
Purpose
Medical use of ionizing radiation began at the end of the 19th century, following the discovery of X-rays in 1895 and radioactive isotopes shortly thereafter [1]. Early applications of radiation therapy rapidly expanded to cancer treatment, including the prostate. The first report of permanent radioactive seed implantation in the prostate was published in the early 20th century, when technical limitations and the lack of image guidance restricted precision and reproducibility [2-4].
Over the past four decades, major technological advances have transformed prostate brachytherapy into a highly precise and minimally invasive technique. The introduction of transrectal ultrasound guidance improved treatment planning systems, and standardized dosimetric constraints enabled safe and effective permanent low-dose-rate (LDR) brachytherapy techniques [5-7]. By the early 21st century, high-quality clinical evidence had established LDR brachytherapy as an effective treatment option, either as monotherapy for low- and favorable intermediate-risk prostate cancer or as a boost combined with external beam radiation therapy (EBRT) for unfavorable intermediate- and high-risk disease [8, 9]. In higher risk patients, androgen deprivation therapy (ADT) was commonly incorporated to enhance disease control [10, 11].
Permanent seed brachytherapy allows delivery of high radiation doses with a steep dose gradient, resulting in effective tumor coverage while limiting radiation exposure to adjacent organs at risk, including the rectum, bladder, urethra, and penile bulb. This dosimetric advantage translates into high disease control rates with a favorable toxicity profile, particularly for patients who are not ideal surgical candidates [12]. In addition, LDR brachytherapy has gained increasing interest as a salvage treatment option for selected patients with locally recurrent disease after prior radiotherapy [13].
Currently, LDR brachytherapy is widely recognized as a safe, effective, and well-tolerated treatment modality. Major international clinical guidelines recommend its use as definitive monotherapy for low- and favorable intermediate-risk prostate cancer, and as a brachytherapy boost combined with EBRT, often with ADT, for unfavorable intermediate- and high-risk disease [14]. Monotherapy is generally associated with lower rates of late gastrointestinal and genitourinary toxicity, whereas combined treatment strategies may increase toxicity but offer improved disease control in higher risk settings. Definitive treatment is typically recommended for patients with a life expectancy greater than 10 years in low- and intermediate-risk disease, and greater than 5 years in high-risk cases [15].
Despite this robust evidence base, the use of permanent seed prostate brachytherapy remains limited and is concentrated in a small number of specialized centers. Limited referral patterns and persistent concerns regarding toxicity and effectiveness may contribute to its underutilization, highlighting the need for real-world data from large institutional cohorts.
Material and methods
This retrospective cohort study included 805 patients with prostate cancer who underwent permanent implantation of iodine-125 (125I) seeds between 2008 and 2023. The study was approved by the Ethics Committee of Faculdade São Leopoldo Mandic (approval number 7.371.139; CAAE: 82100824.1.0000.5374), and conducted in accordance with the Declaration of Helsinki. Patients were stratified into risk groups according to the D’Amico classification [16]. A total of 394 patients (48.9%) were classified as low risk, 303 (37.6%) as intermediate risk, and 108 (13.4%) as high risk. Risk stratification was based on prostate-specific antigen levels, Gleason score, and clinical stage at diagnosis. Low-risk patients were treated with brachytherapy alone, whereas intermediate- and high-risk patients received combined brachytherapy with EBRT (50 Gy). Androgen deprivation therapy was administered for 6 months in intermediate-risk patients and for 18-36 months in high-risk patients, according to institutional practice. The prescribed brachytherapy dose was 145 Gy for monotherapy and 110 Gy when combined with EBRT. Staging imaging was performed as per baseline risk category. Low-risk patients typically underwent transrectal ultrasound and multiparametric magnetic resonance imaging (MRI), usually performed during diagnostic workup prior to biopsy. Intermediate-risk patients underwent MRI and bone scintigraphy. High-risk patients underwent MRI and bone scintigraphy, with computed tomography (CT) or prostate-specific membrane antigen positron emission tomography (PSMA-PET) done in selected cases, depending on clinical indication and availability. Permanent seed brachytherapy was performed as an outpatient procedure, without hospital admission. All patients underwent pre-procedural clinical assessment, including laboratory evaluation and cardiological assessment for anesthetic risk stratification. Procedures were conducted under general anesthesia, with patients positioned in the dorsal lithotomy position. After standard aseptic and antiseptic preparation, urinary catheterization was performed. A transrectal ultrasound probe was inserted and externally fixed to a stepper device, integrated with a perineal template to guide needle placement. Ultrasound images were acquired and transferred to treatment planning system. The prostate and organs at risk were contoured by a radiation oncologist. Treatment planning, including seed distribution and dosimetric optimization, was performed by a medical physicist. Final plan approval and dose prescription were confirmed by the radiation oncologist prior to implantation. Stranded 125I seeds were used in all standard cases; unstranded seeds were reserved for selected situations requiring focal adjustment. Seeds were implanted via transperineal needles under real-time ultrasound guidance. The entire procedure had a mean duration of approximately 100 minutes. Post-anesthesia recovery lasted around 90 minutes, after which patients were discharged home on the same day.
Post-implant dosimetric evaluation was performed using pelvic CT, acquired 15 days after implantation to assess seed distribution and target coverage. Volumetric dose parameters, such as D0.1cc for the urethra and rectum, were not prospectively recorded in the study database. However, treatment planning was performed according to institutional dosimetric constraints, and plan review confirmed that urethral D0.1cc was maintained below 150% and rectal D0.1cc below 100% of the prescribed dose.
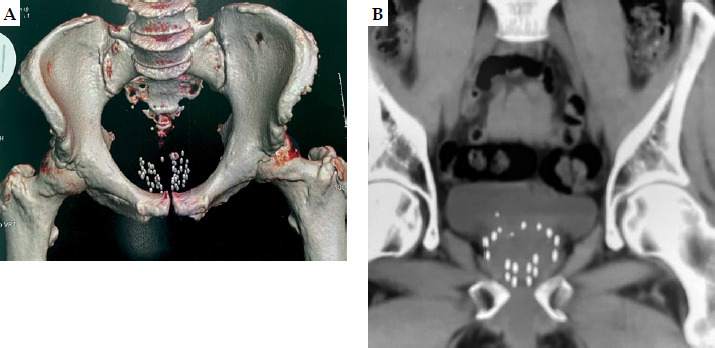
Figure 1A illustrates a three-dimensional reconstruction of pelvic anatomy used for spatial assessment of seed placement, while Figure 1B demonstrates a coronal CT scan used for dosimetric analysis.
Fig. 1
A) Three-dimensional reconstruction of pelvic anatomy used for spatial assessment of seed placement. B) Coronal computed tomography (CT) scan showing post-implant seed distribution used for dosimetric evaluation
Patients were followed up every 3-6 months during the first 3 years after implantation, every 6-12 months between years 3 and 5, and annually thereafter. Each follow-up visit included clinical evaluation, serum prostate-specific antigen (PSA) measurement, and structured assessment of treatment-related toxicity. Genitourinary and gastrointestinal toxicities were graded according to the RTOG/EORTC toxicity criteria, with acute toxicity defined as events occurring within 90 days after treatment and late toxicity described as events occurring thereafter. Erectile function was assessed through patient-reported symptoms during follow-up visits. Biochemical recurrence was defined according to the Phoenix criteria, as a PSA increase of ≥ 2.0 ng/ml above the nadir value [17]. All analyses were performed using the available sample size for each variable (complete-case analysis), without imputation for missing data.
Statistical analysis
Statistical analyses were conducted by a dedicated biostatistician using validated statistical software. Descriptive analyses included frequency tables for categorical variables, and measures of central tendency and dispersion for numerical variables. Group comparisons of categorical variables were performed using chi-square test or Fisher’s exact test, as appropriate. Mann-Whitney U test was used to compare continuous variables between two groups. Spearman’s rank correlation coefficient was employed to measure associations between continuous variables. Changes in symptom proportions over time were evaluated using McNemar’s test or symmetry test. Survival analyses were performed using Kaplan-Meier method, and survival curves were compared using Wilcoxon (Breslow) test, which provides greater weight to early events. Cox proportional hazards regression analysis was done to explore factors associated with biochemical relapse. Variables were first evaluated in univariate models and subsequently entered into a multivariable model. Due to missing values in some covariates, the final multivariable model included 643 patients. Treatment modality and risk group were carefully evaluated due to their strong clinical correlation with treatment allocation. A two-sided significance level of 5% was adopted for all statistical analyses. Kaplan-Meier curves were generated using the available number of patients for each analysis, and censoring was appropriately applied at the time of last follow-up or competing events.
Results
A total of 805 patients underwent permanent 125I seed brachytherapy; monotherapy was delivered to 494 patients (61.4%), whereas 311 (38.6%) received combined treatment with EBRT. Salvage brachytherapy was performed in 8 patients (1.0%), and ADT was administered in 353 cases (43.9%). The mean age was 65.1 years (range, 39-92 years), with a mean PSA level of 7.1 ng/ml and a mean prostate volume of 31.3 cc. According to the D’Amico risk classification, 394 patients (48.9%) were categorized as low risk, 303 (37.6%) as intermediate risk, and 108 (13.4%) as high risk. The baseline patient and treatment characteristics are summarized in Table 1.
Table 1
Patient and treatment characteristics
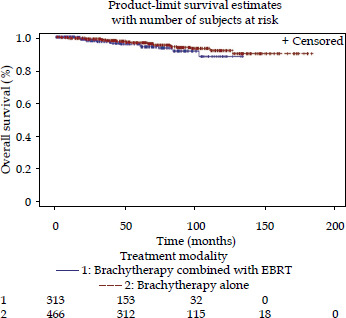
The median follow-up for the entire cohort was 64.2 months (range, 0.8-183.7 months), and overall survival (OS) at last follow-up was 95.4%. When analyzed by risk group, OS was 95.3% for low-risk, 95.9% for intermediate-risk, and 94.2% for high-risk patients. The Kaplan-Meier analysis demonstrated no statistically significant differences in OS among risk groups (p = 0.3619, Figure 2). Overall survival was also comparable between patients treated with monotherapy and those receiving combined therapy (mean survival 122.1 vs. 98.5 months, respectively, p = 0.3764, Figure 3).
Fig. 2
Kaplan-Meier curves showing overall survival (OS) stratified by D’Amico risk groups (low, intermediate, and high). No statistically significant difference was observed between groups (p = 0.3619, Wilcoxon test)
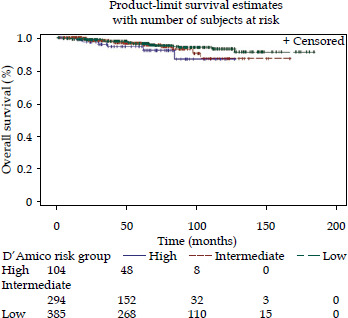
Fig. 3
Kaplan-Meier curves showing overall survival (OS) according to treatment type (brachytherapy monotherapy vs. combined treatment with external beam radiation therapy [EBRT]). No statistically significant difference was observed between groups (p = 0.3764, Wilcoxon test)
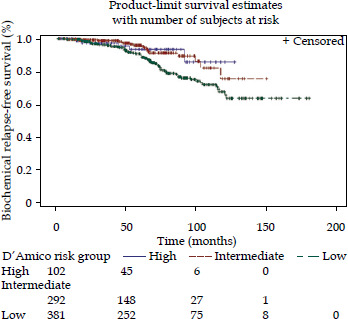
Biochemical recurrence was observed in 88 patients (11.3%). Time-to-event analyses were performed using the Kaplan-Meier method, with appropriate censoring at last follow-up or death from other causes. Among these events, 14 (1.7%) occurred within the first 5 years, 18 (2.4%) between 5 and 10 years, and 56 (7.0%) at later or unspecified time-points. The 5-year biochemical relapse-free survival (bRFS) rate for the overall cohort was 92.1%. Five-year bRFS rates by risk group were 95.3% for low-risk, 96.0% for intermediate-risk, and 94.3% for high-risk patients. The mean bRFS was 108.2 months. Biochemical relapse-free survival was numerically higher in patients receiving combined therapy (94.3%) compared with monotherapy (85.3%), although this difference was not statistically significant (p = 0.1134, Figure 4). A statistically significant difference in bRFS was observed among risk groups (p = 0.0151, Figure 5). Interestingly, patients classified as low risk demonstrated numerically lower biochemical relapse-free survival compared with intermediate- and high-risk groups. This unexpected finding may be related to treatment selection bias, differences in treatment intensification (e.g., use of EBRT and ADT), or limitations inherent to retrospective risk stratification. Patients who developed biochemical failure had significantly higher PSA nadir values (p = 0.0054).
Fig. 4
Kaplan-Meier curves showing biochemical relapse-free survival (bRFS) according to treatment type. No statistically significant difference was observed between groups (p = 0.1134, Wilcoxon test)
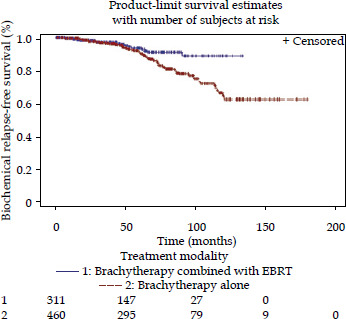
Fig. 5
Kaplan-Meier curves showing biochemical relapse- free survival (bRFS) stratified by D’Amico risk groups (low, intermediate, and high). A statistically significant difference was observed between groups (p = 0.0151, Wilcoxon test)
During follow-up, 43 patients (5.3%) died; only two deaths (0.2%) were attributed to prostate cancer, eight deaths (1.0%) were related to second malignancies, while 33 deaths (4.1%) resulted from causes unrelated to prostate cancer.
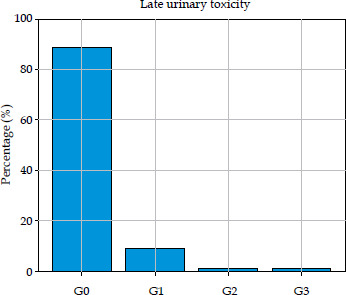
Treatment-related toxicity was assessed cumulatively per patient throughout follow-up, considering the highest grade recorded for each toxicity category. Acute gastrointestinal (GI) grade 1-2 toxicity occurred in 3.4% of patients, while acute genitourinary (GU) grade 1-2 toxicity was observed in 41.0%. Late GI and GU grade 1-2 toxicities were reported in 1.6% and 10.3% of patients, respectively. Late grade 3 GU toxicity occurred in 1.0% of patients, and no grade 4 or 5 toxicities were observed (Figures 6-9).
Fig. 6
Distribution of acute genitourinary (GU) toxicity (grade, 0-3). Most patients experienced no symptoms (57.3%) or only mild indications (37.9%)
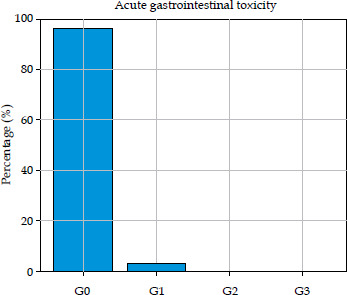
Fig. 7
Distribution of late genitourinary (GU) toxicity (> 6 months post-implant). Absence of symptoms was observed in 88.7% of patients; moderate and severe events were rare (1.0% each)
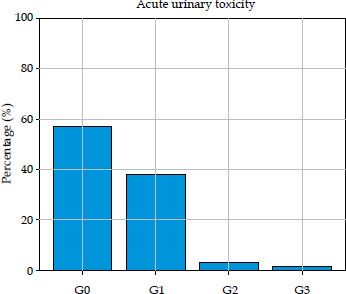
Fig. 8
Distribution of acute gastrointestinal (GI) toxicity. The vast majority of patients (96.4%) presented no symptoms; grade 2-3 events were infrequent (0.6%)
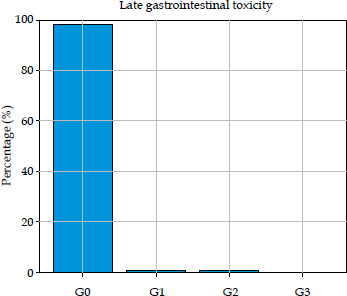
Fig. 9
Distribution of late gastrointestinal (GI) toxicity. Symptoms were rare and mild; only 0.7% of patients experienced moderate symptoms, and no severe events were recorded
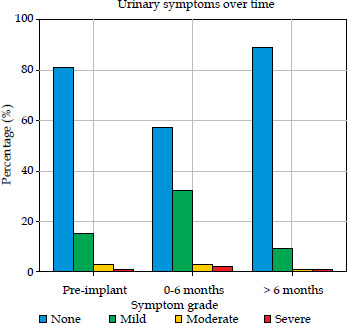
Regarding urinary symptoms, 80.8% of patients were asymptomatic prior to implantation, and 15.2% reported mild symptoms. During the acute phase (0-6 months post-implantation), the proportion of patients with mild urinary symptoms increased to 37.9%, while 4.8% reported moderate to severe symptoms. After 6 months, urinary symptoms improved substantially, with 88.7% of patients having no symptoms and only 2.0% reporting moderate to severe complaints (p < 0.0001, Figure 10).
Fig. 10
Temporal evolution of urinary symptoms (pre-implant, 0-6 months, and > 6 months). Mild symptoms increased during acute phase and significantly improved after 6 months (p < 0.0001, symmetry test)
Erectile function data were inconsistently reported and therefore analyzed descriptively. Based on available information, no clear deterioration in erectile function was observed following treatment.
Eight patients underwent salvage brachytherapy for locally recurrent disease after prior radiotherapy. Their mean age was 70.6 years. Five patients were initially classified as low risk and three as high risk. The mean urethral and rectal doses were 117.8 Gy and 63.2 Gy, respectively. After salvage treatment, seven patients remained disease-free at last follow-up, while one experienced biochemical failure. Post-treatment urinary symptoms were absent in six patients and mild in one. Given the small number of salvage cases, these results were presented descriptively without statistical comparison.
Discussion
Comparative studies evaluating radical prostatectomy, permanent seed brachytherapy, and EBRT, have demonstrated similar oncologic outcomes, although with distinct toxicity and functional profiles. Brachytherapy is consistently associated with lower rates of urinary incontinence, whereas surgical approaches may result in less acute urinary irritation [18-20]. It should be acknowledged that nearly half of the patients in our cohort were classified as low risk, a group known to have excellent long-term oncologic outcomes regardless of treatment modality. This cohort characteristic should be considered when interpreting the favorable survival outcomes observed in the present study.
Large contemporary cohorts with extended follow-up have confirmed the long-term effectiveness of permanent seed implantation, both as definitive monotherapy and as a boost combined with EBRT. In a large cohort of nearly 3,000 patients, permanent seed brachytherapy achieved durable cancer control with favorable functional outcomes [21]. Patients treated with brachytherapy generally report better urinary continence and erectile function compared with those undergoing radical prostatectomy, including nerve-sparing robotic techniques. Transient urinary obstructive symptoms may occur after implantation, whereas gastrointestinal toxicity is more commonly associated with EBRT [22].
Although surgery is frequently offered to younger patients, permanent seed brachytherapy has demonstrated excellent oncologic outcomes in this population. Langley et al. reported 10-year cancer-specific survival rates ranging from 95% to 100%, with preservation of erectile function in approximately 75% of patients at 5 years [23-28]. Our results are consistent with these findings; among 229 patients younger than 60 years old, the overall survival was 96.1%, with no prostate cancer-related deaths recorded.
Erectile function was not systematically assessed using validated questionnaires in our retrospective cohort. However, clinical follow-up suggested preservation of erectile function in most patients with favorable baseline status. Due to the lack of standardized assessment tools, definitive conclusions regarding sexual outcomes cannot be drawn, and these findings should be interpreted cautiously.
When used as monotherapy for low- and intermediate-risk disease, permanent seed brachytherapy provides excellent long-term biochemical disease control. Routman et al. reported 10-year biochemical control rates of 92% for low-risk and 76% for intermediate-risk patients [29]. In the present cohort, intermediate-risk patients demonstrated biochemical control rates comparable to or slightly higher than those observed in low-risk patients. The finding of lower biochemical control in low-risk patients compared with higher-risk groups is counterintuitive. This unexpected finding likely reflects treatment-related confounding, as intermediate- and high-risk patients more frequently received combined modality treatment, including EBRT and ADT, which may have contributed to improved biochemical control compared with brachytherapy alone in low-risk patients. These results highlight the limitations of retrospective comparisons across heterogeneous treatment strategies.
Although differences were not statistically significant, patients who developed biochemical recurrence exhibited significantly higher PSA nadir and last PSA values, consistent with established prognostic markers.
Beyond its local oncologic efficacy, brachytherapy has been hypothesized to exert immunomodulatory effects. Increases in peripheral CD3 and CD4 T-cell counts following treatment have been reported [30]. Population-based studies have suggested similar or favorable overall survival rates compared with age-matched controls, raising the possibility of a broader systemic effect [31, 32]. In the present cohort, late grade ≥ 2 clinically significant genitourinary toxicity occurred in 2.0% of patients, while late gastrointestinal toxicity was observed in only 0.7%, with no grade ≥ 3 gastrointestinal events reported.
For unfavorable intermediate- and high-risk disease, the combination of EBRT and brachytherapy delivers a high biologically effective dose (BED), often exceeding 200 Gy, which has been associated with improved biochemical control and reduced prostate cancer-specific mortality [33]. Several contemporary studies have demonstrated superior outcomes with combined therapy compared with EBRT alone in these risk groups [34, 35]. In our series, patients treated with brachytherapy boost achieved numerically higher biochemical relapse-free survival compared with monotherapy, although this difference did not reach statistical significance, likely reflecting treatment heterogeneity and limited event numbers. In our institutional protocol, treatment allocation is largely determined by baseline disease risk according to the D’Amico classification. Consequently, treatment modality and risk group are closely related variables, which may introduce collinearity in multivariable models and limit the ability to fully separate their independent effects.
Concerns regarding the feasibility and toxicity of brachytherapy in patients with prior transurethral resection of the prostate (TURP) have diminished over time. Multiple studies have demonstrated acceptable toxicity profiles and preserved oncologic outcomes in this setting [36, 37]. In our cohort, 94 patients who had undergone prior TURP were treated with brachytherapy without increased genitourinary or gastrointestinal toxicity, supporting safety of this approach in appropriately selected patients.
Partial-gland brachytherapy has been proposed as a strategy to reduce toxicity, particularly in salvage settings following prior radiotherapy [38]. Current recommendations emphasize careful patient selection, adequate interval from primary treatment, advanced imaging, and histological confirmation [39]. In this study, partial-gland implantation was employed in selected salvage cases, with favorable short-term outcomes and no unexpected toxicity. Given the small number of salvage patients, these results should be regarded as hypothesis-generating rather than definitive.
Late toxicity remains a critical consideration in radiation therapy. In our cohort, toxicity rates were low, with no grade ≥ 3 gastrointestinal events observed. These rates compare favorably with a published study, in which late toxicity following permanent seed implantation has generally been reported as ≤ 10% [40]. Seed migration was not observed, consistent with the use of stranded seeds [41]. Rectal bleeding occurred in 0.6% of patients, and all cases were mild to moderate in severity. This incidence is notably lower than rates reported in some combined-modality series, where rectal bleeding rates up to 12% have been described [42]. Careful image-guided planning and adherence to rectal dose constraints likely contributed to these favorable outcomes. Although follow-up duration was reported for the overall cohort, the retrospective nature of the study and heterogeneity of treatment modalities precluded uniform stratification of follow-up by risk group and treatment approach. Nevertheless, the observed durability of disease control in intermediate- and high-risk patients, together with the low incidence of late grade ≥ 2 toxicity, supports the long-term safety and clinical relevance of permanent seed brachytherapy in appropriately selected patients.
Several limitations of this study should be acknowledged, including its retrospective design, potential selection bias, and incomplete data on various clinical variables, particularly erectile function and comorbidity profiles. Treatment heterogeneity across risk groups, including variable use and duration of ADT and EBRT, limits causal interpretation and direct comparison between treatment strategies. Risk-stratified biochemical recurrence-free survival and metastasis-free survival analyses were not uniformly available, further underscoring the need for careful interpretation. In addition, although multivariable Cox regression was performed, the interpretation of these results should be cautious due to the correlation between treatment modality and baseline risk group as well as the reduction in sample size in the final model. Despite these limitations, this large single-institution series demonstrates that permanent seed brachytherapy provides durable disease control with a very low incidence of clinically significant late toxicity. These findings support the continued role of permanent seed brachytherapy as an effective and versatile treatment option for localized prostate cancer, whether used as monotherapy, as a boost combined with EBRT, or in carefully selected salvage settings.
Conclusions
Permanent seed brachytherapy is an effective and well-tolerated treatment option for localized prostate cancer across different risk groups. The present findings demonstrate durable oncologic outcomes and a very low incidence of clinically significant late toxicity, supporting its continued role as a definitive treatment modality. In carefully selected patients, including younger individuals and selected cases of local recurrence, permanent seed brachytherapy represents a valuable therapeutic option when performed by experienced multidisciplinary team.








