
Infective endocarditis (IE) is a life-threatening disease caused by microbial infection of the endocardial surface of the heart and most often involving the cardiac valves. Despite diagnostic and therapeutic advances, IE carries an in-hospital mortality of 15–30%, with higher rates when complicated with periannular extension such as abscess formation, fistula, or large vegetations, emphasizing the need for early diagnosis and optimal management [1].
Herein, we report a rare case of native aortic valve IE complicated by paravalvular abscess, aorto-right atrial fistula, and large right atrial vegetation, successfully managed with emergency surgical intervention.
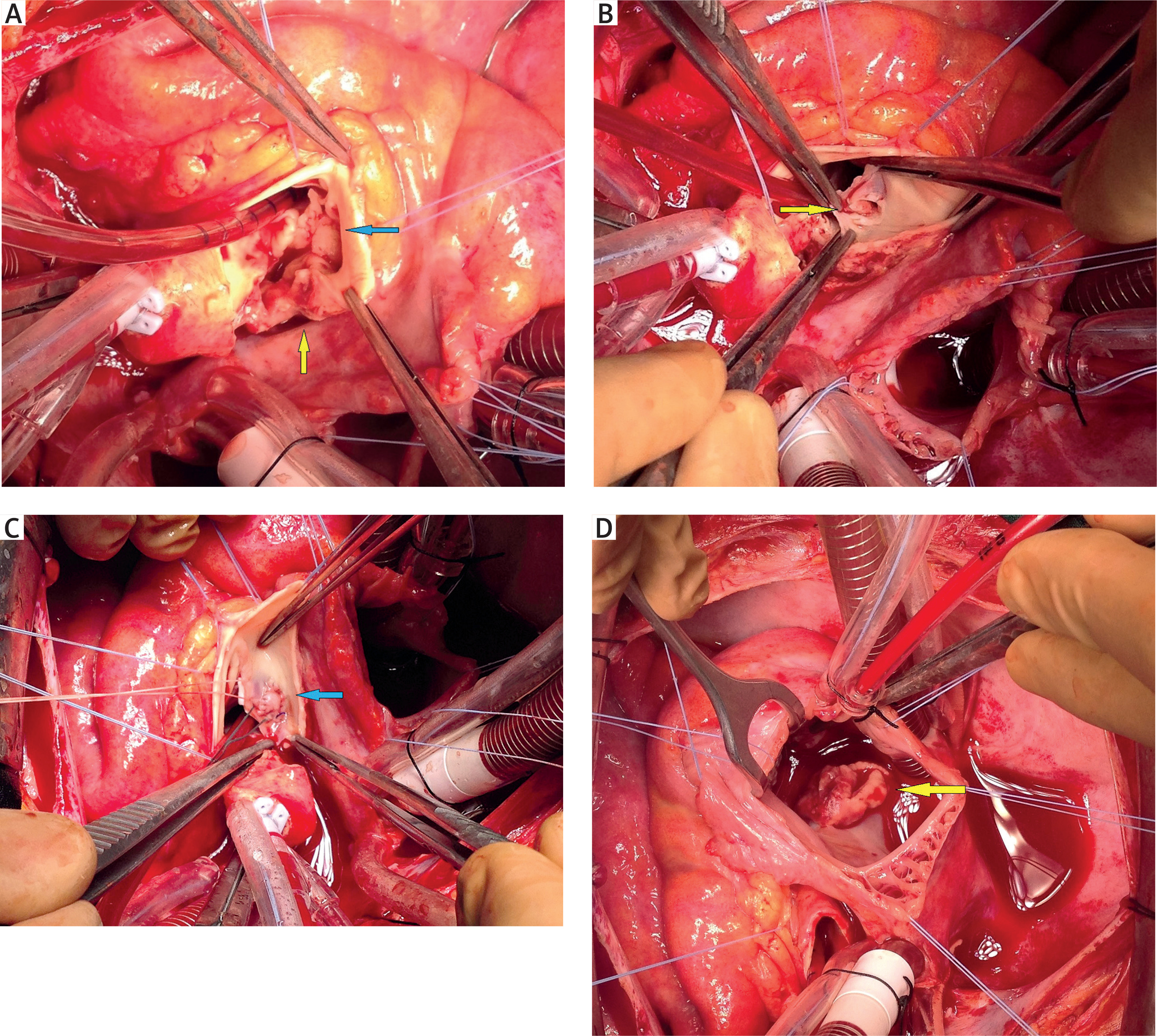
A 21-year-old female patient was admitted to our hospital with complaints of fever and abdominal pain. She had persistent fever for approximately 45 days before admission. Physical examination revealed splenomegaly, while abdominal ultrasonography and computed tomography (CT) demonstrated splenic infarcts. Laboratory findings showed leukocytosis (12,400/mm³) and elevated C-reactive protein (23.2 mg/l). The patient was hospitalized in the surgical intensive care unit for further evaluation. During follow-up, she developed dyspnea and hypotension. Transthoracic echocardiography (TTE) revealed severe aortic regurgitation and a 0.5 × 0.6 cm vegetation on the aortic valve. Additional findings included an aortic paravalvular abscess, an aorto-right atrial fistula originating from the noncoronary sinus and a 1.2 × 1.3 cm mobile mass in the right atrium. Brain CT demonstrated ischemic infarct areas without neurological deficits. Considering the identified findings, a multidisciplinary team including cardiology, infectious diseases, and cardiovascular surgery decided on emergency surgical intervention with the diagnosis of complicated aortic valve IE. The time from admission to hospital and diagnosis/surgery was 5 days. The surgery was performed via median sternotomy with aorto-bicaval cannulation. Left-sided vegetations were observed on the non-coronary sinus, left coronary sinus, and the aortic wall, with destruction of these cusps (Figure 1 A). The fistula between the noncoronary cusp and the right atrium was confirmed (Figure 1 B). The aortic valve and vegetations were excised, and a 21-mm ATS mechanical valve was implanted via aortic root enlargement using the Nicks technique with pledgeted sutures. The fistula orifice was closed with an autologous pericardial patch (Figure 1 C). Right atriotomy for removal of the mobile right atrial mass incidentally revealed an atrial septal defect. The right atrial mass was removed, appearing macroscopically as vegetation (Figure 1 D). The atrial septal defect was repaired with continuous primary suturing. The patient received empirical antibiotic therapy in the surgical intensive care unit for 2 days. After the two sets of blood cultures were found positive for methicillin-sensitive Staphylococcus aureus, the antibiotic regimen was adjusted accordingly. No specific predisposing factors for infective endocarditis were identified, including recent dental procedures, invasive interventions, or intravenous drug use. The postoperative course was uneventful, and the patient was discharged after completing 6 weeks of intravenous antibiotic therapy. The patient was regularly monitored for INR levels up to the second-year follow-up without cardiac complaints.
Figure 1
A – Intraoperative view demonstrating vegetations on the left and non-coronary sinuses (blue arrow), along with destruction of the aortic wall (yellow arrow) extending to the adjacent cusps. B – Intraoperative view demonstrating the orifice of the aorto-right atrial fistula originating from the non-coronary cusp. C – Intraoperative view of the aorto–right atrial fistula orifice repaired with an autologous pericardial patch. D – Intraoperative view of the right atrial mass which appeared macroscopically as a vegetation
This case represents the multifaceted course of IE in a young patient and draws attention to several clinically significant aspects of the disease. Periannular complications, including abscess and fistula formation, represent advanced stages of the disease. Extension of infection into the perivalvular tissue occurs in up to 30% of aortic valve endocarditis cases, whereas aorto-cavitary fistulas are reported in fewer than 2% [1–3]. Such complications are associated with rapid hemodynamic deterioration, highlighting the critical importance of early detection. In our patient, echocardiography played a pivotal role not only in identifying vegetations but also in revealing the abscess, fistula, and mobile right atrial mass which guided the decision for emergency surgery.
Systemic embolic events constitute another major concern in IE, particularly in the presence of large and mobile vegetations. Splenic infarctions and cerebral ischemic lesions, both observed in our patient, may occur in approximately 20–40% of IE cases [4]; notably, as in our patient, such embolic complications are commonly asymptomatic and diagnosed by non-invasive imaging [1]. Some embolic events, even when clinically silent, carry a worse prognosis and frequently require urgent surgical intervention. Current guidelines strongly recommend early surgical intervention in patients with recurrent embolization, periannular extension, and persistent infection despite appropriate antibiotic therapy [1, 5].
In complicated IE, the multiplicity of pathological components makes surgical intervention highly challenging and is linked to increased morbidity and mortality. Early recognition of periannular extension and prompt intervention remain crucial to improving survival in this complex disease. The choice of surgical strategy in complicated IE must be individualized and adapted to the extent of infection. Radical debridement of infected tissue is essential to reduce the risk of recurrence, while repair of intracardiac fistulas with autologous or bovine pericardial patches has demonstrated durable outcomes [6]. In our case, pericardial patch closure of the aorto-right atrial fistula, mechanical valve replacement, and primary repair of an atrial septal defect were successfully performed, and the incidental discovery of a foramen ovale type defect underscored the importance of thorough intraoperative evaluation, as concomitant cardiac lesions may influence both surgical planning and long-term prognosis. Another key point is the timing of surgery. Several studies have demonstrated that early surgical intervention in complicated IE is associated with improved survival compared to delayed procedures [1]. Despite the risks and a delayed diagnosis of 5 days, emergency surgery was lifesaving for this patient with complicated infective endocarditis. Microbiological findings play an equally important role in postoperative management. Staphylococcus aureus is among the most virulent organisms causing IE, with high rates of periannular destructions and embolization [1, 7]. Targeted antibiotic therapy is crucial, and close collaboration with infectious disease specialists ensures optimal outcomes.
This case emphasizes the importance of a multidisciplinary approach involving cardiologists, infectious disease specialists, and cardiac surgeons, as well as other specialties such as neurology and general surgery depending on the individual complications of IE. Such collaboration facilitates timely decisions on surgical timing, antibiotic therapy, and postoperative management, ultimately improving survival in this high-risk patient group.









