
Silicosis, a well-recognized occupational lung disease resulting from chronic inhalation of respirable crystalline silica, remains a global health concern in mining, tunneling, foundry, and sandblasting industries [1]. The hallmark of silicosis is progressive fibrosis and nodular parenchymal changes, which reliably predispose patients to a variety of complications, including progressive massive fibrosis, pulmonary hypertension, tuberculosis, and lung cancer [2]. In contrast, pleural involvement in silicosis is exceedingly rare, and spontaneous pneumothorax is arguably its most significant recognized pleural complication [3]. Although secondary spontaneous pneumothorax (SSP) has been described in association with silicosis, it is considered an uncommon event and typically occurs late in the disease course when the pulmonary architecture is severely compromised [3, 4]. In a retrospective series of patients with pneumoconiosis, Iga et al. observed that patients with silicosis who developed SSP had significantly worse baseline physical status, required longer durations of chest tube placement, and experienced high rates of recurrence, underscoring the therapeutic challenges in this setting [5]. Similarly, Meena et al. documented that in a cohort of silicosis patients, pneumothoraces were frequently unilateral and carried high morbidity, emphasizing the need for vigilant diagnostic assessment in any acute respiratory deterioration in these patients [6]. The true incidence of SSP among silicosis patients remains unclear, in part because episodes may be misattributed to progression of underlying disease rather than recognized as pneumothorax. A recent cross-sectional study by Bairwa et al. found that among silicosis patients admitted for acute worsening of dyspnea, approximately 43% had a pneumothorax at presentation, with left-sided and bilateral occurrences documented [7]. This suggests that SSP in silicosis may be underappreciated and underscores the importance of maintaining a high index of suspicion. In this context, we present an instructive case of advanced silicosis complicated by a persistent left-sided spontaneous pneumothorax, managed successfully with uniportal video-assisted thoracoscopic surgery (VATS).
Our aim is to highlight the pathophysiological mechanisms, diagnostic challenges, and surgical considerations in managing this rare but potentially life-threatening complication.
A 59-year-old male patient with a history of advanced pulmonary silicosis was admitted to our department with a persistent left-sided secondary spontaneous pneumothorax (Figure 1 A). His past medical history included a right-sided mantle pneumothorax, a bronchopulmonary fistula on the right, and multiple prior thoracoscopic operations on the right lung. The patient had initially presented several weeks earlier to a community hospital with a left-sided pneumothorax, but declined referral to our department at that time despite medical advice. In the days preceding the current admission, he developed progressive dyspnea, chest pain, headache, and a dry cough, which led him to seek medical attention again. Due to persistence of the pneumothorax, he was transferred to our institution for further diagnostic evaluation and treatment. Chest radiography and computed tomography of the thorax confirmed an extensive left-sided seropneumothorax with signs of mediastinal shift suggesting a tension component. Imaging also demonstrated bilateral perihilar consolidations, disseminated nodules, pleural thickening, and fibrotic parenchymal alterations, consistent with the known diagnosis of silicosis. No evidence of emphysematous bullae was identified (Figure 2). After preoperative preparation, the patient underwent uniportal video-assisted thoracoscopic surgery with pleurolysis and subtotal pleurectomy of the left hemithorax (Figure 3). The intervention was completed without complications, and the patient was transferred postoperatively to the intensive care unit. He was extubated promptly and remained hemodynamically stable without respiratory compromise. Histology confirmed the diagnosis of lung silicosis (Figure 4). On the first postoperative day, he was transferred to the general ward, where he continued his recovery with mobilization and respiratory physiotherapy. The postoperative course was uneventful, the chest tube was removed on the sixth postoperative day, and the patient was discharged on the following day in a stable clinical condition. At the time of discharge, he was free of respiratory symptoms, and the surgical wounds were unremarkable. At follow-up after 10 days, the patient remained free of symptoms, and the chest X-ray showed no signs of recurrent pneumothorax. Secondary spontaneous pneumothorax (SSP) is a recognized but infrequent complication of advanced silicosis and can present dramatically, including bilateral or tension physiology, because stiff, fibrotic lungs poorly tolerate additional loss of functional volume. Case series and reports emphasize that pneumothorax in silicosis often occurs in the setting of progressive massive fibrosis (PMF), pleural adhesions, and subpleural nodules; nonetheless, its overall incidence remains low, which likely contributes to delays in definitive management and variation in practice patterns [1, 5, 8]. Our patient’s imaging did not demonstrate frank emphysematous bullae, underscoring that SSP in silicosis can arise without obvious cystic disease. Mechanistically, rupture of subpleural silicotic nodules, ischemic necrosis around conglomerate masses, and shear forces at fibrotic–pleural interfaces have all been implicated, in addition to pleural thickening that can impede re-expansion and predispose to persistent air leak. Observational data suggest an association between bullae and SSP in acute/accelerated silicosis, but the absence of bullae on CT does not preclude rupture, particularly in the context of PMF and heterogeneous pleuro-parenchymal scarring [1, 2]. Initial conservative measures (oxygen, drainage) frequently fail in SSP because of reduced elastic recoil and impaired pleural apposition in diseased lungs. Contemporary reviews and surgical series support early escalation to thoracoscopic management for ongoing air leak, non-expansion, or recurrence, with VATS allowing targeted treatment of culprit lesions and durable pleurodesis in a single setting. In comparative cohorts, VATS – often combined with mechanical and/or chemical pleurodesis – shortens hospital stay and reduces recurrence relative to tube drainage and chemical pleurodesis alone, even in older or comorbid SSP populations. The optimal pleurodesis strategy in SSP remains debated. Long-term series indicate that, when combined with bullectomy or targeted resection, pleural abrasion, poudrage, and pleurectomy achieve similarly high freedom from re-operation, while choice is often individualized to pleural anatomy and surgeon preference. In fibrotic pneumoconiosis with dense adhesions, subtotal pleurectomy can be pragmatically favored to maximize pleural symphysis and minimize residual pleural space, aligning with approaches reported in silicosis-specific case series [8]. Finally, recurrence risk after SSP remains higher than for primary pneumothorax and is amplified by underlying interstitial and fibrotic disease burden. Accordingly, definitive pleural procedures at first index hospitalization for persistent air leak or failed re-expansion are increasingly recommended to improve long-term outcomes and quality of life; our patient’s prompt recovery after uniportal VATS with pleurolysis and subtotal pleurectomy is concordant with these data [5].
Figure 1
Serial chest radiographs. A – On admission, showing a large left-sided pneumothorax (arrows). B – Immediately after thoracoscopic pleurectomy, demonstrating lung re-expansion and satisfactory postoperative result. C – At discharge, showing complete resolution with no residual pneumothorax
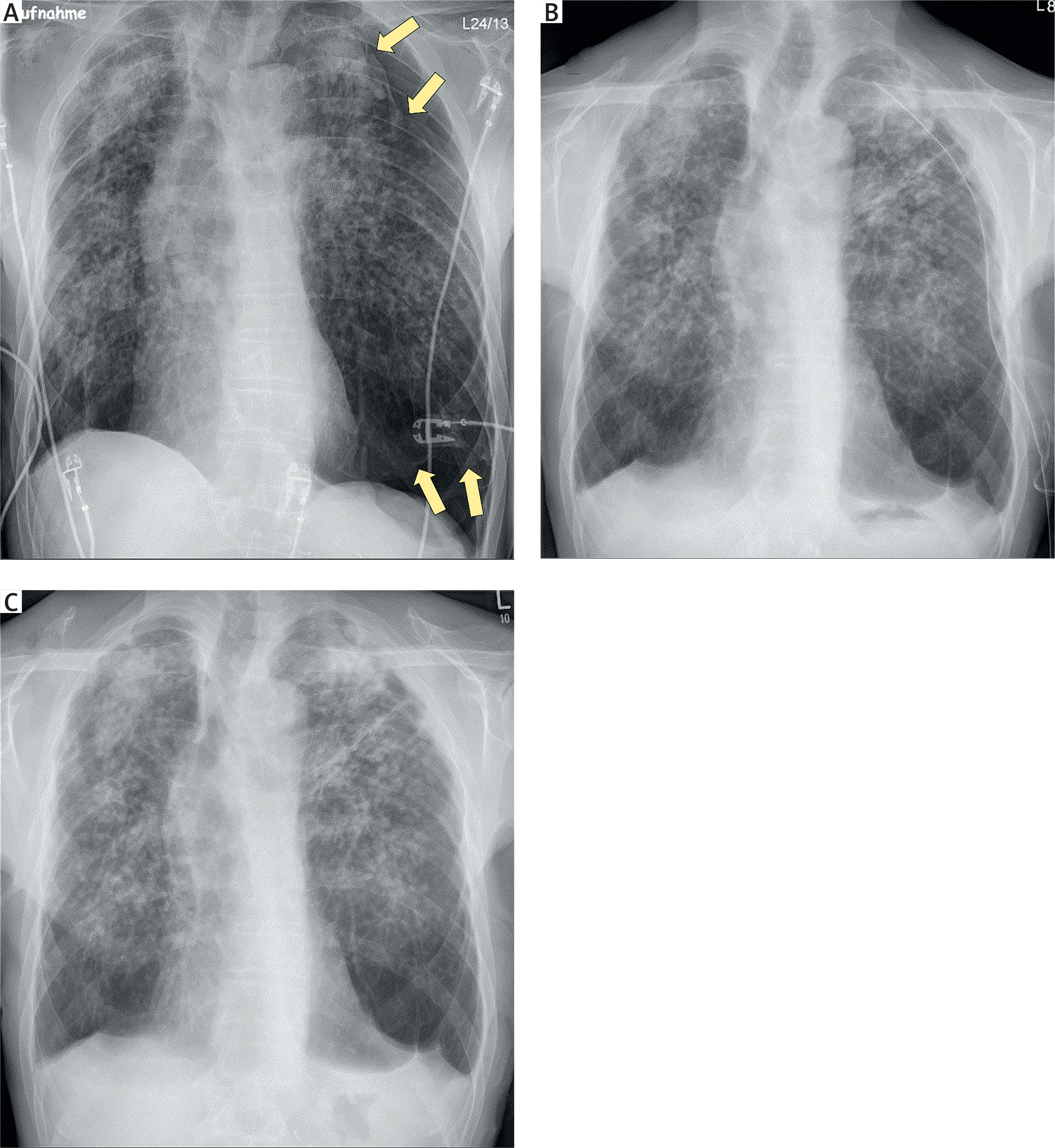
Figure 2
Computed tomography of the chest. A – Axial image showing a left-sided pneumothorax with pleural adhesions between the lung and chest wall (arrow). B – Axial image demonstrating mediastinal shift to the right, suggestive of a tension component (arrow). C – Axial image revealing diffuse and advanced silicotic changes with multiple parenchymal nodules (arrows). D – Coronal reconstruction illustrating the extent of pneumothorax. E – Sagittal reconstruction confirming parenchymal distortion and pleural involvement
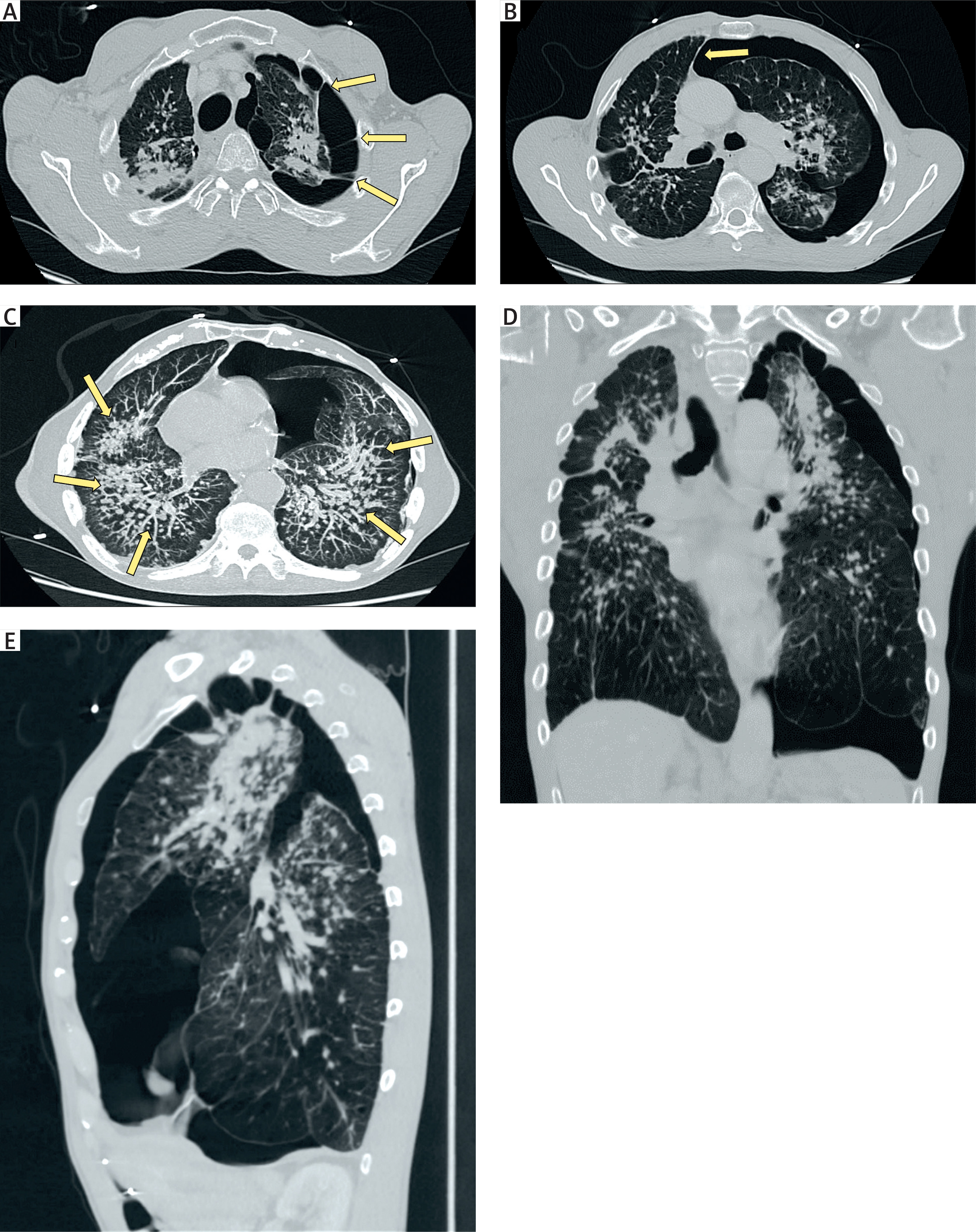
Figure 3
Intraoperative thoracoscopic views showing dense pleuro-pulmonary adhesions (blue arrows) and advanced fibrotic changes of the lung parenchyma: A – dorsoapical region; B – dorsobasal region
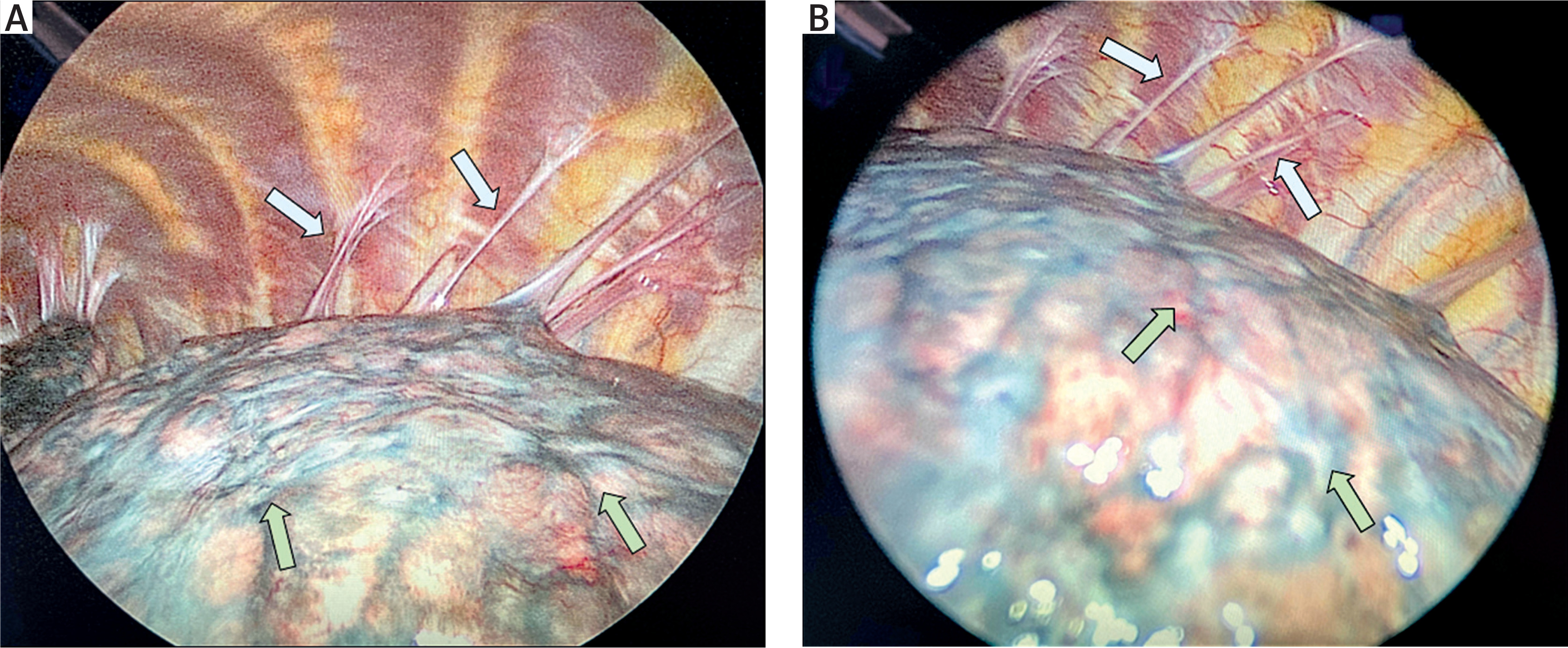
Figure 4
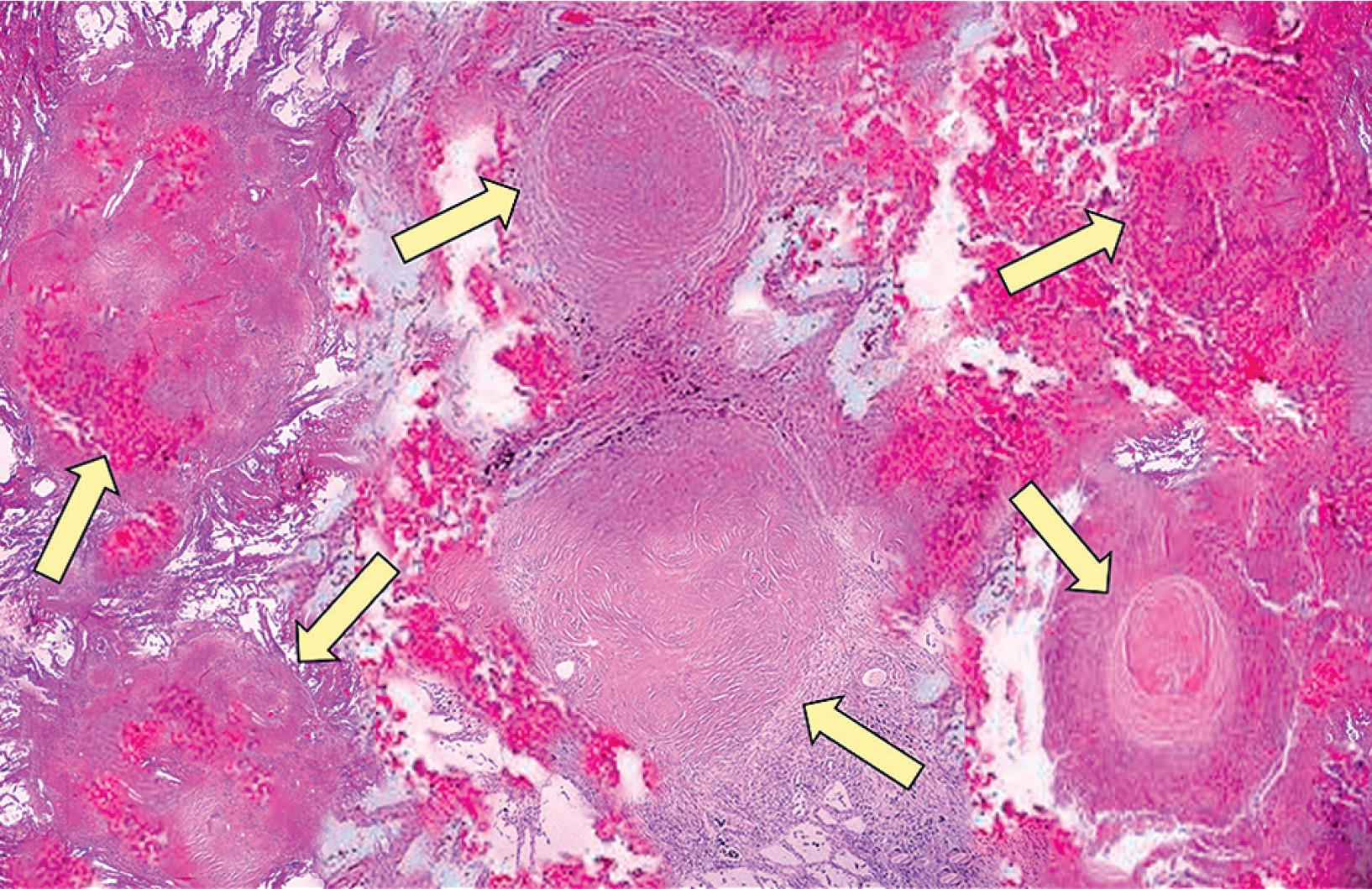
Histopathological appearance of lung silicosis. Silicotic nodules within the lung parenchyma (arrows), composed of interlacing bundles of dense, eosinophilic collagen with minimal associated inflammatory reaction. The number and size of silicotic nodules increase with cumulative silica exposure and duration, and correlate with the degree of restrictive lung disease
Spontaneous pneumothorax is a rare but clinically significant complication of advanced silicosis that should be considered whenever affected patients present with acute chest pain or dyspnea. Its occurrence often reflects severe underlying structural lung damage and may be associated with protracted air leaks, difficulty in achieving re-expansion, and a high risk of recurrence. Early recognition, prompt imaging, and timely escalation to definitive pleural intervention are essential for favorable outcomes. Our case highlights that uniportal video-assisted thoracoscopic surgery with pleurolysis and subtotal pleurectomy can be performed safely in selected patients with compromised fibrotic lungs, providing effective resolution of persistent pneumothorax. Awareness of this complication and multidisciplinary management are crucial to optimize care in this vulnerable patient population.









