
Purpose
Keratinocyte carcinoma (KC), formerly known as non-melanoma skin cancer, encompasses basal cell carcinoma (BCC) and cutaneous squamous cell carcinoma (SCC). It is the most common form of cancer in the United States, affecting more than 3 million people annually [1, 2]. Although KC has low metastatic potential, it represents a significant source of morbidity and poses a large economic burden [3-6].
For patients with newly diagnosed KC, a wide variety of treatment options are available, including surgical and non-surgical approaches. The primary goals of treatment are to achieve effective disease control while preserving function and cosmetic appearance. In the United States, current standard of care involves a diagnostic biopsy, followed by surgical excision or Mohs micrographic surgery (MMS). Notably, the use of MMS has increased by approximately 400% from 1996 to 2008 [7]. Despite its efficacy, MMS is invasive, costly, and may have sub-optimal cosmetic outcomes, particularly when treating tumors located in functionally sensitive areas, such as the tip of nose, ears, mouth, or scalp. In these areas, surgery can pose risks of nerve damage, fibrosis, and undesirable scarring [8, 9].
Elderly population represents a growing demographic in KC management, as the incidence of cancer increases with age [10]. These patients often present with multiple comorbidities, reduced physiological reserves, and are at high-risk for surgical complications, making invasive procedures, such as MMS or wide local excision, less ideal [11]. Furthermore, many elderly individuals prioritize quality of life, functional preservation, and cosmetic outcomes over aggressive interventions. These factors highlight the need for effective, low-risk, and well-tolerated treatment alternatives to surgery [12].
Superficial radionuclide-based high-dose-rate (HDR) brachytherapy has emerged as a favorable treatment option modality for selected KC patients, offering excellent local control with minimal invasiveness [7, 13, 14]. Currently, according to guidelines from the American Brachytherapy Society (ABS) and the Groupe Européen de Curiethérapie, European Society for Radiotherapy and Oncology (GEC-ESTRO), superficial tumors with depth greater than 5 mm should be treated with interstitial implants to ensure adequate dose coverage and treatment efficiency [15, 16]. Recent publications have demonstrated feasibility of using individualized, home-made superficial brachytherapy molds for deep non-melanoma skin cancer, with critical reviews of recommendations regarding prescription depth, bolus thickness, and maximum dose in superficial radionuclide-based HDR brachytherapy with flaps and customized molds [17-19].
In this case series, we described the clinical outcomes associated with superficial radionuclide-based HDR brachytherapy for the treatment of deeper KC lesions (> 5 mm), and presented evidence that challenges the current guidelines. The purpose of this report was to critically evaluate the validity of a 5 mm depth cut-off.
Material and methods
After obtaining institutional board approval, we retrospectively reviewed four patients with pathologically confirmed KC, who were treated with superficial radionuclide-based HDR brachytherapy at one institution. Lesion depth was clinically and radiographically assessed by a radiation oncologist. All patients were immobilized with thermoplastic masks. Gross tumor volume (GTV) was determined visually and outlined by a treating physician. Clinical target volume (CTV) consisted of GTV with a 0.5 cm margin for BCC and 1.0 cm margin for SCC. Lesions were delineated on the skin during CT-simulation, and approved by the treating physician.
For three of the four patients with deep skin lesions, a custom, in-house multichannel flap applicator (Figure 1B) with a 1 cm source-to-skin distance (SSD) was applied to take advantage of the less pronounced dose fall-off. One patient was treated using a custom, in-house multichannel flap applicator, with a standard 0.5 cm SSD due to lesion location on the lip, where limiting dose penetration was a priority.
Fig. 1
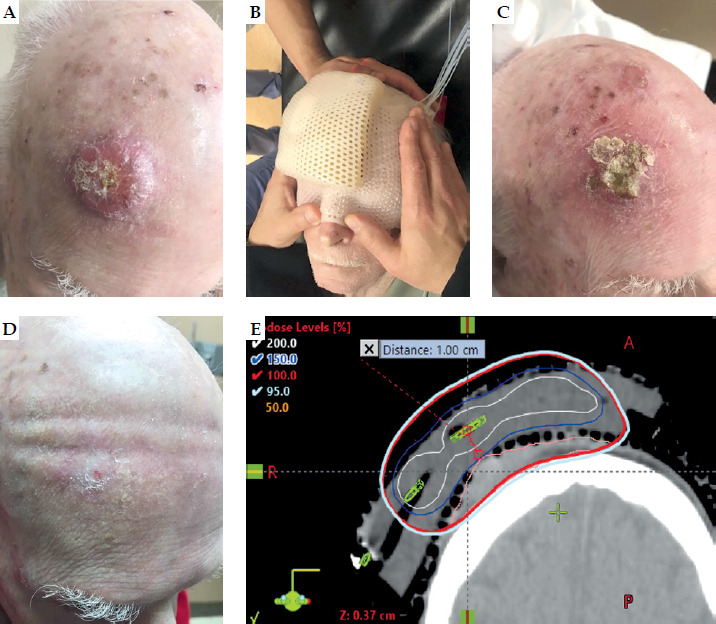
A 88-year-old male patient with biopsy-proven squamous cell carcinoma. A) Before treatment. B) In-house custom 1 cm multichannel flap applicator on patient in treatment position. C) Grade 2 radiation dermatitis at the end of treatment. D) Post-treatment. E) CT-based HDR brachytherapy treatment plan demonstrating isodose distribution with 1 cm SSD. The color-coded isodose lines demonstrate conformal dose coverage to CTV
Custom HDR skin flaps were fabricated using a tissue-equivalent bolus. Flap length was limited to ≤ 11 cm to maintain catheter trajectory accuracy. Bolus was cut to the desired length with an additional 1-2 cm of excess width for stabilization, and secured to a cardboard base with four peripheral pins. Transfer guide entrance and exit points were marked at 1 cm intervals.
Using a 17-gauge straight needle, channels were created at the mid-bolus height by advancing the needle along a controlled trajectory from entrance to exit. Needle path adjustments were performed incrementally to maintain consistent depth and minimize deviation. Following channel creation, HDR transfer guide tubing was inserted by advancing the tubing along the needle path, while gently withdrawing the needle to ensure accurate channel conformity. Tubes were intentionally over-advanced by 1-2 cm to facilitate final positioning and marker placement.
This process was repeated for all channels, with periodic re-alignment of the bolus to counteract deformations. After placement, stabilization pins were removed, and the bolus was trimmed to final width. The completed flap was wrapped in multiple layers of plastic film for infection control and durability, with guide tube markers secured flush to the bolus surface. Transfer guides were labeled by channel number at both the connector and flap interface to minimize the risk of setup error. The step-by-step demonstration of the skin flap fabrication process is provided in Supplementary material.
All treatments were delivered under direct supervision of an authorized user, whereas an authorized medical physicist confirmed accurate applicator positioning. Treatment dose was 40 Gy delivered in 8 fractions, twice weekly, with a minimum 48-hour interval between fractions. Individualized, CT-based planning was employed to ensure complete tumor coverage. Treatment planning was done in BrachyVision Eclipse treatment planning system (versions 15.6 and 16.1), with manual optimization utilized for treatment planning. Treatment was delivered with an iridium-192 radioactive source via a Bravos afterloader system by Varian. Dosimetric parameters V150, D95%, mean dose delivered to CTV, and maximal dose (defined as D0.1cc) were analyzed. Acute toxicity was assessed using Radiation Therapy Oncology Group (RTOG) criteria from 0 to 5. Toxicity and cosmetic outcomes were documented during each follow-up visit and graded by a radiation oncologist.
Results
Between March 2019 and November 2023, four patients were treated with HDR brachytherapy at a single institution (three females and one male). The median age of patients was 90.22 years (range, 81-95). Of the patients, three presented with SCC and one with BCC. Sites of the malignancies included the upper lip, scalp (Figure 1A), elbow, and distal forearm. The median depth of the tumor was 7.6 mm (range, 5.6-10.8). The median CTV volume was 7.8 cc (range, 2.3-13.3), the median V150 was 0.0057 cc (range, 0-0.09), and the median D95% was 95.1% of the prescribed dose (range, 94.9-102.4%). The median mean dose was 44.72 Gy (range, 41.61-48.38), the median maximal dose was 71.24 Gy (range, 52.23-87.45), while the median follow-up of the patients was 52.5 days (range, 0-150) (Table 1). There were no grade 3 or higher toxicities reported. The most common grade 2 toxicity was dryness and erythema (Figure 1C), which typically resolved by the end of the follow-up period, leaving minimal cosmetic discoloration or scarring (Figure 1D).
Table 1
Patient and treatment characteristics
Discussion
This current study demonstrates the efficacy of utilizing superficial nuclide-based HDR brachytherapy for treatment of deep (> 5 mm) KC, with an acceptable toxicity profile. As the incidence of KC continues to rise, so does the number of patients who require effective and tolerable treatment options. This is particularly evident in the elderly population, with over 80% of patients being treated for KC being over the age of 60 [20]. In this population, the presence of multiple comorbidities often limits surgical eligibility, increasing the need for effective and less invasive treatment alternatives.
Despite its low metastatic potential, untreated KC frequently diminishes quality of life (QoL) in elderly individuals due to local progression of the disease. Most often, invasive surgical intervention is pursued, which can lead to fibrosis or scarring. However, studies have demonstrated that maintaining skin integrity and aesthetics is strongly correlated with better post-treatment emotional and mental health outcomes in older adults, further indicating the need for less invasive options [21-23]. Therefore, successful treatment of KC in the elderly population necessitates benefits beyond tumor control, extending into patient well-being.
The ABS and GEC-ESTRO guidelines recommend the use of superficial brachytherapy for early-stage BCC and SCC, particularly in patients who are poor surgical candidates or have tumors located in cosmetically sensitive areas. They support the use of surface applicators for lesions with a depth ≤ 5 mm, and emphasize the importance of individualized treatment planning, accurate dosimetry, and patient-centered care. Additionally, the ABS endorses brachytherapy for lesions ≤ 4 cm in diameter, situated in locations where surgical excision may result in disfigurement or functional loss [15, 16]. Recent evidence has validated the use of individualized, home-made superficial brachytherapy molds for KC, with critical reviews of prescription depth, bolus thickness, and maximum dose considerations with flaps and customized molds [18, 24]. Additionally, surface mold brachytherapy for head and neck KC has demonstrated excellent local control rates and survival [17, 19]. Our current study’s use of surface-based radionuclide-based HDR brachytherapy for deeper lesions, expands upon this by demonstrating the feasibility of treating beyond superficial involvement, provided that appropriate dose coverage is achieved.
We found that superficial radionuclide-based HDR brachytherapy demonstrated effective local control in deep KC lesions, and resulted in minimally invasive cosmetic outcomes. The most common acute reactions were RTOG grade 2 toxicities, such as dryness and erythema. Importantly, no patients experienced grade 3 or higher events. Due to limited follow-up in this series, long-term toxicity data could not be evaluated.
A key dosimetric consideration was utilizing the inverse square law to optimize dose distribution and minimize high-dose exposure to the skin surface [25]. By developing a custom 1 cm SSD applicator, we were able to use the rapid fall-off in dose with increasing distance from the source. This allowed for effective coverage of deeper tumor volumes while limiting the volume of the skin receiving 150% of the prescribed dose (V150), thereby reducing the risk of surface toxicity. Although the inverse square law provides a useful conceptual framework for understanding geometric dose fall-off, it should be noted that in brachytherapy, the radioactive source cannot be strictly approximated as a point source at short distances typically evaluated. The inverse square law is most accurate when the distance from the source is several times greater than the physical length of the source, a condition that is often not fully met in brachytherapy applications. Consequently, deviations from ideal inverse square behavior occur due to the finite source length and anisotropic emission characteristics of HDR sources. In clinical brachytherapy dose calculations, these effects are more accurately described using TG-43-based geometry, radial dose functions, and anisotropy corrections. These factors help explain differences in spacing between isodose curves, such as those between the 100% and 150% dose levels, which may not strictly follow the inverse square scaling as demonstrated in prior studies [18]. Precise source placement and individualized treatment planning were essential in achieving this goal, supporting the favorable toxicity profile observed in this series.
Emerging technologies in brachytherapy for customized applicator design, such as 3D printing, offer promising avenues for further optimization of dose distributions and treatment delivery [26, 27]. While our study utilized traditional fabrication methods for applicator construction, future integration of 3D-printed molds may enhance reproducibility in the treatment of complex anatomical sites.
Limitations of the case series that need to be acknowledge include a small sample size and short-term follow-up, which may underestimate long-term recurrence and late toxicity. Nevertheless, these outcomes serve to reinforce the role of superficial radionuclide-based HDR brachytherapy for deep KC in appropriately selected patients.
Conclusions
This case series demonstrates the use of superficial radionuclide-based HDR brachytherapy as a safe and effective treatment modality for deep (> 5 mm) KC, particularly in elderly patients who are not ideal surgical candidates. With a favorable acute toxicity profile and effective local control in limited follow-up, this treatment shows potential as a non-invasive approach for lesions that are > 5 mm deep. Further research with larger cohorts and extended follow-up are needed to validate long-term outcomes.








