
Purpose
Carcinoma of uterine cervix constitutes a major cause for cancer-related morbidity and mortality in Indian women. GLOBOCAN India 2020 data reveals that cancers of cervix uteri have the second most common incidence rate among females (18.3%) as well as mortality rate (9.1%) in all age groups [1]. Most patient demographics for these malignancies include women of the middle or lower income groups and those from rural settings. Being a preventable and highly curable cancer, these statistics pose major challenges in the eventual outcomes for this patient population.
Majority of these tumors present in advanced stages, with radical chemoradiation followed by brachytherapy being the standard of care [2]. With better therapeutic resources and improved technological access, patients are experiencing enhanced clinical outcomes with longer disease-free and overall survival (OS) periods [2]. In recent years, brachytherapy has been a major contributor to providing excellent results for even more advanced disease stages [2, 3]. The addition of volumetric imaging, treatment planning system-based contouring, and planning as well as optimized and individualized treatment delivery, have added immensely to the range of therapeutic team [4].
Over the last few years, the focus of brachytherapy management has shifted from ‘one-size-fits-all’ to a more analyzed, catered, and personalized approach, allowing each patient to receive a plan matching their respective disease status. The reason for this change is the fact that, as more patients are surviving longer, loco-regional failure patterns and local complication rates are being further scrutinized to try and shift the curve positively and to improve outcomes and quality of life.
Hybrid intracavitary/interstitial (IC/IS) applicators represent a key innovation in this regard [2, 5, 6]. Diverging catheters used in hybrid systems enable better access to distal parametrial disease, ensuring adequate tumor coverage, particularly in irregular or asymmetric volumes, which may not be optimally treated by traditional IC/IS techniques [5, 6]. This expanded reach enhances therapeutic doses to target volumes while maintaining organs at risk sparing [3]. Traditional interstitial brachytherapy templates often require transperineal needle placement, which can be invasive, uncomfortable, and logistically demanding [2]. In contrast, the Tulip Add-On kit is a patient-friendly alternative, designed to be used with existing intracavitary applicators, such as Henschke, Fletcher-Suit, or ring systems, allowing transvaginal insertion of interstitial plastic needles through pre-defined guiding channels [7]. This design reduces procedural invasiveness while preserving implant precision and stability [7].
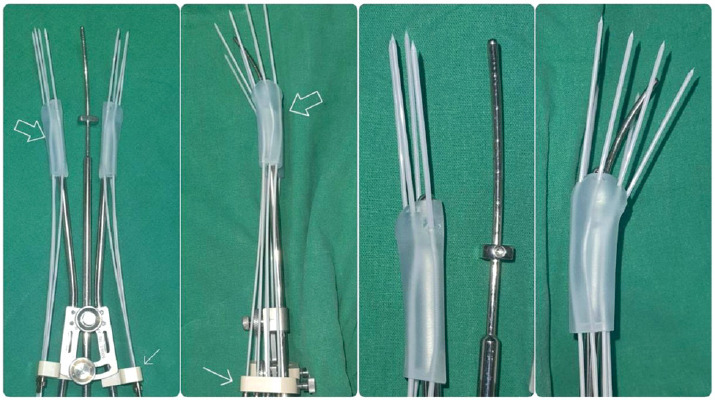
Availability of 3D printing technology, in addition to the upgraded standard brachytherapy kits, have provided an alternative and unique therapeutic option for centrally and/or para-centrally located residual diseases after completion of external radiation therapy [8, 9]. The Tulip Add-On interstitial kit with plastic needles designed for Henschke, Fletcher-Suit, or ring intracavitary applicator sets, operates in this concept of adaptive target volume coverage [7, 9]. It consists of two parts, i.e., needle guide and needle template. Needle guide (3D-printed component) is attached to the existing ring or ovoid tube of IC applicators, providing secure and accurate needle guidance with different pre-fixed guiding angles to cover target areas [9, 10]. The needle template latches onto the proximal end of IC tube, and ensures implanted needles’ secured placement during treatment [7] (Figure 1).
In this paper, we presented our initial clinical experience of using the Tulip Add-On interstitial kit designed for Henschke intracavitary applicator sets.
Material and methods
Between January 2021 and January 2022, eight patients with uterine cervical cancer of FIGO stages IIB to IIICr1, treated at a tertiary care university teaching hospital, underwent combined IC/IS brachytherapy using Tulip applicator with Add-On set.
External beam radiotherapy
All patients were treated with a 6 MV linear accelerator (Elektra Synergy) using three-dimensional conformal radiotherapy (3D-CRT) technique to a dose of 45 Gy in 25 fractions over 5 weeks, along with concurrent weekly cisplatin chemotherapy. In our institution, boost doses to enlarged nodal regions are decided upon physician’s discretion, and are administered up to a dose of 54 to 60 Gy, depending on the location. However, none of the patients in this series received any boost dosing.
Brachytherapy details
Procedure
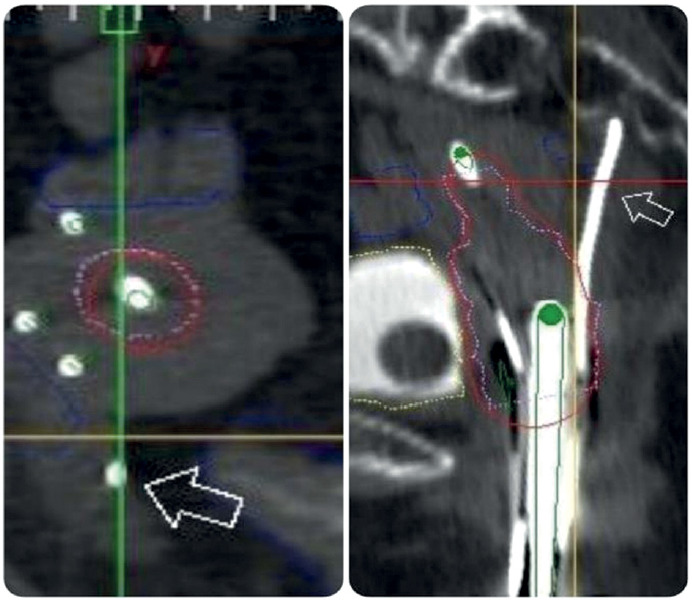
In all patients, brachytherapy was performed after an interval of 10-15 days from the last day of external radiation, and it was conducted under combined spinal-epidural anesthesia in the operating theatre. Following an examination under anesthesia (EUA), the standard Henschke applicator with the Tulip Add-On kit was placed. In four patients, the Add-On kit was provided into one side, whereas the other four patients had the kits placed bilaterally, with majority of them requiring all 4 needles to be inserted. Following this, patients underwent computed tomography (CT) planning scan with 2.5 mm slices, with diluted bladder and rectal contrast for accurate organ at risk (OAR) delineation. These images were transferred to the treatment planning system (SagiPlan v. 2.0.1), where the applicators were digitized according to protocol. In one patient, a posteriorly angled needle was abutting the rectum (Figure 2), and was close to the pelvic side wall musculature. Therefore, it was decided to remove this one needle to avoid any perforation or pain during treatment. OARs, including the bladder, rectum, and sigmoid colon as well as high-risk clinical target volume (HR-CTV) were delineated by a radiation oncologist. Intermediate-risk clinical target volume (IR-CTV) was created by applying 10 mm margin to HR-CTV, and trimming it from OARs.
Dosimetry
Subsequently, the physicist activated dwell positions in the applicators, and prescribed to HR-CTV a dose ranging from 6.5 to 7.5 Gy, delivered in 3-4 fractions, over two consecutive days. During optimization, isodose re-shaper was used to improve coverage and minimize OAR doses.
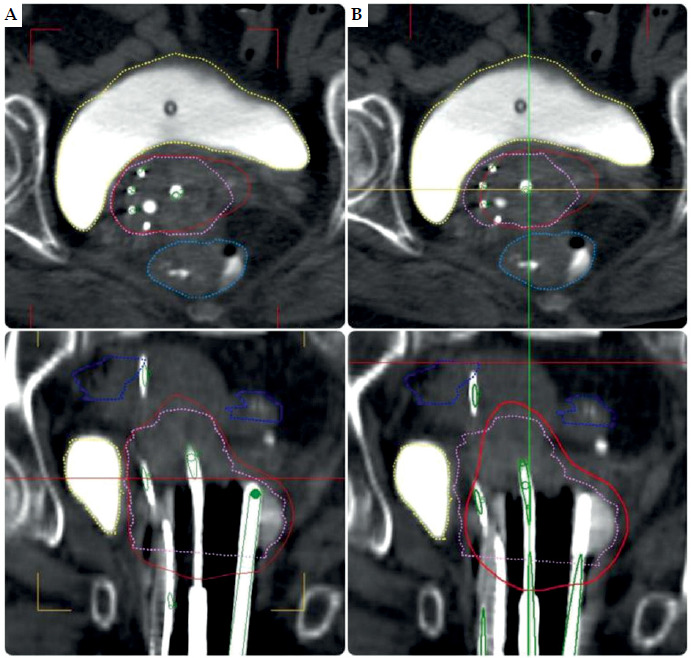
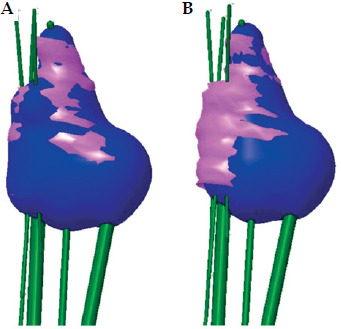
A second plan was generated with the same scan, in which only tandem and ovoids were activated (without the needles) to deliver the same dose to HR-CTV and similar OAR constraints (Figures 3 and 4). Various dosimetric parameters, such as dose received by 0.1 cc, 1 cc, and 2 cc of the bladder, rectum and sigmoid colon, were recorded for both plans. Also, dosimetric parameters with regards to HR-CTV, such as D90, D98, D100, V90, V100, V150, and V200, were also documented for comparison of the two plans.
Fig. 3
Dose distribution with (A) and without (B) needles
HR-CTV – pink; Isodose – red; Bladder – yellow; Rectum – light blue; Sigmoid – dark blue
The equivalent dose in 2 Gy (EQD2) was calculated using the following formula:
EQD2 = nd [(1 + d / α/β) / 1 + 2 / α/β)]
where n is the number of fractions, d is the dose per fraction, and α/β is 10 for tumor/3 for tumor.
These EQD2 data were incorporated into planning parameters, allowing to determine doses to HR-CTV needed to be achieved as well as constraints to be met for OARs.
Treatment
Following approval of the plan by the radiation oncologist, treatment was executed using BEBIG SagiNova unit (Eckert & Ziegler), with a minimum of 6 hours interval between fractions, over two consecutive days. The needle obturators were kept in-situ between fractions to avoid any twisting or compression of the plastic tubes. At implant removal, the policy is always to first remove the needles and then extract the tandem and ovoids, as this can prevent shearing resulting in injury and hemorrhage. Most patients had minimal to no bleeding, and were discharged on the same day.
Results
Between December 2020 and January 2022, eight patients with favorable clinical profiles were treated with IC/IS brachytherapy using an add-on applicator kit. The median age was 58 years (range, 50-70 years). Based on FIGO staging, five patients were stage IIIB, one was IIB, and two were IIICr1 due to pelvic nodal involvement, with all having good performance status and no major comorbidities (Table 1).
Table 1
Patient demographics and treatment characteristics
After completing external beam radiotherapy (EBRT), the patients were re-assessed with MRI. All scans showed persistent medial parametrial involvement, prompting the use of an IC/IS technique for better dose coverage. The Henschke applicator was applied with add-on interstitial needles; six patients had bilateral needle insertion and two had unilateral placement based on disease extent. Brachytherapy was delivered over two days. Four patients received 4 fractions of 6.5 Gy, two received 3 fractions of 7 Gy, and two received 3 fractions of 7.5 Gy. The median HR-CTV was 55.6 cc (range, 25.6-81 cc), and was larger than volumes typically seen with intracavitary brachytherapy alone.
Dosimetric comparison between the IC/IS (Tulip) and conventional tandem/ovoid (IC-only) plans confirmed similar OAR doses. The median rectal D2cc was 65.90 Gy with Tulip vs. 65.46 Gy with tandem/ovoid, bladder D2cc was 71.63 Gy vs. 74.01 Gy, and sigmoid D2cc was 55.10 Gy vs. 54.98 Gy.
However, target coverage was significantly better with the IC/IS approach. The median D90 to HR-CTV was 77.24 Gy with Tulip vs. 69.54 Gy with tandem/ovoid. Similarly, D98 was 77.24 Gy vs. 69.54 Gy, and D100 was 63.83 Gy vs. 56.95 Gy, respectively (Table 2).
Table 2
EQD2 dosimetric parameters
In summary, while OAR doses were comparable, the IC/IS technique provided superior target coverage, especially in cases with residual medial parametrial disease, supporting its role in improving local control in advanced cervical cancer. Table 3 shows the implant metrics for both Tulip applicator compared with tandem/ovoid one. All metrics indicated better implant parameters for the Tulip application with higher DHI and CI values as well as lower DNR and ODI numbers, suggesting a more appropriate and ideal application compared with the tandem/ovoid procedure for this patient series.
Table 3
Dose-volume parameters to assess implant metrics
[i] V90 – volume of HR-CTV (cc) receiving 90% of dose, DHI – dose homogeneity index: ratio of the target volume, receiving a dose in the range of 1.0 to 1.5 times of the reference dose to the volume of the target that received a dose equal to or greater than the reference dose (ideal: 1), DNR – dose non-uniformity index: ratio of the target volume, receiving a dose equal to or greater than 1.5 times of the reference dose to the volume of the target that received a dose equal to or greater than the reference dose (ideal: 0), ODI – overdose volume index: ratio of the target volume, receiving a dose equal to or more than 2 times of the reference dose to the volume of the target that received a dose equal to or greater than the reference dose (ideal: 0), CI – coverage index: fraction of the target volume, receiving a dose equal to or greater than the reference dose (ideal: 1)
Discussion
Traditionally, intracavitary brachytherapy (ICBT) using tandem with ovoids or ring applicators, has been the cornerstone of definitive radiotherapy for cervical cancer. This method, based on point A dosimetry, delivers radiation to a defined anatomical point irrespective of tumor volume, shape, or topography. While this technique is adequate for small, symmetrical tumors confined to the cervix, its limitations become evident in larger tumors, or in those with asymmetrical or lateral extension into the parametria, where inadequate coverage can compromise local control [4, 8, 11].
To address these shortcomings, image-guided adaptive brachytherapy (IGABT) has emerged as a transformative approach. IGABT incorporating volumetric imaging, such as MRI or CT, into planning, enables visualization of the tumor (HR-CTV) and adjacent OARs, allowing dose adaptation tailored to patient-specific anatomy [12]. The integration of interstitial needles into intracavitary applicators, termed hybrid brachytherapy (IC/ISBT or HBT), has further improved dose conformity and therapeutic outcomes [3]. Applicator systems, such as the Vienna (tandem + ring + needles), Utrecht (tandem + ovoid + needles), Venezia, and Geneva, enable oblique needle insertion into the parametrial tissues, effectively expanding the dose coverage laterally to the uterus [13].
Nomden et al. evaluated the clinical feasibility of the Utrecht applicator; although it provided adequate coverage for medial parametrial disease, it was often insufficient for distal extensions [6]. To address this, Fokdal et al. proposed integration of free-hand interstitial needles beyond the limits of the fixed channels of hybrid applicators. Their work showed that such additions could achieve improved dosimetric coverage in distal parametrial disease while maintaining acceptable toxicity profiles [14]. Despite the procedural complexity and learning curve, these techniques demonstrated clinical feasibility, and are increasingly being adopted in high-volume centers.
Further modeling studies by Yoshida et al. compared ICBT, IC/ISBT, and ISBT, across varying tumor volumes ranging from 8 cc to 112 cc. They found that, while ICBT sufficed for small tumors, IC/ISBT began to outperform it for tumors exceeding 36 cc, and ISBT was significantly superior for tumors larger than 80 cc [10]. Kirisits et al. also reported that, while the 100% isodose is in line with ICBT extending approximately 25 mm from the tandem at the level of point A, it could reach 31 mm with IC/ISBT, highlighting its superior spatial dose distribution [15].
Hong et al. stratified patients by parametrial extension width (≤ 3 cm, 3.1-3.5 cm, 3.6-4 cm, and > 4 cm), and showed that the addition of distal parametrial interstitial needles (IC/IS + ISBT DP) provided a dosimetric benefit to only extensions > 3 cm, aligning with previous findings by Kirisits et al. [16].
These studies collectively reinforce that the benefit of hybrid or interstitial brachytherapy becomes evident with increasing tumor volume or lateral extension.
Comparative planning studies have further established the superiority of IC/ISBT. In a cohort of 51 patients with locally advanced cervical cancer, Mohamed et al. reported that the HR-CTV D90 was significantly higher in patients treated with IC/ISBT (84 Gy) compared with those who received ICBT plus an EBRT parametrial boost (79 Gy). Additionally, the IC/ISBT group demonstrated lower D2cc values for the bladder and rectum, reflecting improved OARs sparing [9].
Evidence from large prospective cohorts, particularly the EMBRACE trials, has further solidified the role of IC/ISBT in modern brachytherapy. The EMBRACE I study reported a 3-year local control rate of 92% for patients treated with MRI-guided IC/ISBT, with favorable toxicity profiles even in patients with extensive disease or poor response to EBRT [3]. The EMBRACE II trial, a prospective multicenter study initiated in 2016, focused on optimizing multiparametric dose constraints and individualized treatment planning to improve therapeutic ratios. While final peer-reviewed results are awaited, interim analyses presented at ESTRO 2025 provided important insights supporting this approach [12].
Recent literature confirms our findings and further strengthens utilization of IC/IS hybrid techniques. Wark et al. reported on 149 patients treated with MRI-guided IC/IS brachytherapy, achieving a median D90 of 88.9 Gy and local control of 81% at 24 months, with tolerable toxicity profiles [17]. Haider et al. reported that in a low-resource setting, the use of Venezia hybrid applicators led to a complete response rate of 65.9%, with no grade 3-4 toxicities [18]. Similarly, Le et al. described the successful use of CT-guided outpatient hybrid brachytherapy under minimal sedation, with 96.8% feasibility and only 22% bleeding incidents [19]. These studies demonstrate that hybrid techniques can be applied across various clinical contexts, from high-income, MRI-based centers to outpatient, resource-limited settings.
An institutional review from India (2025) showed that among 71 patients treated with tandem-ovoid-based IC/IS brachytherapy, a median D90 of 87.4 Gy EQD2 was achieved, with local control rate of 83.6% and OS of 88.6%, along with acceptable GU/GI toxicity profiles [20].
Najjari-Jamal et al. in their review of recent phase III trials, including OUTBACK, INTERLACE, and CALLA, found that, while IGABT was increasingly adopted, the use of volume-based planning with IC/IS brachytherapy was still underutilized (23-60% use), indicating room for broader implementation [21]. In line with this evidence, the American Brachytherapy Society (ABS) 2025 consensus guidance explicitly recommended hybrid IC/IS brachytherapy as standard of care for patients with large HR-CTV, asymmetrical or parametrial extension, or sub-optimal geometry [22].
In our institutional experience, we utilized the Tulip Add-On interstitial needle kit that integrates with the Henschke intracavitary applicator, allowing precise needle placement in patients with persistent parametrial disease post-EBRT. This approach is particularly valuable in resource-limited settings, where newer, costlier applicators may not be available. Among the eight patients treated with this method, dosimetric analysis comparing needle-loaded vs. non-loaded plans demonstrated that OAR doses (D1cc for the bladder, rectum, and sigmoid) remained comparable or were slightly reduced with the use of interstitial needles. More importantly, target coverage parameters (D90, D98, D100, V90, and V100) showed significant improvement in needle-loaded plans. Additionally, quality indices, such as conformity index (CI) and dose homogeneity index (DHI), were superior in the needle-loaded group, with median CI of 0.615 and DHI of 0.556. At the same time, indicators of non-uniformity, such as dose non-uniformity ratio (DNR) and overdose volume index (ODI), were lower, reflecting improved dose distribution and reduced hot-spots.
Our findings re-affirm the growing body of evidence supporting hybrid brachytherapy, especially in tumors with HR-CTV volumes > 36 cc, medial/lateral parametrial persistence, or poor response post-EBRT. The Tulip Add-On system offers a practical and effective solution for centers transitioning from traditional ICBT to image-adapted hybrid techniques. As global brachytherapy practice moves towards individualized, image-based protocols, resource-adaptive hybrid applicator systems, such as the Tulip, may play a vital role in closing the gap between evidence and accessibility.
Conclusions
The ratio of HBT in brachytherapy of cervical cancer has increased from 4.8% in 2015 to 13% in 2019. Many radiation oncologists are now accustomed to HBT procedure that is more invasive than ICBT, and they are now implementing HBT to increase the dose to the involved parametria. The evidence indicates that the radiotherapy technique of HBT has excellent dosimetry parameters for cervical cancer patients with distal parametrial extension. The use of advanced applicators, such as the Tulip system, further enhances the ability to reach lateral disease while maintaining optimal organs at risk sparing.
So far, there is no published prospective trial investigating the superiority of HBT over conventional ICBT in the management of locally advanced uterine cervical carcinoma (LAUCC), even though its advantages seem plausible, considering that it enables individualized, three-dimensional (3D), anatomy-oriented dosimetry. The actual indication of ICBT, HBT, and multicatheter ISBT, is a challenging topic that needs clinical experience in order to select the most appropriate brachytherapy modality depending on tumor size and shape. Hybrid brachytherapy is the patient-friendly answer for combining the simplicity of ICBT with similar coverage as ISBT, with a potential for better conformity and coverage, along with reduced dose to organs at risk.








