
INTRODUCTION
The differential diagnosis of Alzheimer’s disease dementia (AD), vascular dementia (VaD), and mixed dementia (MD) remains a significant challenge in both clinical practice and research [1]. Differentiating MD characterised by both Alzheimer’s and vascular patho-logy from pure vascular dementia is clinically relevant, as the presence of Alzheimer-type pathology may justify cholinesterase inhibitor or memantine treatment, which are not recommended for pure vascular dementia. While AD is the most common cause of dementia worldwide, cerebrovascular pathology is also highly prevalent in aging populations and often coexists with neurodegenerative changes. Neuropathological studies consistently show that many older adults with cognitive impairment = exhibit both Alzheimer-type pathology and vascular brain injury, highlighting the clinical importance of MD [2], which is sometimes considered the most frequent aetiology of dementia. However, in clinical practice, the majority of patients in the early stages of dementia are diagnosed with AD, followed by MD, with pure VaD proving relatively rare [3]. Another explanation for the classification of VaD as the second most common cause of dementia stems from the Vascular Impairment of Cognition Classification Consensus Study, which incorporates MD – along with subcortical ischemic vascular dementia, post-stroke dementia, and multi-infarct dementia – into four phenotypic subgroups of vascular cognitive impairment and dementia [4].
According to current diagnostic criteria, the evalua-tion of dementia requires the examination of a combination of medical history, informant reports, and standardized cognitive testing, complemented by additional procedures, such as neurological and psychiatric examination, neuroimaging, and laboratory testing [5]. The differential diagnosis is further complicated by the fact that many risk factors for VaD, including a history of stroke, low educational attainment, lifestyle factors (e.g., poor diet, low physical activity), psychological factors (e.g., depression, sleep disorders), substance use (smoking, alcohol abuse), and medical conditions such as cardiovascular disease and diabetes, substantially overlap with risk factors for AD – with the notable exception of stroke history [6, 7].
Cognitive assessment, mainly neuropsychological evaluation, is helpful, as distinct profiles characterize different types of dementia. Classically, AD features a progressive amnestic syndrome, with early impairment in episodic memory due to involvement of the medial temporal lobe, followed by a decline in language, visuo-spatial processing, and executive functions [5], often accompanied by apathy. In contrast, VaD is typically associated with cognitive slowing, attentional deficits, reduced working memory, and dysexecutive symptoms that reflect subcortical-frontal disconnection. Language and episodic memory deficits in VaD vary across subtypes; for instance, subcortical VaD typically causes executive and retrieval problems, whereas cortical or strategic infarct VaD may produce aphasic or language-dominant profiles comparable to AD [8]. However, the distinction diminishes in advanced stages. In addition to the pre-sence of cerebrovascular events, vascular neurocognitive disorder is usually differentiated from other neurocognitive disorders by early motor and mood changes (emotional lability) [9]. Importantly, mixed dementia frequently presents with overlapping impairment patterns, in which vascular lesions exacerbate AD-related deficits or accelerate decline across multiple domains [10]. These clinical realities blur the diagnostic boundaries, reducing the reliability of syndromic criteria alone [11]. Neuropsychological services are often limited, may involve long waiting times, or require private funding, as they provide highly specialized diagnostics. These factors can delay both diagnosis and subsequent treatment [12]. Cognitive screening may offer a partial solution. Although various screening methods exist, not all have demonstrated sufficient diagnostic utility for differentiating dementia subtypes.
As mentioned above, executive dysfunction is a well- established impairment in VaD, typically accompanied by relatively preserved memory. In contrast, AD typically presents the opposite pattern, characterized by poor memory but preserved executive functions. Therefore, clinicians should prioritize assessment tools that evaluate these specific cognitive domains. According to the review by Tomaszewska et al. [13], only a few screening scales adequately assess executive functions and are designed for general use, including in particular Addenbrooke’s Cognitive Examination III (ACE-III) [14] and Montreal Cognitive Assessment (MoCA) [15]. The Mini- Mental State Examination (MMSE) [16] shows limited sensitivity in detecting the deficits associated with vascular changes [9].
Some studies have evaluated the role of the MoCA in differentiating between various types of dementia, and the results suggest its total scores and subscores can be valuable in differential diagnosis [17-19]. However, the current study has revealed that the MoCA indeed helps differentiate between patient populations with different dementia aetiologies, except for VaD [20].
Recent work by Carrick et al. [21] highlights the fact that ACE-III is sensitive to cognitive changes across a broad range of severities in typical and atypical dementia presentations. Due to its multidomain structure – encompassing Attention, Memory, Fluency, Language, and Visuospatial abilities – the ACE-III also provides opportunities for qualitative analysis that may support differential diagnosis [22].
Evidence for the utility of the ACE-III in differen-tiating MD from VaD remains scarce, as VaD groups examined to date are typically smaller than other dementia cohorts, highlighting the need for further research with larger samples [23-25].
The present study has compared three dementia groups to evaluate the diagnostic value of the ACE-III in distinguishing between dementia subtypes.
Methods
Participants
The study included data extracted from a fully anonymized research database, ensuring participants’ confidentiality and compliance with ethical standards. From this dataset, 138 Caucasian native Polish patients, diagnosed with mild-stage AD, VaD, or MD were selected for further analysis. Due to the limited number of patients with VaD, this group served as a reference population. Each group consisted of 46 patients (21 women and 25 men), matched for sex, education, and age to participants with VaD, encompassing both early- and late-onset forms of the disease.
According to current diagnostic criteria, the evalua-tion of dementia requires an assessment of medical history, informant reports, clinical interview, and standardized cognitive testing. Diagnostic classification was based on established clinical criteria [5, 26] and neuroimaging pathology (as described in computed tomography or magnetic resonance imaging). The clinical profile and severity of dementia were confirmed by standard neuropsychological testing (a detailed description has been published previously) [27], with ACE-III as a routine part of cognitive evaluation. Patients with atypical AD variants, severe somatic/psychiatric conditions, and those with incomplete or invalid test data were rigorously excluded, ensuring the study’s integrity. All assessments were conducted by the same examiner (A.B.).
This study is a retrospective analysis of fully anonymized data, ensuring participants’ confidentiality and compliance with ethical standards.
Procedure and measures
The ACE-III Polish version (2014) was used in the study (https://www.sydney.edu.au/brain-mind/resources- for-clinicians/dementia-test.html). The total maximum score is 100, a sum of the following domain scores: Attention: 0-18, Memory: 0-26, Fluency: 0-14, Language: 0-26, and Visuospatial: 0-16. In this study, the total score and domain subscores were analyzed, as along with single tasks within the domains.
Data analysis
Statistical analyses were carried out using JASP (Version 0.95; JASP Team, 2025) [28], a software package that is free, reliable and widely used in psychological research. Descriptive statistics were computed for all variables. Group differences in categorical variables were assessed using the c2 test of independence. Normality was tested with the Shapiro-Wilk test and homogeneity of variances with Levene’s test, both indicating violations of parametric assumptions (all p < 0.05). Therefore, nonparametric tests were applied. Post-hoc pairwise comparisons were conducted using Dunn’s test with Bonferroni correction (Dunn-Bonferroni method) to adjust for multiple comparisons following significant Kruskal-Wallis results. In addition to significance testing, effect sizes were calculated to estimate the strength of group differences. For pairwise comparisons, the effect size r was computed as Z/√N, where Z is the standardized test statistic from the Mann- Whitney or Dunn-Bonferroni test, and N is the total number of participants across both groups. According to Cohen’s (1988) guidelines [29], r values of approximately 0.10, 0.30, and 0.50 correspond to small, moderate, and large effects, respectively. Effect sizes are reported for significant and near-significant contrasts to facilitate interpretation of the magnitude of group differences. Adjusted p-values are reported for each contrast (VaD vs. AD, VaD vs. MD, and MD vs. AD). Where applicable, exact p-values are presented; values exceeding the significance threshold are reported as non-significant (n.s.).
Results
The three groups did not differ in demographic charac-teristics. Gender distribution was identical (21 females, 25 males in each group). No significant differences were observed for age or years of education (see Table 1). Since all groups included both early- and late-onset patients, we compared the total ACE-III scores across the clinical populations. No significant group differences were observed between patients below and over 65 years of age (VaD: H = 2.43, p = 0.12; MD: H = 2.63, p = 0.104; AD: H = 0.16, p = 0.69).
Table 1
Demographic characteristics of studied groups with means, median and interquartile range (IQR) values
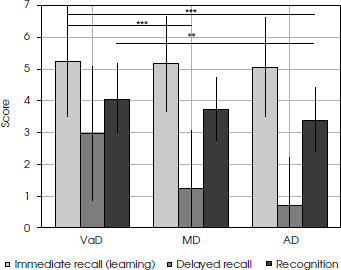
Total ACE-III scores did not distinguish between the studied populations. See Table 2 for details. A significant group effect was found only in the Memory domain (p < 0.001). Post hoc comparisons showed that VaD patients performed significantly better than both MD (p < 0.001) and AD (p = 0.005) patients, whereas no difference was observed between MD and AD patients. At the subtest level, no group differences were found for Name and Address or Famous People. In the Recall of 3 Items task, VaD patients outperformed both MD (r = 0.22) and AD (r = 0.22), but the effect was small. The Recall Name and Address task showed the most significant difference between VaD (mean 2.96) and the rest of the clinical populations, with moderate (MD; mean score 2.00, r = 0.39) or large effect (AD; mean score 0.67, r = 0.51; both p < 0.001). In the Recognition of Name and Address task, VaD patients also scored significantly higher than AD patients with a moderate effect (p = 0.003, r = 0.30), but similarly to the MD group. Patients with AD and MD had similar results across the Memory domain (see Table 2). Figure I illustrates performance in immediate and delayed recall, and recognition of Name and Address task across all groups.
Figure I
Name and Address immediate recall, Delayed Recall of Name and Address, and Recognition of Name and Address performance in participants with vascular dementia (VaD), mixed dementia (MD), and Alzheimer’s disease (AD)
Within the Attention domain, only the Serial 7 Subtraction task revealed a significant group effect (see Table 2). Post hoc analyses indicated that AD patients performed significantly better than VaD patients, with a moderate effect size (p = 0.006, r = 0.28). No significant differences were found between VaD and MD or between AD and MD. The remaining tasks (Time and Orientation, Registration of 3 Items) did not differentiate between the groups.
For the Fluency domain, no overall group effect was observed. However, the Letter Fluency (K), post hoc comparisons showed that VaD patients obtained lower scores than AD patients (mean scores: 3.5 vs. 4.3), but with a small effect (r = 0.18). Compared to either VaD or AD, MD patients performed in between, without significant differences. The category Fluency (Animals) did not reveal significant differences. Table 2 presents all details. The Language domain showed no significant group differences in either the total domain score or the individual subtests (see Table 2). Within the Visuospatial domain, although there was no effect across all populations, only the Counting Dots task showed significant group diffe-rences. AD patients performed best, while VaD patients performed worst. Post hoc comparisons confirmed that VaD scored significantly lower than AD, with a moderate effect (p < 0.001, r = 0.28), and that AD also outperformed MD, with a small effect (p = 0.005, r = 0.21). No significant differences were found between VaD and MD. Other visuospatial tasks (Intersecting Infinity Loops, 3D Wire Cube, Clock, Identifying Letters) did not differentiate the groups (see Table 2).
Table 2
ACE-III domains and subtest performance in patients with vascular dementia (VaD), mixed dementia (MD), and Alzheimer’s disease (AD)
Discussion
In this study, we compared cognitive performance across VaD, MD, and AD using the ACE-III. The demographic factors such as age, education, and sex were well-matched across groups. As previously mentioned, due to the limited number of patients with VaD, this group served as the reference to which the other clinical populations were matched for demographics. Although after AD, VaD is traditionally considered the second most common cause of dementia, several studies have highlighted that mixed pathology is more frequent than isolated VaD, particularly in older populations [30], and our study design reflects this finding.
Our populations included both early- and late-onset patients, yet we did not observe significant differences related to age of onset. Whether and how these subgroups of various age of onset differ remains unclear [1, 31]. Nevertheless, even with some differences, the overall cli-nical profile of early- and late-onset cases appeared similar.
As expected, and consistently with previous reports total ACE-III scores did not differentiate between the dementia groups [24, 32]. Although the ACE-III has been shown to outperform other screening methods in the early detection of cognitive impairment [33] and in staging dementia severity [34], our findings reinforce the limitation of total scores; when distinct clinical popu-lations are compared, total scores often remain similar if impairment severity is matched across groups [24, 34]. An extensive population study by Potts et al. [24] reported that AD patients had higher median total ACE-III scores than MD and VaD patients. However, our findings differed: the total ACE-III score fell between the median scores for VaD (the highest) and MD (the lowest). All the differences were minimal. Notably, previous research has shown that demographic adjustments may further reduce the discriminative power of screening methods. Piccininni et al. [35] demonstrated that correcting for age and education can lower diagnostic accuracy, suggesting that excessive adjustment may obscure clinically meaningful differences. It underscores the importance of domain-level interpretation rather than sole reliance on global scores. By design, the ACE-III allows analysis of cognitive domains, and as suggested by Sitek et al. [22], qualitative analysis within domains may support diffe-rential diagnosis.
Potts et al. [24] reported that AD patients scored highest in the Fluency, Visuospatial, and Language domains compared with MD and VaD groups. However, it is only partially consistent with our findings, as, in gene-ral, Fluency and Visuospatial domains scores were significantly better in AD patients than in the other groups. However, in our cohort, AD patients obtained the lowest language scores, albeit the difference was minimal. While published reports found significant differences between AD and VaD in Visuospatial and Language domains [24], we were unable to replicate these findings, nor did we observe differences between AD and MD populations. It is worth noting that patients in the cohort mentioned above were, on average, about a decade older than those in our study, included more women, and although similarly well-educated, were more severely impaired, as indicated by ACE-III total scores approximately 10 points lower than those of our population.
In our study, significant differences emerged only in the Memory domain, where VaD patients performed significantly better than both AD and MD patients, while AD and MD showed comparable performance. This finding is consistent with observations that, despite frequent subjective memory complaints from patients and informants, episodic memory is relatively spared in VaD even in patients already diagnosed with mild dementia [9]. It underscores the need for objective cognitive assessment, as emphasized in diagnostic guidelines, to address the discrepancy between subjective complaints and test performance [36]. Interestingly, the Memory domain in the ACE-III includes both retrograde and anterograde components, and detailed subtest-level analysis revealed new insights. The only significant group differences were observed in episodic (anterograde) memory tasks (Recall of 3 Items, Name and Address Recall, and Recognition). As expected, AD patients scored lowest, and VaD patients scored highest. These results reinforce the view that episodic memory impairment is the hallmark of AD, while patients with mild VaD show much less involvement of this function [37]. This supports the discriminatory utility of the ACE-III in differential diagnosis, particularly in distinguishing AD-related pathology from VaD. As expected, MD patients were more similar to AD than to VaD [10].
Although no significant differences were found in other domains, more detailed analyses revealed some group-specific patterns. For example, the Serial 7 Subtraction task, a classical working memory measure within the Attention domain, was the only subtest to show group differences. Working memory impairment has been reported to be similar in AD and VaD, or even more pronounced in VaD [38], which was also observed in our cohort. When considered as part of the executive functions’ spectrum, decline in working memory fits well with the established clinical profile of VaD [36]. Raimondi et al. [32] reported some differences: their AD patients performed better on orientation in time and place, but we failed to replicate this finding (see Table 2). Their patients were also slightly older than ours, which may partly explain the discrepancies. It should be noted that the Attention domain in the ACE-III has been criticized for limited construct validity and internal consistency. It combines heterogeneous tasks (orientation, registration, serial subtraction) rather than a pure measure of attentional capacity [14]. Including this caveat enhances transparency when interpreting domain-level results.
In the Fluency domain, overall scores were similar across groups. However, detailed analysis revealed that Letter Fluency differentiated between the populations being most impaired in VaD and most preserved in AD, with MD patients scoring in between. This pattern is consistent with other reports identifying letter fluency as a measure of executive functioning, thus more impaired in VaD [39]. In contrast, category Fluency (Animals) was similar across all groups, contradicting other findings from ACE III stu-dies [32]. Unlike in other published data [2, 40], our MD patients were similar to those with AD.
Although ACE-III provides a more extensive language assessment than other screening methods, we did not observe differences in the Language domain, suggesting comparable levels of language impairment across all three conditions. Although some authors have argued that VaD patients may be disproportionately affected by executive and syntactic deficits [8], our results did not support these findings. In general, the existing data on language performance in VaD are inconsistent, but most reports also suggest no specific differences between the populations. Moreover, we also failed to confirm the previously published suggestion of a distinct language pattern compared to both VaD and AD [2, 10, 40], which could be due to the relatively small number of patients.
Within the Visuospatial domain, only the Counting Dots task showed significant group differences, and it was the sole measure distinguishing AD and MD. Previous studies suggested better performance on this task in VaD, but our findings contradicted this result – VaD patients achieved the lowest scores; MD patients were similar to VaD patients, with AD having the highest score. The reported population consisted of patients with various levels of dementia severity (mild to severe), while our patients displayed only mild dementia, which can explain the discrepancies [41]. Other Visuospatial ACE-III tasks – 3D Wire Cube, Clock, Intersecting Infinity Loops, and Identifying Letters – also did not differentiate between the groups. This contradicts some reports [42] on the Clock drawing task for clinical differentiation but confirms other findings, suggesting its limited diagnostic value [43].
While the ACE-III provides a global measure of cognitive functioning, its true diagnostic potential lies in the analysis of separate cognitive domains – Attention, Memory, Fluency, Language, and Visuospatial abilities. Domain-level comparisons allow for the identification of cognitive signatures characteristic of different dementia subtypes, which may not be evident when considering total scores alone. In this context, post hoc analyses play a cri-tical role. The initial omnibus test (e.g., Kruskal-Wallis) indicates whether group-level differences exist, but only post hoc pairwise comparisons clarify which diagnostic groups differ. This distinction is particularly valuable in dementia research, where overlapping symptom profiles can obscure meaningful clinical differences [24]. Taken together, our results suggest that while global ACE-III scores are of limited diagnostic utility, domain-level and subtest-level analyses can reveal cognitive signatures that support clini-cal differentiation. VaD is characterized by relative pre-servation of episodic memory but impaired attention and executive tasks (serial sevens, letter fluency, dot counting). AD shows profound episodic memory deficits but relative sparing of working memory, executive functions, and visuospatial attention. MD closely resembles AD in its memory profile, supporting neuropathological evidence that mixed pathology often manifests as an AD-like syndrome with additional vascular burden [2].
Practical value
The present findings carry direct clinical relevance. In daily practice, many patients present with overlapping cognitive symptoms and inconclusive imaging results. Our study shows that while ACE-III total scores do not reliably distinguish between the dementia subtypes, the analysis of domain and subtest performance provides valuable diagnostic cues. Specifically, preserved episodic memory alongside impaired executive and attentional tasks (serial sevens, letter fluency, dot counting) suggests a vascular contribution. In contrast, severe episodic memory impairment points toward an Alzheimer’s or mixed aetiology. For clinicians working in the settings without an immediate access to advanced biomarkers or volumetric imaging, this domain-level approach can guide diagnostic reasoning, prompt earlier recognition of mixed cases, and encourage more targeted management of vascular risk factors.
Furthermore, ACE-III is quick to administer, free, and already widely used, making it a practical tool for both neurology and psychiatry clinics and outpatient facilities. Its use can improve triage efficiency by helping identify patients who would benefit from comprehensive neuropsychological testing or biomarker assessment.
Strengths and limitations
The strengths of this study include well-matched groups on demographic factors, examination of all patients by the same trained examiner, and detailed subtest- level analyses of ACE-III results. However, some limitations must be acknowledged. The sample size of 46 patients per group may be underpowered to detect minor differences, and all patients were at the mild stage of dementia, limiting generalizability to the prodromal or advanced stages. Furthermore, biomarker confirmation was unavailable, and the diagnoses relied on clinical criteria supplemented by neuroimaging reports, which sometimes lacked detailed descriptions of atrophy [44].
Future directions
Future research should address these limitations by including larger, multicentre cohorts with biomarker- based classification and longitudinal follow-up to evaluate whether ACE-III trajectories differ across dementia aetiologies. Integrating ACE-III results with imaging and fluid biomarkers may improve differential diagnosis accuracy. Additionally, existing digital adaptations of the ACE-III, combined with machine learning, may further enhance its discriminative utility.
Conclusions
The ACE-III can differentiate VaD from AD prima-rily at the domain and subtest level but does not reliably distinguish AD from MD. Episodic memory tasks (Recall and Recognition) best identify AD-related pathology, whereas executive and attentional tasks are more impaired in VaD. MD patients resemble AD more closely than VaD, reflecting underlying neuropathological overlap. While ACE-III remains a valuable screening and staging tool, its role in differential diagnosis should be considered complementary to standard neuropsycholo-gical, neuroimaging, and biomarker evidence.






