
Introduction
Sternal fractures are uncommon but clinically significant injuries resulting from blunt thoracic trauma. They can be broadly classified into 2 categories: isolated sternal fractures (ISF), which are typically localised and less severe, and polytrauma-associated sternal fractures (PSF), which are frequently accompanied by severe concomitant injuries and may be life-threatening [1, 2]. Distinguishing between these 2 entities is essential for optimal patient management and rational allocation of healthcare resources.
The predominant mechanism of injury is high-energy impact to the anterior chest wall, most often caused by motor vehicle collisions (MVCs). These injuries occur particularly in belted drivers without airbag deployment [1, 3, 4]. With the widespread use of seatbelts, trauma patterns have shifted, resulting in an increased incidence of sternal injuries as part of so-called “seatbelt syndrome” [1, 3–5].
This paper presents a rare case of a polytrauma patient with a flail chest due to bilateral rib fractures and a displaced sternal fracture, managed surgically with rigid fixation. A literature review is also provided to contextualise this case within current therapeutic strategies.
Case presentation
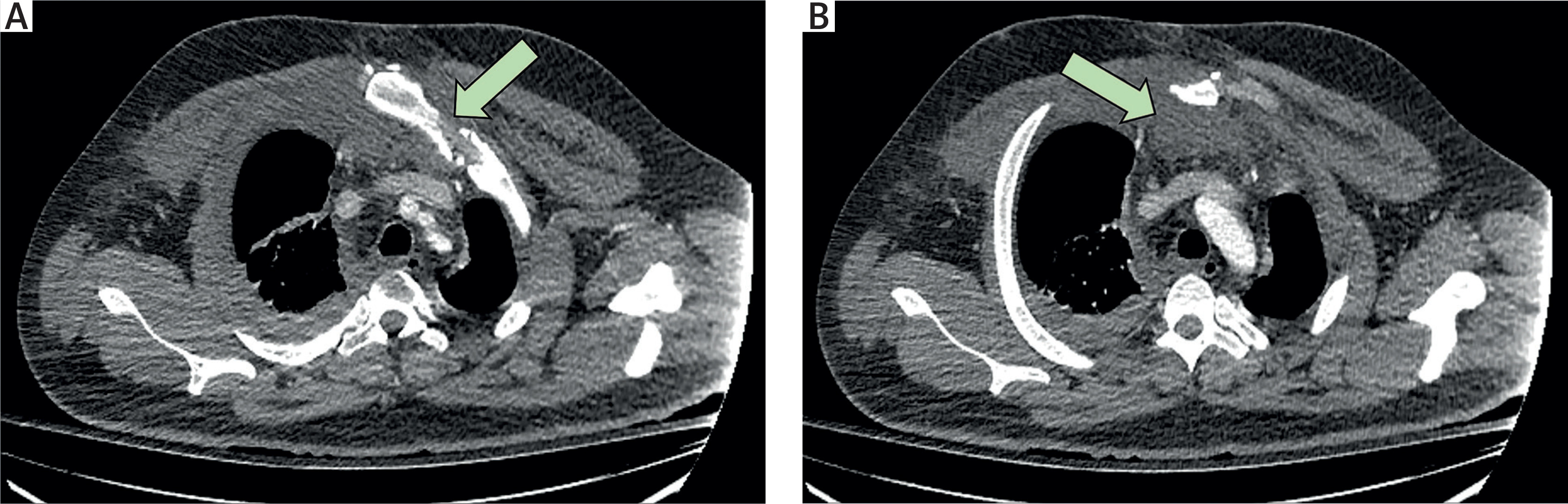
A 33-year-old male was transferred from a regional hospital after a high-impact motor vehicle collision that resulted in the death of the driver. On arrival, he was haemodynamically stable with a Glasgow Coma Scale (GCS) score of 15/15 and was assessed by a multidisciplinary trauma team. Imaging demonstrated a left hip dislocation, a displaced sternal fracture – manually reduced in the emergency department and temporarily stabilised with skin traction – multiple rib fractures (right 4th–8th, left 6th–7th), flail chest, pulmonary contusion, and a sizable retrosternal haematoma without active bleeding (Figure 1). Additionally, the patient had deep lacerations on the anterior aspects of both knees, which were sutured in the emergency department.
Figure 1
Preoperative computed tomography (CT) images demonstrating: A – displaced manubriosternal dislocation, B – associated retrosternal haematoma
Surgical management
The patient was admitted to the Cardiothoracic Surgery Department for close monitoring and stabilisation. Bilateral chest tubes were inserted, each draining approximately 1.5 l of haemorrhagic fluid. Definitive surgical management was performed in collaboration with cardiothoracic and orthopaedic teams.
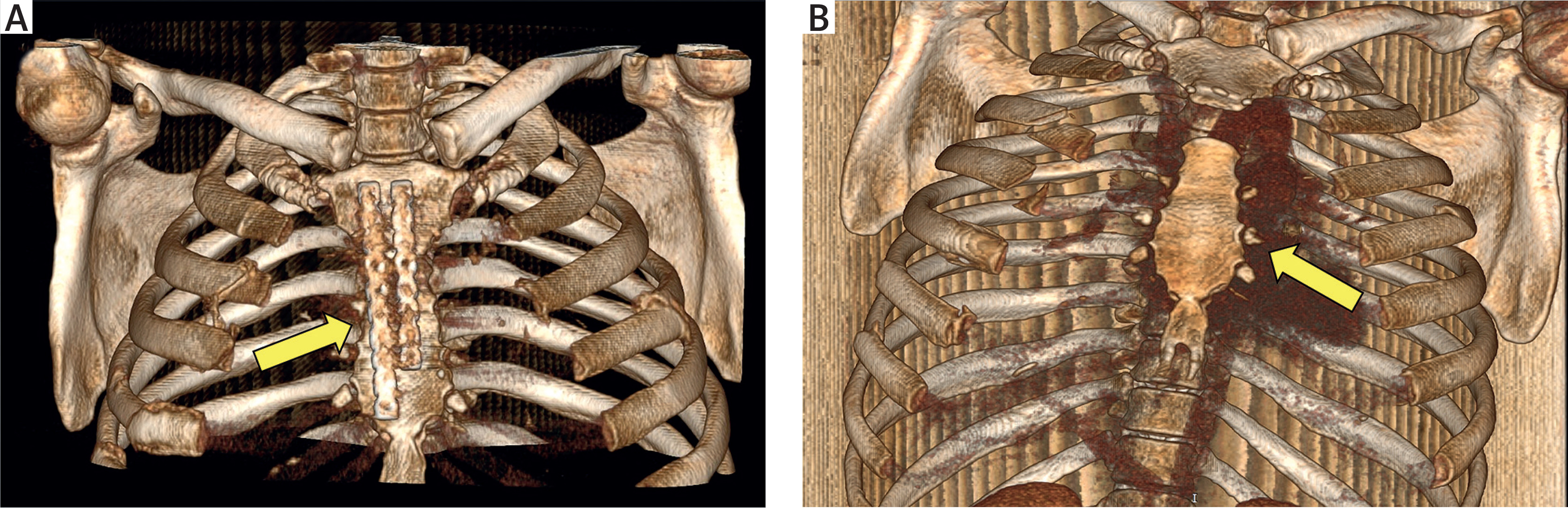
A 10-cm midline incision was made, and the retrosternal haematoma was evacuated. The dislocation between the manubrium and the sternal body was corrected by excising intervening cartilage and bone fragments. Rigid fixation was achieved with open reduction and internal fixation (ORIF) using 2 side-to-side reconstruction titanium plates (3.5 mm) and locking screws (Figure 2). Due to soft tissue interposition at the fracture site, meticulous surgical debridement was performed, and the defect was filled with bone graft to facilitate union. Haemostasis was secured, 2 drains were placed, and the wound was closed in anatomical layers.
Postoperative course
The patient initially recovered uneventfully and was discharged on postoperative day 15. However, he was readmitted one month later with persistent serous wound discharge. Culture identified Proteus mirabilis, for which targeted antibiotic therapy was initiated. A vacuum-assisted closure (VAC) device was applied, resulting in progressive improvement. After 15 days of VAC therapy, the wound had healed satisfactorily, and the patient was discharged in good condition.
Discussion
This case highlights the critical importance of early surgical stabilisation in managing unstable sternal fractures (SFs) within the setting of polytrauma. Although postoperative wound infection represented a significant complication, it was effectively managed through targeted antibiotic therapy and vacuum-assisted closure (VAC), underlining the value of multidisciplinary care in complex thoracic trauma.
Literature review methodology
A focused literature search was conducted in PubMed and Scopus using the terms “sternal fracture”, “operative management”, “sternal plating”, and “polytrauma”. Articles published in English between [year–year] were considered. Reference lists of relevant studies were also screened to identify additional publications. Case reports and clinical studies addressing operative management of sternal fractures were included.
Epidemiology
Despite their clinical significance, sternal fractures account for less than 1% of all blunt trauma admissions. In a cohort of over 42,000 motor vehicle crash victims, only 0.64% sustained a sternal fracture [1]. Males are disproportionately affected, and incidence increases with age [6, 7].
Globally, the burden of sternal and rib fractures has risen steadily over the past 3 decades. East Asia, which comprises 22% of the world’s population, accounts for 28% of the global burden [7]. Projections indicate that both incidence and years lived with disability (YLDs) will continue to increase through 2030, with faster growth among females, gradually narrowing the historical gender gap [7].
Sternal fractures are frequently associated with other injuries sustained during blunt thoracic trauma. Reported co-injuries include rib fractures (28.3–69.9%), soft tissue contusions (56–57.5%), pulmonary contusions (18.8–37.2%), and haemothorax (3.4–34%). Mediastinal haematomas occur in about 33% of patients, while extremity fractures are seen in 28.8–31%. Other common concomitant injuries include traumatic brain injury (3.9–27.8%), pneumothorax (11.6–26.7%), thoracic vertebral fractures (7.4–21.6%), and flail chest (2.2–20.8%). Less frequent but clinically relevant associations include lumbar and cervical spine fractures, abdominal trauma, clavicle fractures, blunt cardiac injuries, pelvic fractures, scapular fractures, thoracic aortic injuries, cardiac lacerations, and cardiac tamponade [8].
Classification
Sternal fractures are generally classified into 2 categories: ISF, which are usually localised and relatively benign, and PSF, which involve significant extrasternal injuries and carry a higher risk of morbidity and mortality [9, 10]. Accurate differentiation between these groups is essential for guiding patient management and allocating resources appropriately [9, 11]. Key differences between ISF and PSF are summarised in Table I.
Table I
Comparison of isolated sternal fractures (ISF) and polytrauma-associated sternal fractures (PSF): clinical characteristics, management, and outcomes
Data from the National Israeli Trauma Registry, which included 1867 patients, revealed that those with isolated sternal fractures did not require endotracheal intubation, chest tube insertion, or thoracotomy, whereas 16.9% of polytrauma patients with sternal fractures required such interventions [9].
Fracture location and morphology also vary. The majority occur in the sternal body (55.8%), followed by the manubrium (31.7%), or involve both regions (12.5%) [8, 12]. Sternal body fractures are relatively evenly divided among transverse (31.7%), oblique (32.9%), and comminuted (35.4%) patterns, while the majority of manubrial fractures (75.5%) are oblique [12].
Mechanisms of injury and pathophysiology
Sternal fractures most commonly occur after a direct blow to the anterior chest wall or as a result of deceleration injuries in which the chest impacts the steering wheel or seatbelt. Motor vehicle collisions (MVCs) account for up to 68% of cases, followed by falls (7.9%), motorcycle accidents (7.9%), pedestrian-struck incidents (3.4%), and bicycle-related trauma (1.4%) [10]. The introduction of seatbelt legislation, particularly with shoulder restraints, has been associated with a higher incidence of sternal fractures [11, 13].
The biomechanics of injury depend on both the direction and magnitude of the applied force. The thorax plays a vital role in respiratory mechanics and organ protection [14]. Sternal fractures may result from direct forces, such as chest compression or localised impact against a steering wheel, blows to the chest in violent assaults, or even chest compressions during resuscitation. Seatbelt-related compression and entrapment injuries represent additional mechanisms [15, 16]. Indirect forces, including flexion, compression, hyperextension, or distraction, can also produce sternal fractures. A characteristic example is flexion–compression injury, often involving the manubriosternal joint, where the manubrium is displaced posteriorly [17, 18].
Fractures frequently involve the third to seventh ribs, and associated injuries such as clavicle or scapular fractures may alter the pattern of rib involvement, shifting it anteriorly or posteriorly [19]. Importantly, the sternum – together with the rib cage – constitutes a “fourth column” of thoracic stability, a concept particularly relevant when thoracic spine integrity is compromised [20, 21]. High-energy trauma may severely disrupt chest wall mechanics, leading to paradoxical motion, impaired ventilation, and respiratory failure, often necessitating surgical stabilisation [8, 22].
Clinical presentation and diagnostic approach
The hallmark symptom of sternal fracture is moderate to severe anterior chest pain, exacerbated by deep breathing or coughing. Dyspnoea may occur, particularly when coexisting with pulmonary contusion, pneumothorax, or haemothorax. Ecchymosis across the chest wall – known as the “seatbelt sign” – is another suggestive feature. On examination, findings typically include localised tenderness, bony crepitus, and, in unstable cases, chest wall paradox [10, 23]. Laboratory tests are generally nonspecific, although elevated cardiac enzymes may indicate concomitant blunt cardiac injury [10].
Imaging is essential for diagnosis. Portable chest X-ray (CXR) is often the initial modality, but its sensitivity is limited [24]. Point-of-care ultrasound is increasingly used for bedside evaluation, offering rapid detection of anterior cortical disruptions and step-off deformities [10]. Nevertheless, computed tomography (CT) remains the gold standard, with significantly higher sensitivity than lateral radiographs [24, 25]. In a large retrospective analysis of thoracic trauma, 94% of sternal fractures were detectable only by chest CT [25]. Furthermore, CT provides valuable information on associated intrathoracic injuries, which are present in over 80% of cases [25].
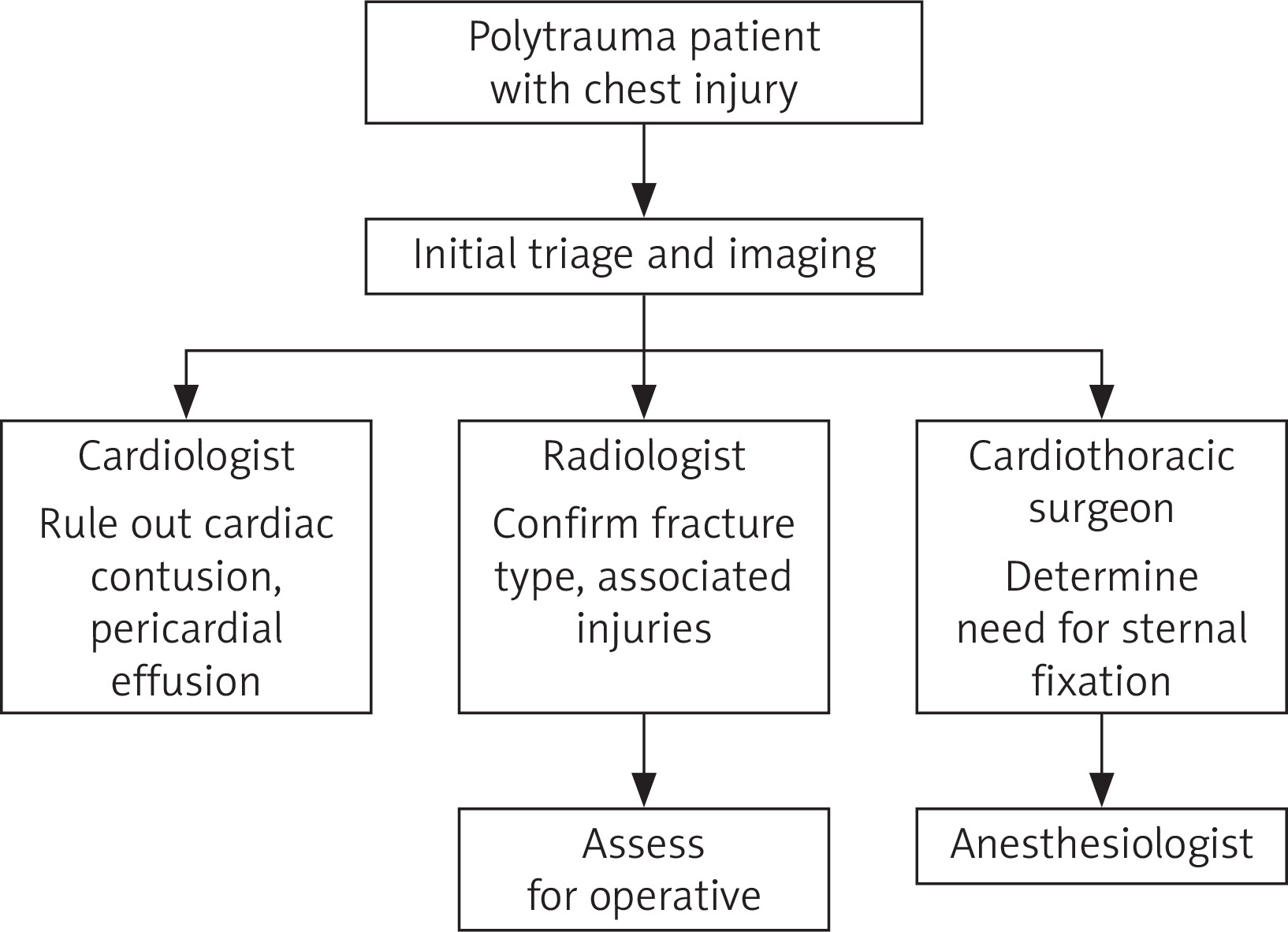
Of note, the degree of fracture displacement is not predictive of underlying cardiac injury, underscoring the importance of careful clinical assessment [26]. For polytrauma patients, a structured multidisciplinary approach is critical. Cardiology input is required to exclude myocardial contusion and pericardial effusion, radiology confirms the fracture type and co-injuries, and cardiothoracic surgery evaluates the need for fixation. Anaesthesiology involvement ensures preparedness for potential operative intervention. Such a systematic team-based strategy enables comprehensive evaluation and timely decision-making in complex thoracic trauma scenarios. The multidisciplinary evaluation pathway for polytrauma patients with chest injury is illustrated in Figure 3.
Figure 3
Multidisciplinary evaluation flowchart for polytrauma patients with chest injury. The algorithm outlines the stepwise approach from initial triage and imaging to specialist involvement. Key contributions include cardiology (exclusion of cardiac contusion and pericardial effusion), radiology (confirmation of fracture type and associated injuries), cardiothoracic surgery (assessment for fixation), and anaesthesiology (perioperative planning)
Conservative management
Most ISFs can be managed conservatively. The primary goals are as follows:
Adequate analgesia – essential to allow deep breathing and coughing, thereby preventing pulmonary complications. A multimodal approach is often employed, ranging from non-steroidal anti-inflammatory drugs to opioids and, in selected cases, regional anaesthesia (paravertebral or epidural blocks).
Respiratory support – incentive spirometry, physiotherapy, and early mobilisation are critical to maintain pulmonary function and reduce the risk of atelectasis or pneumonia [8, 27].
Early mobilisation and rehabilitation – mobilisation as soon as feasible reduces thromboembolic risk and accelerates recovery.
In a 13-year retrospective cohort, Klei et al. confirmed that conservative management with effective pain control is the treatment of choice for most patients with uncomplicated sternal fractures [27]. Other reviews have also emphasised that outpatient management is safe in stable patients without major associated injuries, while short inpatient observation may be appropriate in cases of severe pain, comorbidities, or suspected complications [8, 10].
Although the prognosis is usually favourable, rare but serious complications may arise. Retrosternal haematomas, for instance, may become secondarily infected, leading to purulent mediastinitis or sternal osteomyelitis, which require prolonged antibiotics and, at times, surgical debridement. Chronic pain, malunion, and nonunion are less common but recognised sequelae [28].
Surgical management
Historical perspective
The first report of surgical stabilisation dates back to 1943, when McKim used a Kirschner wire for fixation [29]. Since then, techniques have evolved from simple wiring to modern rigid plating systems designed to achieve reliable stability and promote healing.
Indications for surgery
Although partly surgeon-dependent, accepted indications for operative management include the following:
Unstable or displaced fractures – especially overlapping or malrotated fragments.
Chest wall instability – paradoxical motion or flail chest.
Symptom burden – intractable pain or respiratory insufficiency despite optimal conservative therapy.
Healing complications – malunion, nonunion, or pseudoarthrosis persisting beyond 6 weeks of conservative treatment.
Other considerations – cosmetic deformity, cardiac compression, or the need for rapid recovery in occupationally active individuals [30–36].
These criteria are supported by several systematic reviews and trauma guidelines [30] and are presented in Table II.
Table II
Criteria for operative management of sternal fractures: clinical, radiological, and patient-related considerations
Techniques and fixation materials
Various fixation materials have been reported, including stainless steel wires, absorbable plates (e.g. LactoSorb plating system) [37], non-absorbable plates (e.g. titanium plates), and internal cemented screws [10].
Wire cerclage: Historically, wire cerclage was the standard technique due to its simplicity and cost-effectiveness [38]. However, it may not provide sufficient stability in certain patient populations (e.g. in those with osteoporosis, because a weaker bone cannot hold wires effectively, or COPD due to chronic coughing putting extra stress on the sternum) [31]. It also poses several technical and physiological challenges. The limited operative space makes wire threading difficult, and periosteal dissection – often necessary during the procedure – can compromise the sternal blood supply, potentially affecting healing outcomes [39]. Lafci et al. present a modified Robicsek sternal closure technique, termed the “Double-check”, designed to improve stability and reduce complications such as dehiscence and infection after sternotomy. The method provides reinforced fixation, was applied successfully in their series, and is proposed as a simple and effective alternative for high-risk patients, although larger studies are needed to confirm its benefits [40].
Rigid plate fixation (RPF): Locking titanium plates and screws comprise the most widely accepted technique, which has gained popularity due to better mechanical support, reduced respiratory motion, lower postoperative pain, shorter hospitalisation time, and cost effectiveness [41]. Before performing surgery, a thorough patient evaluation is conducted along with a 3D reconstructed CT scan to obtain precise details about the shape and characteristics of the sternal fracture. Transverse and oblique fractures of the sternal body are stabilised using plates placed lengthwise along the sternum. In contrast, oblique fractures of the manubrium, sternocostal separations, and longitudinal fractures require transverse plating that spans from one rib, across the sternum, to the opposite rib for effective stabilisation [42]. While potentially beneficial for managing sternal fractures, this technique is often underutilised due to several challenges. These include complex preoperative planning, the risk of life-threatening mediastinal injuries or damage to retrosternal organs – particularly from deep drilling – and limited surgical training. The literature reports complication rates ranging from 10% to 19%, often requiring hardware removal [40]. While most surgeons favour an open repair, minimally invasive approaches have also been described [43]. Multiple retrospective cohorts report high union rates and favourable outcomes with plating [31, 36, 42].
Absorbable plating systems: These may be considered a viable option for the fixation of traumatic sternal fractures, given their low incidence of hardware failure, inflammation, and allergic reactions. These systems also offer the potential benefits of promoting osteogenesis and reducing operative time. Ricalde et al. conducted an in vitro study comparing the strength of 6 resorbable plating systems under pre- and post-heating conditions. Among them, Lacto Sorb showed the greatest mechanical strength, requiring the highest force to achieve a clinically significant displacement of 1–2 mm [44]. Ahmad et al. presented a case of surgical fixation of a traumatic transverse sternal fracture using an absorbable plate, which proceeded without complications. While this case supports the feasibility of absorbable plating in sternal trauma, further investigation and long-term studies are warranted to establish its efficacy and safety [37].
Hybrid fixation with bone graft: In cases of pseudoarthrosis or bone loss, bone grafting combined with plating has been employed to enhance bone healing, although this approach is technically demanding and less frequently used. The main surgical fixation techniques for sternal fractures, along with their materials, advantages, and disadvantages, are summarised in Table III.
Table III
Overview of surgical techniques for sternal fracture stabilisation, including fixation materials with associated benefits and limitations
Outcomes and limitations
Across reviews and case series, surgical fixation has demonstrated efficacy in restoring chest wall mechanics, improving respiratory function, and reducing prolonged hospital stays. A meta-analysis of sternotomy closure techniques also showed that rigid plating offers biomechanical advantages over wiring [38]. Reported complication rates for surgical fixation vary from 10% to 19%, most commonly due to wound infection, hardware migration, or the need for reoperation [40]. Careful patient selection, meticulous surgical technique, and rigorous infection control are critical to optimise outcomes.
Overall, rigid plate fixation has emerged as the most reliable method for unstable or complicated sternal fractures, although further prospective multicentre studies are needed to define clear operative criteria and long-term cost-effectiveness [30, 41].
Complications and postoperative course
Patients with sternal fractures are susceptible to a wide spectrum of complications, which may stem directly from the fracture or from associated injuries [10]. Acute complications include cardiac contusion, haemothorax, pneumothorax, mediastinal haematoma, and pericardial injury. Delayed complications may involve malunion, nonunion, chronic pain syndromes, infection, or osteomyelitis. In rare cases, retrosternal haematomas can become secondarily infected, serving as a bacterial nidus and progressing to purulent mediastinitis or sternal osteomyelitis [10, 45, 46].
Risk factors
Risk factors for complications can be grouped into 3 broad categories:
Patient-related: obesity, diabetes mellitus, chronic obstructive pulmonary disease (COPD), malnutrition, osteoporosis, and corticosteroid use.
Operative: prolonged surgical procedures, bilateral internal mammary artery harvesting, and suboptimal sternal closure techniques.
Postoperative: prolonged mechanical ventilation, reoperation, extended intensive care unit (ICU) stay, and cardiac massage [47, 48].
Among these, malnutrition represents a particularly important determinant because it significantly impairs wound healing and immune function. In elderly or immunocompromised patients, even seemingly mild infections can progress rapidly, increasing the risk of deep sternal wound infections and sepsis [28]. This aligns with findings in broader cardiothoracic surgery literature, where nutritional status strongly correlates with the incidence and severity of mediastinitis [47, 48].
Postoperative infection
Sternal wound infection is one of the most serious complications, with reported incidence rates ranging from 1% to 5% in cardiothoracic populations, but lower in isolated trauma cases [41]. Management strategies include targeted antibiotic therapy, aggressive surgical debridement, and adjunctive modalities such as VAC, which has demonstrated efficacy in reducing reinfection rates and improving wound healing times [28].
Future directions
Despite advances in diagnostic imaging, surgical techniques, and perioperative care, the optimal management of sternal fractures remains incompletely defined. Current evidence is largely derived from retrospective case series and small observational cohorts, with a marked absence of high-quality randomised or prospective multicentre studies [10, 27, 41].
Several areas warrant further investigation:
Operative criteria: There is no consensus regarding the exact thresholds for surgical stabilisation. While displacement, instability, and flail chest are commonly cited indications, practice remains highly surgeon dependent. Future multicentre prospective trials should aim to establish evidence-based guidelines that standardise operative decision-making across trauma centres [30, 49].
Fixation systems: Titanium plating is increasingly accepted as the gold standard for unstable or complicated fractures, but the long-term outcomes of absorbable plating systems remain poorly studied. Prospective research is needed to evaluate their biomechanical durability, complication rates, and patient-reported outcomes [37]. Comparative trials between absorbable and rigid fixation could clarify their roles in selected patient populations.
Cost-effectiveness: Surgical fixation, particularly with modern plating systems, carries higher upfront costs compared to conservative care. However, potential benefits such as reduced ventilator days, fewer pulmonary complications, and shorter hospital stays may offset expenses. Formal cost-effectiveness analyses in polytrauma populations would provide important insights for health systems [36, 41].
Patient-centred outcomes: Beyond radiographic healing, future studies should incorporate patient-reported outcome measures (PROMs), quality of life indices, and functional recovery endpoints. This is particularly relevant in younger and working-age patients, for whom rapid return to baseline activity is critical [42].
Multidisciplinary care pathways: Polytrauma patients with chest injuries often require coordination between trauma surgeons, cardiothoracic specialists, anaesthesiologists, and physiotherapists. The development and validation of standardised multidisciplinary care protocols could enhance early decision-making and improve outcomes [49, 50].
In summary, more prospective, multicentre trials are needed to define clear operative criteria, validate the long-term outcomes of both rigid and absorbable plating systems, and assess the cost-effectiveness of surgical versus conservative treatment in diverse trauma populations.
Limitations
This report has certain limitations. First, as a single case study, the findings cannot be generalised to the wider trauma population. Second, while a literature review was conducted to contextualise the case, the available evidence on sternal fracture management remains limited, with most data derived from retrospective series and small cohorts. Consequently, recommendations regarding operative versus conservative strategies are largely based on observational data and expert opinion rather than high-level evidence. Finally, long-term follow-up beyond the immediate postoperative period was not available in this case, which restricts conclusions regarding functional recovery and quality of life. Recognising the rarity but clinical importance of such injuries, we plan to collect and analyse additional similar cases to develop a larger case series that may offer more generalisable conclusions in future work.
Key clinical takeaways
Rigid plate fixation is biomechanically superior to wire cerclage and may reduce hospital stay in selected cases.
VAC therapy is an effective strategy for managing postoperative sternal wound infections.
Imaging with chest CT is essential, as standard X-rays miss a significant number of sternal fractures.
Careful patient selection and timing are critical for operative success.
Conclusions
Sternal fractures, although uncommon, can pose significant challenges in trauma care, particularly when occurring in the context of polytrauma or chest wall instability. Accurate diagnosis, guided by clinical vigilance and appropriate imaging – most reliably chest CT – is essential for timely management. While conservative therapy remains sufficient for the majority of isolated fractures, surgical stabilisation should be considered in cases of displacement, instability, or complications. Rigid plate fixation provides clear biomechanical advantages over traditional wire cerclage and may facilitate improved recovery, earlier mobilisation, and reduced hospital stay in appropriately selected patients. Nonetheless, evidence remains limited, and further research is needed to refine operative criteria, optimise fixation strategies, and minimise postoperative complications in high-risk populations. Ultimately, sternal fractures in polytrauma patients require comprehensive evaluation, multidisciplinary collaboration, and timely decision-making. In unstable cases, surgical stabilisation can be decisive, offering not only structural restoration but also the potential for life-altering improvement in outcomes.









