
INTRODUCTION
The transformation of Poland’s mental health care system, initiated through the pilot program of Community Mental Health Centers (MHCs), represents one of the most significant structural reforms in public psychia-try in recent decades. Officially launched in 2018 under the National Mental Health Protection Program (Narodowy Program Ochrony Zdrowia Psychicznego – NPOZP), the reform aims to shift psychiatric care from large, hospital- based institutions toward a decentralized, community- oriented model emphasizing accessibility, continuity, and integration across medical and social sectors [1-3].
The MHC model integrates multiple levels of care – inpatient wards, day units, outpatient clinics, and mobile community teams – into a coherent, locally managed system offering comprehensive, person-centred support. Registration and Coordination Points (RCPs) within each center enable immediate access to mental health professionals without a referral, supporting early triage and continuity of care [4-6].
Recent national evaluations indicate that the implementation of MHCs has led to improved service accessibility, better coordination, and higher patient satisfaction compared with traditional models [3, 7-9]. Studies by Biechowska et al. [7] and Kiejna et al. [8] demonstrated an enhanced availability of outpatient services and reduced hospitalization rates following the introduction of the pilot scheme. Similarly, Hat et al. [9] found greater patient satisfaction in the community- based model compared with institutional settings. At the regulatory level, the pilot’s architecture and center functions are defined by the 2018 Ministerial Regulation and subsequent Ministry of Health guidance [4, 5]. At the same time, disparities in regional infrastructure, staffing, and resource allocation persist, underscoring the importance of evaluating local implementation outcomes [3, 7-9]. The 2025 volume of Psychiatria Środowiskowa, edited by Wciórka and Cechnicki, emphasizes that the success of the CZP model depends not only on infrastructure but also on effective multidisciplinary collaboration, integration with primary and social care, and responsiveness to community needs [1, 2]. These directions are consistent with the Recommendations of the Mental Health Congress Working Group for systemic changes in adult psychiatric care [6].
This study aims to explore the ways in which the principles of the national community psychiatry reform have been implemented at a local level. Focusing on MHC operating in the Malbork and Sztum counties, the paper analyses quantitative data from 2023 (prior to the establishment of the MHCs) and 2024 (after one full year of their operation). It examines changes in the most common psychiatric diagnoses, total patient numbers, first-time patient numbers, the overall number of services provided and the structure of these services. The findings contribute to the growing body of knowledge on the practical outcomes of the mental healthcare reform in Poland, offering evidence-based insights into the effectiveness of the community-based model at county level.
METHODS
Study setting and organizational framework
The MHC in the Malbork and Sztum counties was established in January 2024, based on two long-standing outpatient psychiatric clinics that had operated locally for over 25 years. Before implementation, mental health care in this region was limited to traditional outpatient services, with no local day-care or community-based programs. The two counties, with a combined adult population of 81,038, did not have their own psychiatric inpa- tient ward. Patients requiring hospitalization were referred to neighboring facilities – the 800-bed regional psychiatric hospital in Starogard Gdański and a 35-bed psychiatric ward in Prabuty, managed by the same organization that operates the local MHC [10]. This organizational linkage supports coordination between outpatient and inpatient services, particularly in post-discharge follow-up.
Following implementation, new units – the RCP, a psy-chiatric day ward, and mobile community teams – were launched, integrating outpatient, day-care, and community services within a single local network. Patients are assigned to a multidisciplinary team responsible for individualized treatment and crisis intervention. In its first year, the center provided care to 4,146 individuals (5.12% of the adult population). Staff capacity increased from approximately 8 to 12 full-time equivalents (FTE), mainly due to the establishment of new units and the introduction of 24-hour coverage; night and weekend duties accounted for only a small proportion of interventions. As a Type B center, the MHC did not collect comprehensive data on hospitalization; however, National Health Fund (NFZ) reports indicated a decline in psychiatric inpatient days in the region, with budget deductions for patient migration remaining below 30% in 2024.
Data and analysis
The dataset includes all visits by adult patients registered with the local healthcare system between 1 January 2023 and 31 December 2024. Data analysis was performed in Python, using standard tools for data processing (pandas) and visualization (matplotlib) in the Jupyter Notebook environment. The analytical process included the following: calculation of the total number of patients and first-time patients (defined as individuals not recorded in the 2023 dataset); grouping and aggregation of medical services by category (psychiatric consultations, psychotherapy, psychological consultations, and registration point services coded as ICD-10 Z03); consolidation of selected community-based services with the doctor visit category; identification of the seven most common first-time diagnoses based on the primary ICD-10 code (counting only the first occurrence per patient); and the visualization of monthly person-days in the psychiatric day ward in 2024. All tables and charts were created based on raw data, with no statistical modelling techniques, such as interrupted time series analysis, applied.
The analysis aimed to illustrate structural changes in patient profiles and service types following the implementation of the MHC model in the two counties. The dataset was fully anonymized and did not contain any personally identifiable or sensitive information, in full compliance with applicable data protection standards. The analysis involved calculating descriptive statistics to assess changes in service delivery and patient characteristics between 2023 and 2024. Key metrics included the number of patients, new (first-time) patients, service types, and diagnostic categories. These data were analyzed in terms of absolute values and percentage changes and were visualized using bar charts to illustrate emerging trends. Inferential statistical tests, such as those for statistical significance or regression models, were not applied. This decision reflects both the exploratory nature of the study and the characteri-stics of the dataset. Year-to-year comparisons in this context are based on aggregated service data from two consecutive time periods, which are subject to local contextual factors and potential seasonality. Given these constraints, formal significance testing would have limited interpretive value. Instead, the focus was placed on descriptive comparisons in order to identify observable shifts associated with the implementation of the MHC model.
RESULTS
Total and first-time patient numbers
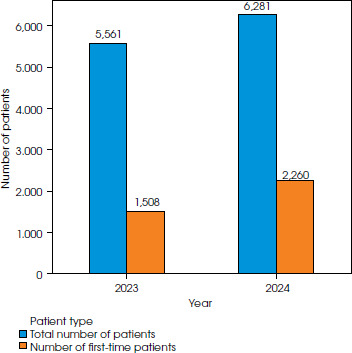
Figure I shows the number of patients in the Malbork and Sztum counties in 2023 and 2024. The total number of patients increased by approximately 12.9%, rising from 5,561 in 2023 to 6,281 in 2024. The number of first-time patients increased from 1,508 to 2,260, representing a rise of around 49.8%.
Number of services by type
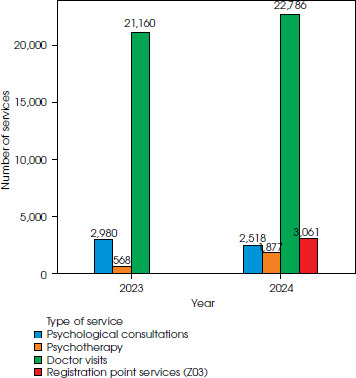
Figure II shows the distribution of services provided by type in 2023 and 2024. The data show a significant increase in the number of psychotherapy sessions, which rose from 568 in 2023 to 1,877 in 2024 – an increase of around 230.5%. There was also a notable increase in registration point services (coded under ICD-10 Z03), which were introduced in 2024 and totalled 3,061. The number of doctor visits increased from 21,160 in 2023 to 22,786 in 2024, representing growth of around 7.7%. Conversely, the number of psychological consultations decreased from 2,980 in 2023 to 2,518 in 2024.
Total number of services
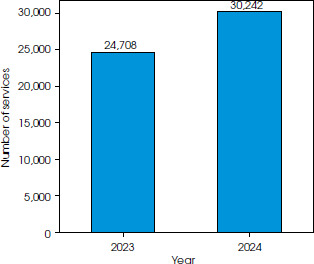
Figure III illustrates the total number of services provided in 2023 and 2024. There was an increase in the number of services from 24,708 in 2023 to 30,242 in 2024, representing a rise of approximately 22.4%.
Most common first-time diagnoses
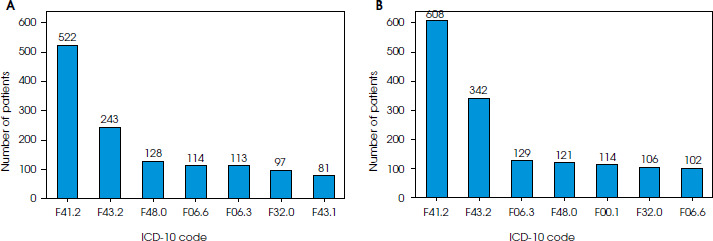
Figure IV shows the seven most frequently made first- time diagnoses in 2023 and 2024. The total number of these within the categories below increased by appro-ximately 17.3%, rising from 1,298 in 2023 to 1,522 in 2024. The most common diagnoses in both years were F41.2 (mixed anxiety and depressive disorders) and F43.2 (adjustment disorders), with increases of 16.5% (from 522 to 608 cases) and 40.7% (from 243 to 342 cases), respectively. In 2024, the F00.1 diagnostic code (dementia in late-onset Alzheimer’s disease) appeared among the most frequent diagnoses, with 114 cases recorded, whereas it was not among the top categories in 2023. Conversely, the number of diagnoses under F43.1 (post-traumatic stress disorder) decreased from 81 to below the top seven most frequent categories in 2024.
Use of the Day Ward
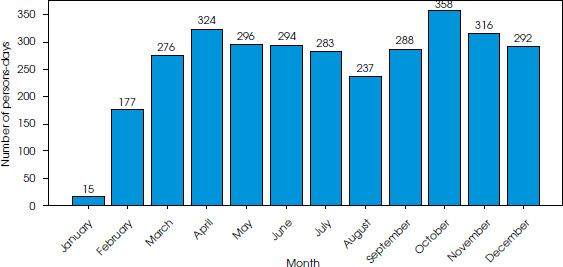
Figure V shows the monthly number of person-days in the Day Ward in 2024. A consistent increase was observed from January to October, with the number of person- days rising from 15 in January to a peak of 358 in October. Between January and April, the number increased by a factor of over twenty. From May onwards, the monthly values remained relatively stable, fluctuating between 237 and 358 person-days, and remained high until the end of the year.
DISCUSSION
General trends following the implementation of the MHC model
The implementation of the MHC model in the Malbork and Sztum counties in 2024 was accompanied by several significant changes in the structure and provision of mental health services. We observed a 12.9% increase in the total number of patients, a 49.8% increase in individuals initiat-ing psychiatric treatment within the MHC system, and a 22.4% rise in the total number of services compared to 2023. The most pronounced growth concerned psychothe-rapy sessions (+230.5%) and initial diagnostic assessments coded Z03 (preliminary medical observation). Meanwhile, psychological consultations declined by 15.5%.
Furthermore, the number of patients who received psychiatric diagnoses for the first time within the seven most common ICD-10 categories increased by 17.3%, with F41.2 and F43.2 remaining the most frequently recorded categories in both years. In 2024, the diagnosis of F00.1 (dementia in Alzheimer’s disease with late onset) appeared among the seven most prevalently assigned dia-gnoses, while F43.1 (post-traumatic stress disorder) was no longer among the most frequently recorded diagnostic categories. Notably, the psychiatric day ward – introduced as part of the CZP model in 2024 – showed a steady and progressive increase in use throughout the year.
These trends are consistent with the core objectives of the psychiatric care reform in Poland, particularly those related to improving access to community-based services for individuals seeking mental health support. The observed increases indicate an enhanced availability and responsiveness of care following the implementation of the MHC model. These findings align with early evaluations of the reform by Sagan et al. [3] and Biechowska et al. [7], which emphasized improved access, engagement, and flexible treatment pathways in community programs.
As highlighted in the expert report Priority Actions in the Field of Mental Health for the Years 2016-2020 [11] and in the Recommendations of the Mental Health Congress Working Group [6], local authorities are key actors in implementing mental health strategies at the community level. This perspective is consistent with the principles outlined by Wciórka and Cechnicki, who emphasize that the success of the reform depends on multidisciplinary collaboration, territorial responsibility, and integration of services across the medical, social, and educational sectors [1, 2]. The development of MHCs and RCPs directly reflects this strategic vision by fostering integrated, accessible, and patient-centred care [4, 5, 6]. Taken together, these findings demonstrate a dynamic structural reorganization and expansion of services during the first year of MHC implementation, which is consistent with both national policy objectives and the broader European deinstitutionalization framework.
Role of registration and coordination points
The marked increase in the number of diagnoses classified under ICD-10 code Z03 further underscores the importance of RCPs, which function as the primary point of contact for individuals seeking mental health care without a formal referral. Within these units, appropriately qualified clinical staff conduct initial assessments and use the Z03 code to record preliminary medical observation and evaluation when a definitive diagnosis has not yet been established.
Assigning this diagnostic category allows for indivi-dualized and flexible diagnostic follow-up tailored to each patient’s needs. This process strengthens early detection, streamlines triage, and facilitates quicker access to appropriate mental health services, which is consistent with the reform’s principles of accessibility and responsiveness.
From an interpretative perspective, the increase in Z03-coded cases may reflect two complementary dyna-mics. On the one hand, it could theoretically raise concerns about a potential “over-categorization” of patients entering the system. On the other hand – and more plausibly – it represents the systematization and formalization of early diagnostic procedures within a structured entry point. In the MHC framework, the Z03 code does not imply overdiagnosis but rather indicates a temporary, administrative diagnosis used to ensure that individuals in need of help are promptly registered, evaluated, and guided toward appropriate care.
Taken together, these findings indicate that RCPs have become a structural foundation for accessibility, coordination, and continuity of care at the local level [4-6].
Coordination of care within the MHC model
Although our dataset does not include direct quantitative indicators of coordination, several organizational mechanisms within the MHC system demonstrate clear progress in this area. Each patient is assigned to a multidisciplinary team (psychiatrist, nurse, psychologist, the-rapist, recovery assistant). The team jointly determines the most appropriate treatment pathway – outpatient follow- up, participation in the day ward, or home-based community support – ensuring continuity across all service levels.
Close cooperation with the affiliated inpatient unit in Prabuty enables seamless transitions between hospital and community settings. Patients hospitalized in this ward remain under the supervision of their assigned MHC team, allowing for immediate post-discharge follow-up and reintegration into outpatient or day-care programs. Shared information systems further enhance communication and strengthen continuity of care.
These mechanisms demonstrate that coordination within the MHC framework is an operational reality embedded in daily clinical practice [6].
Barriers and key areas of success
As detailed in the Methods section, 2024 involved a rapid organizational build-out. The main barrier in year one was the limited community-work experience of newly formed teams, addressed through close senior supervision and targeted training pathways. By year-end, ten staff members had completed or initiated advanced programs (including psychotherapy and community therapy certifications), which strengthened competencies and day-to-day case-management capacity.
Cooperation with local institutions – primary care providers, social welfare services, emergency services, and the police – streamlined referral pathways and improved coordination. Preventive initiatives, such as community education campaigns, “Patient Club” meetings for families, and public exhibitions of therapeutic art, contributed to mental-health awareness and social inclusion.
An innovative development in 2024 was the implementation of a therapeutic ornithology program, combining structured bird-watching sessions with elements of mindfulness and psychoeducation. Recent research indicates that therapeutic ornithology can improve emotional well-being and reduce anxiety among psychiatric patients [12].
Taken together, these developments illustrate a growing adaptive capacity and alignment with the recommendations of the National Mental Health Program and the Working Group of the Mental Health Congress [6, 11]. Overall, the first-year experience suggests that coordinated capacity-building and intersectoral partnerships can translate structural reform into tangible service improvements.
Changes in psychotherapy and psychological consultations
The marked increase in psychotherapy sessions indicates that patients are now more often directed toward structured, long-term psychological support, reflecting an improved coordination of care and faster referral through RCPs. These findings align with the observations of Lisiecka-Biełanowicz et al. [13], who emphasized that well-functioning community systems ensure continuity, adequacy, and personalization of treatment.
In contrast, the decline in short, single-session psychological consultations can be attributed to the systemic reorganization introduced under the MHC model. With the establishment of multidisciplinary teams, initial assessments are now carried out by staff appropriately matched to each patient’s needs. As a result, individuals requiring psychological intervention are more often referred directly to psychotherapy, allowing for quicker and more targeted therapeutic engagement.
Although psychiatrist-provided services increased only moderately (+12%), this pattern reflects a qualitative reorganization rather than a shortfall. In the MHC’s stepped-care model, psychiatrists focus on diagnosis, pharmacotherapy, and periodic medical reviews, while patients typically receive weekly psychotherapy or psychological sessions that provide continuous clinical monitoring. In many stable cases, a single psychiatric visit per quarter is sufficient, because psychologists and community therapists – working within mobile community teams – conduct regular in-home or community-based assessments, flag early risk, and coordinate timely adjustments to care plans. This redistribution of roles reduces the need for frequent physician encounters in the field and consolidates an integrated, team-based approach to psychiatric care.
Transition toward less invasive forms of care
The growing use of the psychiatric day ward in 2024 may indicate a shift toward less invasive forms of care, as is consistent with previous national evaluations reporting reduced hospitalization rates following the implementation of community-based psychiatric services [7, 6]. In our study, the high and rising number of patients treated within the MHC system, combined with the increased use of intermediate services such as the day ward, suggests a broader move toward outpatient and step-down models of support. While our data do not allow for direct comparison with hospitalization trends, the observed pattern aligns with the reform’s intended direction – to improve access while reducing reliance on inpatient treatment.
Diagnostic shifts and early intervention
A particularly noteworthy diagnostic trend was the continued prominence of F41.2 and F43.2 in both years, with significant increases in 2024 (+16.5% and +40.7%, respectively). This likely reflects an improved detection of common emotional and stress-related disorders at earlier stages, enabling timely outpatient interventions.
This underscores the importance of early identification and intervention, which may prevent disease progression and reduce the risk of social exclusion. By supporting individuals before symptoms escalate, the system helps maintain occupational and social functioning. As noted by Kalbarczyk et al. [11], mental health should be regarded not merely as a cost burden, but as a form of individual and collective capital essential for personal development, social participation, and sustainable community growth.
Changing patient profile
Finally, the appearance of F00.1 (dementia in Alzheimer’s disease with late onset) among the most frequently recorded diagnoses, alongside the concurrent decline of F43.1 (PTSD), may indicate a shift in the demographic and clinical profile of patients accessing services. This change could be associated with improved outreach efforts and stronger cooperation with local institutions, allowing MHCs to more effectively identify and support older adults with cognitive disorders.
Limitations and future directions
This study is based on aggregated outpatient data from two consecutive years and does not include hospitalization statistics or qualitative stakeholder perspectives, which constrains causal inference. The observation window – one year pre- and one year post-implementation – limits the assessment of longer-term effects and seasonality. Although headline staffing levels (FTE) were reported, the analysis lacked more detailed workforce data, limiting interpretation of whether higher service volume reflects efficiency or capacity growth. Further multi-regional and longitudinal research is required to assess the sustainability and long-term effectiveness of the MHC model.
Conclusions
Our findings indicate that the implementation in the Mal- bork and Sztum counties of the MHC model was associated with enhanced accessibility, earlier diagnosis, improved coordination, and a more comprehensive approach to psychiatric care. These outcomes are consistent with the guiding principles of Poland’s mental health reform and align with previous national evaluations, underscoring the practical value of community-based mental health services.






