unsuitable, or unwilling to undergo surgery [14-18]. Only patients with an ECOG performance status ≤ 2 were included. Criteria for surgical unsuitability were determined jointly by a plastic surgeon and a radiation oncologist, depending on age, site, prior treatment, comorbidities, and patient preference. Exclusion criteria were metastatic disease at presentation, previous radiotherapy to the same anatomical region, multiple primary synchronous lesions, and incomplete clinical and pathological workup. Written informed consent was obtained from all study participants.
Mould preparation, treatment planning, and delivery
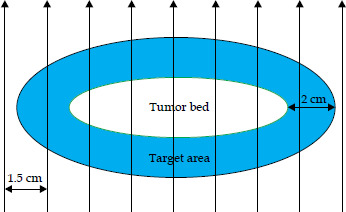
An area of interest (post-operative bed/clinico-radiological skin lesion) was marked with a marker for reference after antiseptic shaving/ cleaning if required. An additional 1.5-2 cm of skin was considered around the area of interest for clinical target determination. Thermoplastic mask was prepared, and an impression of the skin-marked clinical target was made on the mask above the area of interest. Surface mould was prepared by melting layers of wax in a 70°C water bath and applying them over clinical target (area of interest + margin) to achieve a thickness of 0.5-1 cm, based on the patient’s surface contour. Grooves were made on the wax mould at 1 to 1.5 cm intervals to accommodate plastic catheters along the length, thereby reducing the number of catheters required. Plastic catheters were placed in the grooves, and additional wax was molded onto them to prepare the final mould with a thickness of 1.5-2 cm (Figure 1, representative Figure 2).

Computed tomography (CT) simulation was performed with the mould in place, and the clinical target was marked with a lead wire to demarcate the area on the CT scan easily. A non-contrast scan was obtained using 2.5 mm cuts. For radical treatment, the clinical target volume (CTV) depth was determined by the visible tumor. For adjuvant treatment, CTV included the post-operative bed and the region within the skin markers. The depth of adjuvant CTV depended on the initial tumor depth, extent of dissection, and post-operative CT changes. A 2 mm margin was added to CTV to account for inter-fraction variability. Skin, mould, and underlying bone were contoured separately.
For treatment planning, dose points were created around the catheters, and prescription dose was determined. After reconstruction of catheters and source dwell positions, TG-43-compliant BrachyVision (Varian Medical Systems, Palo Alto, USA) was used to create a treatment plan. Following this, volumetric optimization was performed to ensure that 100% prescription isodose conformally covered the target volume. Care was taken to reduce the volume of target covered by a 150% isodose curve. The total prescribed dose was 3,500-4,200 cGy, delivered in twice-daily fractions of 300-450 cGy each, with at least 6 hours interval between fractions, in nine to twelve fractions. Dose homogeneity index (HI) inside planning target volume (PTV), conformity index (CI), and minimum doses to the most exposed 0.1 cc, 1 cc, and 2 cc (D0.1cc, D1cc, D2cc) of organs at risk (OARs) for brachytherapy (BT) plans were assessed.
Following completion of treatment, patients were followed up at four weeks and thereafter at monthly intervals for the first three months, at three-month intervals for the first two years, and thereafter every six months. Patients were assessed clinically for local recurrence, toxicity, regional nodal failure, and cosmetic outcome. Acute and late toxicity were graded according to the Radiation Therapy Oncology Group (RTOG) toxicity scale (Supplementary Table 1) [19].
Study technique, data collection, and analysis
Patients’ characteristics, tumor, and surgical data were collected from medical records using a structured checklist. Mould, target characteristics, and dosimetric data were recorded from the BrachyVision treatment planning system, including target volume, individual inter-catheter separation (mm), average depth of PTV (h in mm), average distance between the midpoint of catheter and skin surface (H in mm), average distance between the midpoint of catheter and deepest point of PTV perpendicular to the catheter (R = H + h, in mm), 0.1 cc, 1 cc, and 2 cc skin dose, and HI. The highest grade of acute skin toxicity was noted from the beginning of treatment up to the first 3 months of follow-up. The highest grade of late toxicity was observed from 3 months post-treatment throughout the follow-up period.
All categorical and continuous data were tabulated and analyzed using the statistical package for the social sciences (SPSS) version 23.0. Categorical data were tabulated using descriptive statistics. Toxicity and cosmetic outcome were compared with dosimetry and mould parameters using independent sample t-test. Binary mould parameters were compared with toxicity profile using chi-squared or Fisher’s exact tests. Since no failures were observed during the follow-up period, no survival analysis was performed. Given the exploratory nature of the study and small sample size, no correction for multiple comparisons was applied.
Definitions
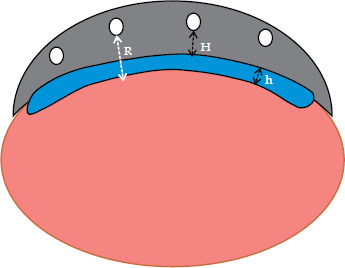
Vx% (V100%, V150%) – volume of the target volume receiving at least x% dose; Dx (D0.1cc, D1cc, D2cc) – minimum dose received by maximally irradiated x% volume; Homogeneity index (HI) – (V100-V150)/V100; Mould dimensions (R, H, and h, Figure 3): H – average distance between the midpoint of catheter and the skin surface; h – average depth of PTV; R – H + h.
Fig. 3
Illustrative demonstration of the cross-section area of a mould over the target showing various dimensions used in the study: Pink region – normal tissue, Blue region – PTV, Grey region – custom surface mould on PTV, H – average distance between the midpoint of catheter and skin surface, h – average depth of PTV, R – H + h
Cosmetic outcome grading
Cosmetic outcome grading was based on physician-reported RTOG and European Organization for Research and Treatment of Cancer (EORTC) late radiation morbidity scheme for evaluation of cosmetic outcomes, by reporting them as excellent, good, fair, or poor [19]: Excellent – no changes to slight atrophy, pigment change, some hair loss, slight induration, and loss of subcutaneous fat; Good – patch atrophy, moderate telangiectasia, total hair loss, moderate but asymptomatic fibrosis, and slight field contracture with less than 10% of linear reduction; Fair – significant post-radiation changes, marked atrophy, gross telangiectasia, severe induration or loss of subcutaneous tissue, and field contracture greater than 10% of linear measurement; Poor – severe post-radiation sequelae and ulceration or necrosis.
Results
After meeting the inclusion and exclusion criteria, twenty-eight patients were included in the study. The baseline patient and tumor characteristics are presented in Table 1. The median age was 54.5 years (range, 43-78 years). Most patients were males (17/28, 60.7%), 19 (67.9%) patients had SCC, and 8 (28.6%) patients were treated with radical intent. The most common location was the nose and nasal bridge. The area of lesion/tumor bed was less than 20 cm2 in 13 (46.4%) patients, while it was more than 40 cm2 in 6 (21.4%) cases.
Table 1
Patient, target, and mould characteristics of the study population
The dose volume and mould characteristics are defined in Table 2. The mean inter-catheter distance was 11.18 mm, and the mean PTV depth was 4.61 mm. The highest PTV depth was 9.8 mm. Seven patients (25%) had a PTV depth > 5 mm. The mean V100 was 95.4% (range, 92.6-98%), and all patients received a 100% dose in at least 90% of PTV. Ten (35.7%) patients had a HI of less than 0.80.
Table 2
Mould, dimension, and dosimetric characteristics of the target
Table 3 shows the toxicity profile and cosmetic outcomes of the study population. Acute skin toxicity was predominantly grade 1-2, with 50% experiencing grade 1 and 46.4% grade 2 toxicity. Among late toxicity, 21.4% (n = 6) and 28.6% (n = 8) had grade 2 late skin and subcutaneous toxicities, respectively. Among grade 3 toxicity, only 1 grade 3 acute skin toxicity was noted. Favorable cosmetic outcomes were reported, with 67.9% and 32.1% of patients showing excellent and good cosmetic outcomes, respectively (100% total).
Table 3
Toxicity profile of the study group
| Parameter | Grade 1 | Grade 2 | Grade 3 |
|---|---|---|---|
| Acute skin toxicity | 14 (50.0%) | 13 (46.4%) | 1 (3.6%) |
| Late skin toxicity | 22 (78.6%) | 6 (21.4%) | 0 |
| Late subcutaneous toxicity | 20 (71.4%) | 8 (28.6%) | 0 |
The 0.1 cc, 1 cc, 2 cc skin dose, and HI were significant predictors of late skin toxicity and subcutaneous toxicity (Tables 4, 5). PTV depth > 5 mm and tumor bed surface area of more than 40 cm2 predicted a growing trend towards increased late toxicity; however, the association was not significant (for the surface area > 40 cm2, 30.8% vs. 13.3% late grade 2 skin toxicity, and 38.5% vs. 20% late grade 2 subcutaneous toxicity). For cosmetic outcomes (Table 6), along with the 0.1 cc skin, 1 cc skin, 2 cc skin, HI, the average distance between the catheter midpoint and the skin surface (H) was a significant predictor of cosmetic outcome (p = 0.03). Patients with H < 7 mm had a higher incidence of grade ≥ 2 late toxicity compared with those with H ≥ 7 mm (44.4% vs. 10%, p = 0.07, Fisher’s exact test). After a median follow-up of 54 months (range, 36-144 months), no disease recurrence was reported among the study population.
Table 4
Comparison of late skin toxicity outcomes with mould, target dimension, and dosimetry parameters
Table 5
Comparison of late subcutaneous toxicity outcomes with mould, target dimension, and dosimetry parameters
Table 6
Comparison of cosmetic outcomes with mould, target dimension, and dosimetric parameters
Discussion
The incidence of NMSC has been rising over the past decade, thus warranting early diagnosis and prompt treatment. These lesions, especially on the skin, are usually diagnosed at an early stage, because patients present to clinicians early. The challenge in treating the tumor is achieving a good cosmetic outcome without compromising local control. While surgery remains the treatment of choice for skin cancer, alternative treatments have been traditionally considered for selected cases, such as tumors at locations with high-risk of poor aesthetic results (i.e., nose, eyelids), or for patients not amenable to surgical procedure due to age or presence of comorbidities [9-11, 13, 20]. Superficial radiotherapy using brachytherapy moulds or devices (plesiotherapy) has been explored since the earliest days of radiation treatment [21, 22]. However, its popularity soon decreased due to concerns about radioprotection against radium or radon sources available at the time [23, 24]. The rapid development of orthovoltage technologies followed by linear accelerators, which offer a wide range of electron energies, also contributed to declined use of plesiotherapy [25]. In recent years, the accessibility to afterloading HDR equipment, which overcomes radiation exposure, has renewed the interest in using brachytherapy for treating both primary and metastatic cancer of the skin. Plesiotherapy with tailored moulds offers several advantages in the treatment of superficial skin tumors [26-30]. A custom-made mould allows precise placement of irradiation source close to the tumor, ensuring that the treatment isodoses match the exact shape of the surface to be treated. Dose distributions in HDR brachytherapy seem at least similar to those obtained with electrons, although doses delivered to subcutaneous tissues, including bone, are reduced.
Numerous organizations have published guidelines for skin brachytherapy in both definitive and adjuvant settings [14-17]. Different applicators and modalities were used, including pre-defined applicators, such as Valencia and Leipzig (Nucletron, Elektra AB, Stockholm, Sweden), electronic brachytherapy devices, and customized moulds. One of the advantages of customized moulds over other techniques is their ability to be tailored for irregular surfaces, applied to large surface areas, and used in resource-limited settings [27, 28].
Our experience with plesiotherapy in the treatment of skin cancers is consistent with that reported in the literature. Rates of complete response after treatment and local control after follow-up are in line with those from series involving more patients. Although acute reactions occurred in nearly all our patients, they were mild to moderate in intensity. Additionally, no patient needed a rest period to recover from toxicity, preventing detrimental interruptions during radiation treatment.
In our study, no local recurrences were observed during the median follow-up of 54 months. Casey et al. reported overall local control as 80-100% in the literature [31], whereas individual studies showed local control rates of 84.4% to 98% after a median follow-up of 8-66 months [27, 31-34]. Gauden et al., with a sample size of 236 patients and a median follow-up of 66 months, demonstrated 98% of local control and only 4 local recurrences [32]. An Italian study reported that 85% of patients treated with radical radiotherapy achieved 90% of local control at 2 years [34]. Overall, comparable local control rates have been reported in all studies with both radical and adjuvant treatment intent.
Various dose-fractionation schemes have been presented in the literature, along with prescription depth [14, 16-18]. In most studies, prescribed doses were 3-5 mm below the skin, while limited research targeted CTV with prescription isodose. Almost all studies preferred hypofractionated treatment, with standard fraction sizes of 2-4 Gy used in most papers [31, 32]. However, some research used large fraction sizes of 6-7 Gy per fraction [33, 35], including Tormo et al. who employed a large dose per fraction prescribed at 4 mm depth, using Valencia applicator [33]. The American Brachytherapy Society has recommended doses of 40 Gy in 10 fractions and 42 Gy in 6 fractions for custom-made moulds [14].
Majority of studies have reported favorable toxicity profiles for surface mould brachytherapy in NMSC; the most common toxicity was late radiation dermatitis, with rare grade 3-4 toxicity observed [27, 31-37]. Gauden et al. [32] revealed 71% of grade 1 skin toxicity, and Casey et al. [31] dermatitis grade 1 and 2 (58% and 32%, respectively). A report by the Greater Poland Cancer Centre for HDR brachytherapy in skin cancer reported grade 3 acute and late skin toxicity as 8.9% and 4.9%, respectively [36]. However, this study used a relatively large dose per fraction (50-60 Gy/10 fractions or 30-40 Gy/6-8 fractions), and a larger depth of prescription of 1 cm. Arenas et al. observed acute grade 3 and 4 toxicity at 40.3% and 2.2%, respectively, and late grade 3 and grade 4 toxicity as 4% and 0.8%, respectively [37]. In the current study, only 1 case of grade 3 acute skin toxicity was observed with no grade 3 late toxicity, even within 25% of patients having a PTV depth of more than 5 mm and relatively high mean small-volume doses to the skin (0.1 cc, 1 cc, and 2 cc).
Excellent or good cosmetic outcomes were achieved in all patients. Overall, excellent to good cosmetic outcomes have been reported in 69-98% of the literature [6]. A meta-analysis with 21,000 patients showed that brachytherapy and MMS result in better cosmetic outcomes than external beam radiotherapy (EBRT) and standard excision [38]. Here, 0.1 cc, 1 cc, and 2 cc skin doses, and homogeneity index, significantly predicted late skin and subcutaneous toxicity and cosmetic outcome. Arenas et al. observed greater grade 3-4 toxicity with custom moulds compared with Leipzig applicators, probably due to a larger treatment surface area with custom moulds [37]. CTV V100, V150, and V200 are predictors of late skin toxicity in the literature [35, 39]. The distance of applicator catheters from the skin surface was demonstrated to cause greater skin toxicity, as catheters very close to the skin create more hot spots [6]. Total radiation dose, treatment volume, and using manufactured flaps have been shown as determinants of acute grade 3 toxicity in the literature [40]. In our study, patients with grade 2 toxicity and a less-than-excellent cosmetic outcome had a shorter mean distance between the catheter and the skin surface; however, this difference was significant only for cosmetic outcome (p = 0.03).
Our study is unique in that no recurrences were observed during the follow-up period, even among patients with considerable PTV depth (> 5 mm) and a large treatment area (25% with surface area > 70 cm2). We also demonstrated a correlation between small volume skin dose parameters and toxicity, an area that remains relatively underexplored in the existing literature.
Although various radiotherapy techniques demonstrated comparable local control with acceptable toxicity profiles, external beam radiotherapy using photons or electrons remains the most widely employed modality. However, the implementation of customized surface mould brachytherapy requires dedicated training, meticulous planning, and experienced multidisciplinary coordination, including skilled radiation oncologists, medical physicists, and technicians. Consequently, this modality is predominantly practiced in centers with established institutional expertise. Broader adoption of surface mould brachytherapy may be facilitated by structured training programs, standardized protocols, and collaborative knowledge-sharing among peer institutions, enabling its safe and effective integration into routine clinical practice.
Recent advances in three-dimensional (3D) printing expanded the scope of individualized surface mould brachytherapy. CT-based applicator design integrated with treatment planning systems, enables precise catheter geometry and improved conformity to irregular anatomical surfaces, thereby reducing air gaps [41]. Dosimetric investigations demonstrated good agreement between planned and delivered dose distributions using polylactic acid-based applicators, with reproducible positioning and acceptable organ at risk doses [42]. Early clinical implementation in small patient series further reported complete local responses with manageable acute toxicity profiles assessed using RTOG criteria [43]. These developments suggest that 3D-printed applicators represent a practical and promising evolution of customized skin brachytherapy, particularly in anatomically challenging sites.
Conclusions
Surface mould brachytherapy can provide excellent local control and cosmetic outcome for the treatment of non-melanoma skin cancer in both adjuvant and definitive settings. While local control is excellent, cosmesis is often an issue. However, careful selection of the depth of wax bolus and keeping small volume doses within pre-defined limits may help reduce long-term skin toxicity and improve cosmesis.








