
Purpose
Carcinoma of the hard palate is a relatively uncommon entity, accounting for 1-3.5% of all head and neck cancers [1]. Surgical resection remains the mainstay of treatment; however, it is frequently associated with a development of oro-antral or oro-nasal fistulae, necessitating lifelong rehabilitation with obturator prostheses. These post-operative defects contribute to substantial functional morbidity, including dysphagia, compromised mastication, speech impairment, and nasal regurgitation, collectively diminishing patients’ quality of life [2].
Surface mould brachytherapy (SMB) has emerged as a viable, organ-preserving alternative for managing early-stage superficial lesions of the oral cavity, particularly hard palate cancers. By delivering high-dose-rate (HDR) brachytherapy with custom-fabricated mould, SMB allows conformal dose distribution while sparing adjacent normal structures [3]. In a study of 35 patients, Budrukkar et al. demonstrated favorable outcomes with this approach, reporting a 5-year local control rate of 76% in head and neck malignancies treated with SMB. Furthermore, SMB provides excellent functional outcomes and lower toxicity profile [4]. This technique, though conventionally performed regularly for hard palate cancers, is truly challenging in edentulous hard palate cancer cases. However, with advanced dental fabrication methods and individualized approach, SMB can be performed for such cases [5].
In this report, we presented a case of completely edentulous patient with a second primary squamous cell carcinoma of the hard palate (cT1N0M0), previously treated with external beam radiotherapy. A novel HDR brachytherapy approach using customized complete denture prosthesis with interlocking acrylic struts was employed for this patient. This case highlights the feasibility and utility of individualized SMB in the treatment of recurrent or second primary tumors in complex, edentulous settings, contributing to the evolving paradigm of patient-specific brachytherapy applications.
Material and methods
Case presentation
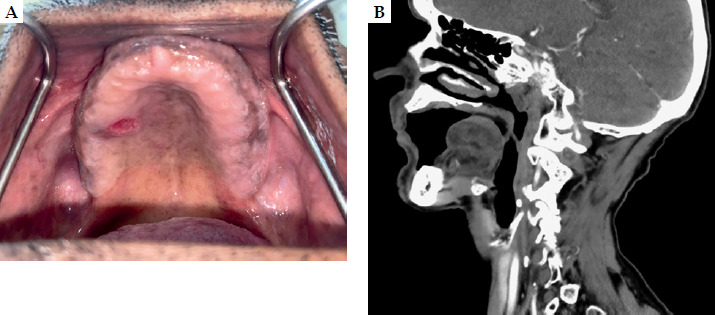
A 73-year-old male, with no known comorbidities and a history of chronic beedi smoking (10-12 beedis/day for 20 years, discontinued 8 years ago), presented with a persistent, non-healing ulcer over the anterior aspect of the hard palate. He was previously treated for stage III squamous cell carcinoma of the left vallecula (cT3N0M0) with definitive concurrent chemo-radiotherapy (70 Gy in 35 fractions) eight years earlier. On examination, a 1 cm × 1 cm superficial ulcer was noted on the right anterior hard palate, adjacent to the alveolar ridge. The patient was fully edentulous and had no palpable cervical lymphadenopathy (Figure 1A). Contrast-enhanced computed tomography (CECT) of the head and neck revealed a superficial lesion confined to the mucosal surface of the hard palate, with no underlying bony erosion or nodal involvement (Figure 1B). Histopathological evaluation confirmed moderately differentiated squamous cell carcinoma. Based on these findings, the disease was staged as carcinoma of the hard palate, cT1N0M0, stage I (AJCC 8th edition).
The patient was treated with conventional B/L portals using cobalt-60 and off-cord after 46 Gy. Planning was done using conventional simulator, assuming that patient has received maximum tolerable dose. Considering previous irradiation and elderly age, multidisciplinary clinic decision was to plan for surface mould brachytherapy and not to consider for surgery. The patient’s complete edentulism deemed him unsuitable for conventional surface mould brachytherapy due to significant challenge in achieving adequate prosthetic retention, particularly under the weight of nylon catheters and wax components required for SMB. However, a notable finding on clinical examination was the prominent vertical height of both the maxillary and mandibular arches. This anatomical consideration facilitated the fabrication of a unique, patient-specific interlocking maxillomandibular mould that ensured prosthetic stability and reproducibility of catheter positioning for brachytherapy delivery.
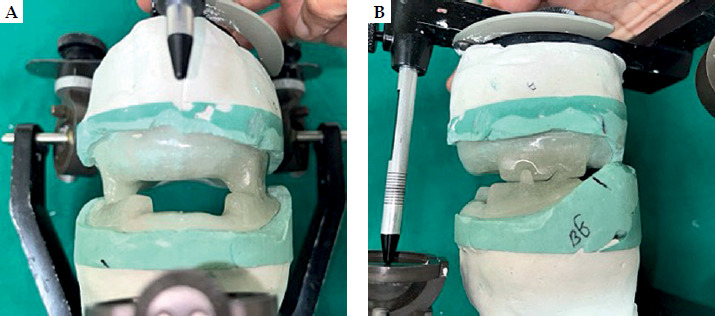
The prosthetic fabrication was carried out in collaboration with the Department of Maxillofacial Prosthodontics. Primary impressions of the maxillary and mandibular arches were obtained using irreversible hydrocolloid (Zelgan Plus™; Dentsply). Once the custom tray was fabricated, borders of the prosthesis were muscle trimmed with low-fusing impression compound (DPI™ Pinnacle tracing stick), to ensure optimal retention, stability, and support. A wash impression was made with light body elastomeric material (3M Express XT Light Body) (Figure 2); a stone master cast was obtained and tentative wax occlusal rims were fabricated on acrylic record bases (Figure 3). Maxillo-mandibular relation was recorded ensuring proper centric relation (with the condyles properly seated in the fossa) and vertical relation (at the physiologic rest position) of both the jaws (Figure 4). Once the master casts were mounted, the wax rims were modified and interlocking struts were carved out. The anterior portion of maxillary denture was kept devoid of the rims in order to facilitate anterior-posterior placement of nylon catheters. The trial setup was assessed and deemed adequate. The maxillary and mandibular denture was acrylized in heat-cure polymerizing poly methacrylate resin (Trevalon; Dentsply Sirona), and the dentures were checked clinically for the right fit and retention (Figure 5; Supplementary Video 1).
Fig. 2
Primary impression of the maxillary and mandibular arches recorded with irreversible hydrocolloid
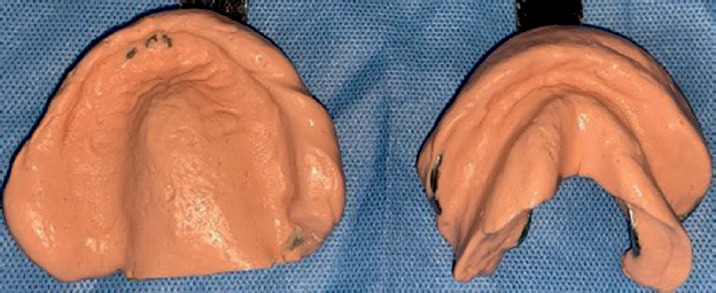

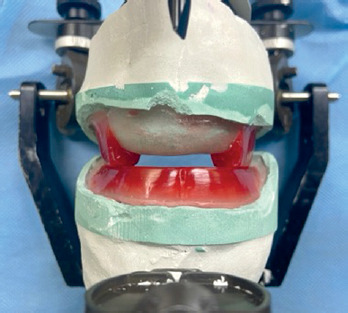
Fig. 5
Mounted casts on an articulator. Note the acrylized maxillary and mandibular rims with interlocking struts, allowing proper stability of the surface mould
Target volume was delineated on the maxillary acrylic mould by drawing gross tumor volume, and 1 cm margin was added to create clinical target volume (CTV). Subsequently, the positions of catheters were decided and marked on the mould with inter-catheter distance of 1 cm (Figure 6A). Modelling wax softened and adapted on the polished outer surface of the acrylic maxillary mould. Four 6-F nylon catheters were positioned 1 cm apart as already decided and marked on the mould, and secured with a layer of wax and fitted to the patient, ensuring proper placement (Figure 6B, C). A CT scan was carried out to verify the intimate fit of the prosthesis (Figure 7A) and to confirm absence of air gaps between the mould and palatal mucosa, ensuring accurate dose distribution. Simulation scan was done with and without copper wire for better delineation of clinical target volume (Figure 7B). Treatment planning was conducted using Oncentra brachytherapy planning system (Elekta™), with dose prescribed at catheter point and reference isodose line optimized to cover the lesion with appropriate margins (Figure 8). HDR brachytherapy using a remote afterloading iridium-192 (192Ir) source was delivered at a dose of 4 Gy per fraction, twice daily, with a minimum inter-fraction interval of 6 hours, to a total dose of 52 Gy over 7 consecutive days. CTV was completely enclosed within 90% isodose line. D2cc to the oral cavity, maxilla, and mandible were 10 Gy, 1 Gy, and 1 Gy, respectively.
Fig. 6
A) Target volume delineation on the maxillary acrylic mould. B, C) Catheter fixation with modelling wax. D) Checking the fitting of surface mould on the patient
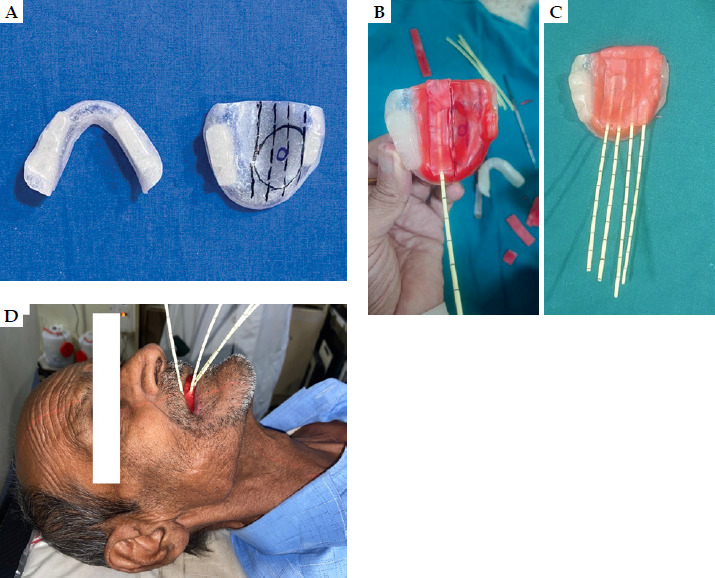
Fig. 7
A) Check scan taken for any air gaps. B) Simulation computed tomography scan after wiring gross tumor volume with copper wire
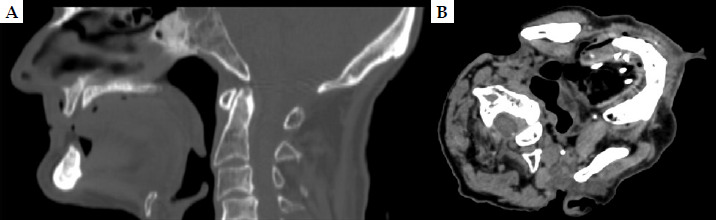
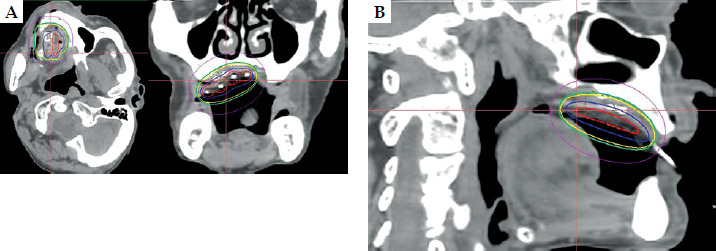
Fig. 8
A, B) Dose distribution on the planning scan of final plan. Red line: 200% isodose, blue line: 150% isodose (both on the mould), yellow line: 100% isodose, green line: 90% isodose, magenta line: 50% isodose, GTV: green dotted line, and CTV: orange dotted line
The patient developed grade 3 mucositis assessed at 2 weeks post-brachytherapy (Figure 9), which corresponded to the 100% isodose line and resolved subsequently with appropriate oral care. At the last follow-up, twenty two months post-therapy, the patient was disease-free with excellent cosmetic and functional outcomes (Figure 10), including intact speech and swallowing, with no signs of recurrence observed.


Discussion
The presented case underscores the clinical value of surface mould brachytherapy (SMB) in addressing a particularly challenging scenario: a second primary squamous cell carcinoma (SCC) of the hard palate in a completely edentulous, previously irradiated patient. Conventional SMB workflows are optimized for dentate individuals, where natural dentition or dentures provide inherent stability and reproducibility for mould positioning [6].
Dholam et al. addressed a challenging clinical case of severe trismus in a patient with recurrent oral carcinoma, for whom conventional surgery and external beam radiotherapy were contraindicated. The authors anchored a custom acrylic mould using two endosteal implants placed in the edentulous maxilla, allowing mould retention and secure delivery of HDR brachytherapy (49 Gy in 14 fractions of 3.5 Gy). The patient experienced no recurrence at 6 months post-treatment, and the technique proved both innovative and technically feasible. However, it involved surgical placement of implants and highly individualized prosthetic fabrication, which may not be universally implementable [5]. Similarly, Ealla et al. described a simplified and cost-effective method using dental wax molded over dental stone casts for stage I hard palate carcinoma. This technique enabled precise catheter alignment without the need for dentition or implants. Importantly, it achieved 100% local control at 2 years, highlighting the oncologic efficacy of SMB in early-stage disease [7]. Apart from being used as radical treatment in early stage, SMB has been also employed as boost in external beam radiotherapy in T2-T3 N0 hard palate cancers in a case series of five patients [8]. However, the fabrication process was entirely manual, and depended on dental impressions and skilled prosthodontic input. The lack of digital integration limited adaptability, especially in cases with complex anatomy or in settings with no dental infrastructure.
A more technologically advanced approach was presented by Lancellotta et al., who employed individualized 3D-printed moulds created from patient imaging. This method ensured high precision in catheter positioning, excellent mucosal conformity, and enhanced reproducibility. The mould was fabricated using bio-compatible resin, eliminating the need for conventional impressions, thus expediting workflow. The patient achieved successful local control, but broader implementation is currently limited by the availability and cost of 3D-printing technology, especially in low-resource environments [9].
Collectively, the above studies illustrate that mould-based HDR brachytherapy provides excellent local control and function preservation in early-stage hard palate carcinoma. However, the choice of fabrication method ranging from manual thermoplastic or acrylic moulds to advanced 3D-printed carriers, must balance clinical efficacy, technical complexity, cost, and resource availability. Future integration of digital workflow and 3D-printing may overcome the existing limitations, offering personalized, accessible solutions for intra-oral brachytherapy across diverse healthcare settings. Despite these advances, practical challenges, such as fabrication time, cost, and anatomical constraints, remain relevant. The interlocking strut-based design employed in the current case presents a reproducible, cost-effective alternative, providing mechanical retention, accurate catheter alignment, and close mucosal contact, the key parameters for effective dose distribution and clinical efficacy.
Re-irradiation in previously treated head and neck cancers involves well-documented risks of both acute and late toxicities. A prospective experience reported by De Crevoisier et al. in 169 patients treated with full-dose re-irradiation, revealed high rates of acute grade 3 (32%) and grade 4 mucositis (14%), along with significant long-term complications, including cervical fibrosis (41%), mucosal necrosis (21%), osteoradionecrosis (8%), trismus (30%), and five instances of carotid blowout hemorrhage. These data emphasize the critical importance of precise target delineation, rigorous dose constraint adherence, and judicious patient selection in re-irradiation setting [10]. In this context, SMB offers distinct advantages, particularly in delivering highly localized re-irradiation with sharp dose fall-off, thereby minimizing exposure to adjacent critical structures. In a case series of 18 patients with oral and oropharyngeal cancer, treated either with SMB alone or as boost, 1-year and 2-year local control was 81% and 68%, respectively, with favorable acute and late toxicity profile [11].
In the present case, the patient achieved favorable oncologic and functional outcomes, including complete mucosal healing, preserved oral intake, and sustained local control at 24 months post-treatment, all without hospitalization or feeding tube dependency. These factors directly impact post-treatment quality of life and patient satisfaction.
Although SMB could be successfully implemented in our edentulous patient, it requires overcoming various challenges with multidisciplinary team approach. First of all, the major challenge is identifying the suitable patient, e.g., our case: the patient had adequate maxilla-mandibular arch height and good mouth opening to fabricate the implant process and manipulate the mould making and retention. Additionally, it is essential to assess the patient for any residual grade 3 toxicity, such as xerostomia or mucosal changes from previous radiotherapy, especially in re-irradiation cases. Convincing the patient for the complex procedure before starting treatment is another important factor, which could be overcome by detailed counselling and explanation of the entire procedure as well as pros and cons of different treatment options. The most important requirements for execution of such complex technique are a motivated prosthodontic department and appropriate communication and collaboration with the entire team. Treatment delivery following planning also requires expertise and personalized attention to ensure adequate fitting and retention of the mould, so that planned dose can be delivered with precision.
This case demonstrates the role of SMB as a viable, outpatient-compatible option for re-irradiation in anatomically complex, edentulous patients. With careful planning and innovative prosthetic solutions, curative-intent treatment can be pursued without compromising patient safety or comfort.
Conclusions
Surface mould brachytherapy is a feasible option even in edentulous hard palate cancers. Patient selection and adapting and fabricating the technique are the key for success of SMB. The incorporation of interlocking acrylic struts is an innovative, cost-effective, and viable approach, to ensure prosthesis stability, precise dose delivery, and favorable oncological and functional outcomes.
The case report was presented at the 14th Annual Conference of Indian Brachytherapy Society IBSCON-2024, Gurugram, India.
Supplementary Video 1 is available: https://drive.google.com/file/d/1LxF1CBRju8qqdpyvgMT0YJvY6-n8fFhh/view?usp=drive_web








