
Fibrous dysplasia (FD) is a lesion arising from the bone marrow, accounting for 30–50% of all benign tumors within the chest wall. In FD, normal bone is replaced by fibrous connective tissue and irregularly formed woven bone [1]. The disease affects both sexes equally and can occur at any age, although its peak incidence is observed in the third decade of life. Based on systemic manifestations and the extent of skeletal involvement, fibrous dysplasia is classified into one of four forms: monostotic, polyostotic, or associated with McCune-Albright syndrome or Mazabraud syndrome [2].
Diagnosis relies on the clinical picture, imaging studies – primarily computed tomography (CT) and magnetic resonance imaging (MRI) – as well as histopathological examination, which is essential to confirm the diagnosis and to exclude aggressive malignant lesions such as telangiectatic osteosarcoma [2]. The standard therapeutic approach for benign sternal tumors typically involves curettage of the lesion with cavity filling using either bone graft or bone cement, often combined with stabilizing techniques such as titanium or synthetic meshes to reinforce chest wall stability.
In this report, we present a case of fibrous dysplasia of the manubrium sterni in a 31-year-old woman. The aim is to provide a detailed description of the clinical features, diagnostic findings, surgical treatment including reconstruction, and follow-up outcomes in this rare presentation, which may contribute to better understanding and optimization of management strategies in patients with sternal fibrous dysplasia.
A 31-year-old female patient with suspected aneurysmal bone cyst of the sternum was admitted to the Department of Thoracic Surgery in March 2025 for surgical treatment. The patient was in good general condition, a non-smoker, and without comorbidities. She reported no symptoms. The lesion was incidentally detected during a postpartum spinal MRI performed as a follow-up examination, which revealed abnormalities in the sternum. A chest CT performed approximately 4 months before admission demonstrated an expansile lesion of the manubrium sterni with periosteal disruption and invasion of adjacent soft tissues, measuring 43 × 21 mm (Figure 1 A). The patient was on combined oral contraception containing 0.03 mg ethinylestradiol and 2 mg dienogest, taken once daily. Past medical history included a bone cyst of the left fibula in 2009. Her father had a history of colorectal cancer.
Figure 1
Radiological and intraoperative images. A – Chest computed tomography (CT) scan showing a lesion in the manubrium sterni. B – Intraoperative view of the anterior plate of the sternum with a bone defect. C – Cavity filled with surgical cement mixed with gentamicin. D – Anterior surface of the sternum covered with a mesh fixed with sutures
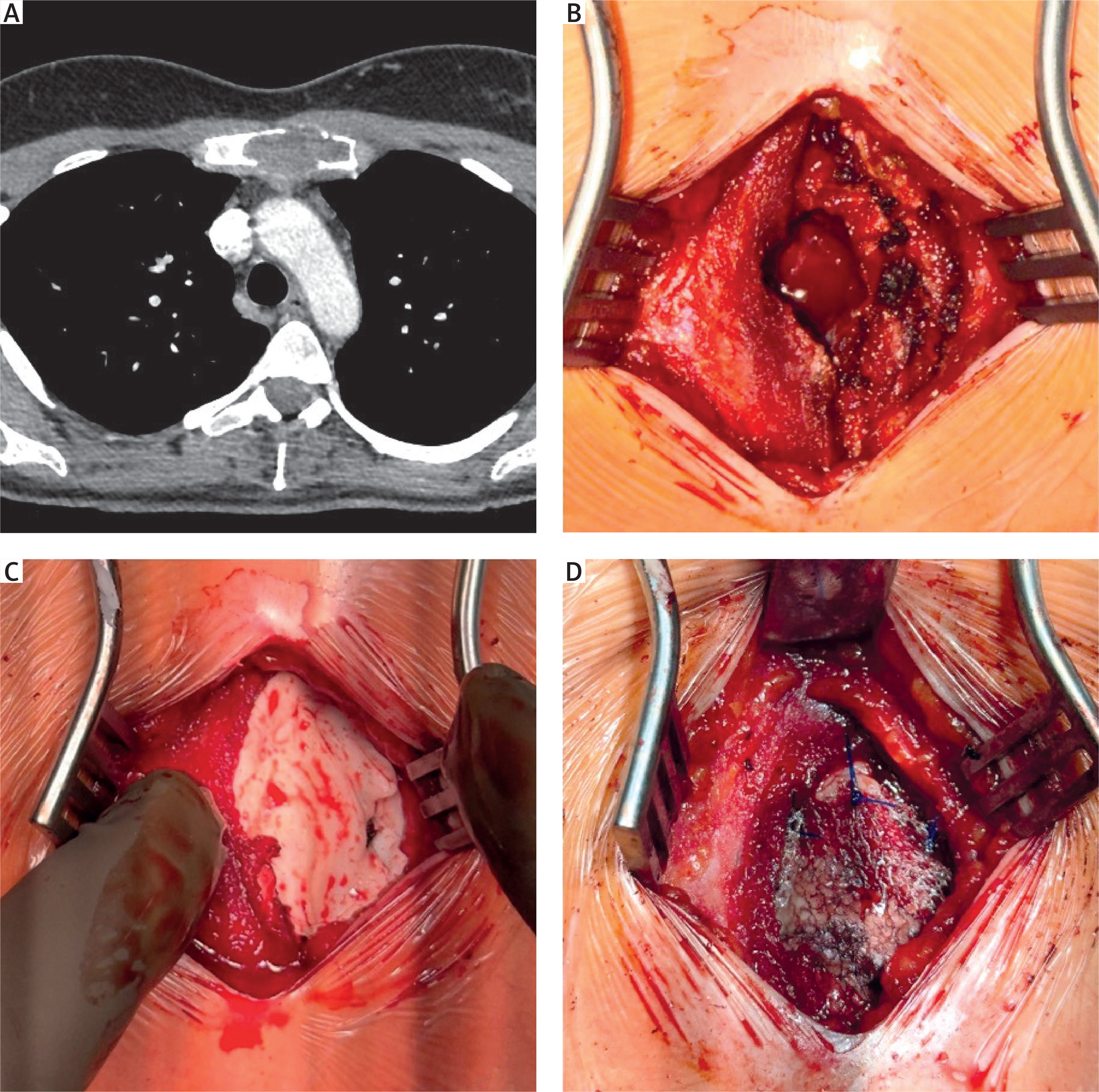
Under general anesthesia, a midline incision over the manubrium sterni was made. Following dissection, a small anterior cortical defect was noted (Figure 1 B). The cortical defect was enlarged, and the pathologically altered marrow cavity was curetted. The material was sent for histopathological analysis. A mesh was introduced into the bottom of the cavity, followed by surgical cement mixed with gentamicin, filling the cavity (Figure 1 C). A mesh was applied to the anterior surface of the sternum, covering the bone defect. The mesh was secured with simple sutures (Figure 1 D). The wound was closed with sutures, and a sterile dressing was applied. Postoperatively, the patient was transferred to the recovery ward and received analgesic treatment. The procedure was uneventful.
Histopathological evaluation suggested a diagnosis of fibrous dysplasia. A postoperative chest radiograph revealed cement filling at the site of the resected lesion in the left part of the manubrium, thoracic scoliosis, and no other abnormalities.
One month after discharge, the patient reported satisfaction with the treatment outcome. The only complaint was occasional pruritus in the operated area.
The clinical and radiological presentation of fibrous dysplasia can be highly variable, mimicking other benign bone lesions such as aneurysmal bone cyst (ABC), giant cell tumor of bone (GCTB), osteoma spongiosum, or simple bone cyst. The monostotic form of FD is the most common, with a spectrum ranging from asymptomatic cases, as in this patient, to severe manifestations with pain, pathological fractures, and significant bone deformities [2]. Aneurysmal bone cysts should always be considered in the differential diagnosis, as its clinical picture is nearly indistinguishable from FD. ABC is a rare (2.5% of primary bone tumors), benign, but often locally aggressive and expansile lesion characterized by blood-filled multi-chamber cavities, which are absent in FD. ABC typically arises in the metaphyses of long bones (most commonly the femur, tibia, and humerus) and in the spine and in about 80% of cases is diagnosed before the age of 20 [3, 4], while FD is more frequently detected in patients over 30 years of age [5].
When clinical, radiological, and histopathological findings are inconclusive, genetic testing may aid in diagnosis. Fibrous dysplasia has been associated with mutations in the GNAS gene (guanine nucleotide-binding, alpha-stimulating complex locus) located on chromosome 20q13.3, encoding the alpha subunit of heterotrimeric Gs protein. Identification of this mutation facilitates differentiation from primary ABC, which may harbor USP6 rearrangements, or secondary ABC, arising in the context of other bone lesions [2, 3, 5].
In the presented case, the combination of imaging (CT and MRI – superior for showing possible fluid-fluid levels inside the lesions) and histopathological findings strongly favored the diagnosis of fibrous dysplasia, while excluding malignancy such as telangiectatic osteosarcoma.
For benign sternal tumors without massive bone or soft tissue destruction, reconstruction using bone cement stabilized with surgical meshes remains a preferred approach. This technique ensures chest wall stability while minimizing extensive scarring or keloid formation, which may be of significant esthetic and psychological importance, particularly in young women. In cases of extensive destruction, however, total sternotomy may be required, necessitating complex chest wall reconstruction using materials such as polypropylene or polytetrafluoroethylene (PTFE) patches, methyl methacrylate meshes, or titanium plates and clips [6].
In recent years, autologous bone grafting has emerged as a promising alternative to synthetic materials, offering reduced infection risk and improved biomechanical properties. Rib grafts are most commonly harvested, though in large chest wall defects this approach may increase perioperative mortality. Such strategies have been described, for example, by Sheikhy et al. [7]. The patient provided informed consent for her case to be described in this report.









