
Pulmonary segmentectomy is a sublobar resection technique currently recommended in guidelines as a radical treatment option for primary non-small cell lung cancer (NSCLC) lesions smaller than 2 cm [1, 2], and it is also considered a treatment option for metastases in selected patients. Apicoposterior segmentectomy allows for histological diagnosis and preserves more lung parenchyma than upper lobectomy or trisegmentectomy. Segmentectomy performed via the uniportal video-assisted thoracoscopic surgery (VATS) technique is both feasible and safe [3, 4].
However, it is considered a technically demanding procedure, especially due to the preservation of segment 3. The anatomical relationships are difficult to understand, particularly for junior or less experienced surgeons, and identification and separation of the intersegmental plane is also challenging. Furthermore, the vascular anatomy of the upper left lobe is characterized by significant variability. We present our technique for a left-sided S1+2 segmentectomy performed via the uniportal VATS approach.
The case involves a 57-year-old male patient, with a history of total gastrectomy and esophagojejunal Roux-en-Y anastomosis, along with D2 lymphadenectomy performed in January 2023 for tubular adenocarcinoma of the stomach (Lauren intestinal type), G2, ypT2 ypN0 TRG2 (AJCC 8th edition), R0 (0/9 lymph nodes), following preoperative FLOT chemotherapy and one postoperative FLOT cycle (discontinued due to intolerance). No significant comorbidities were observed.
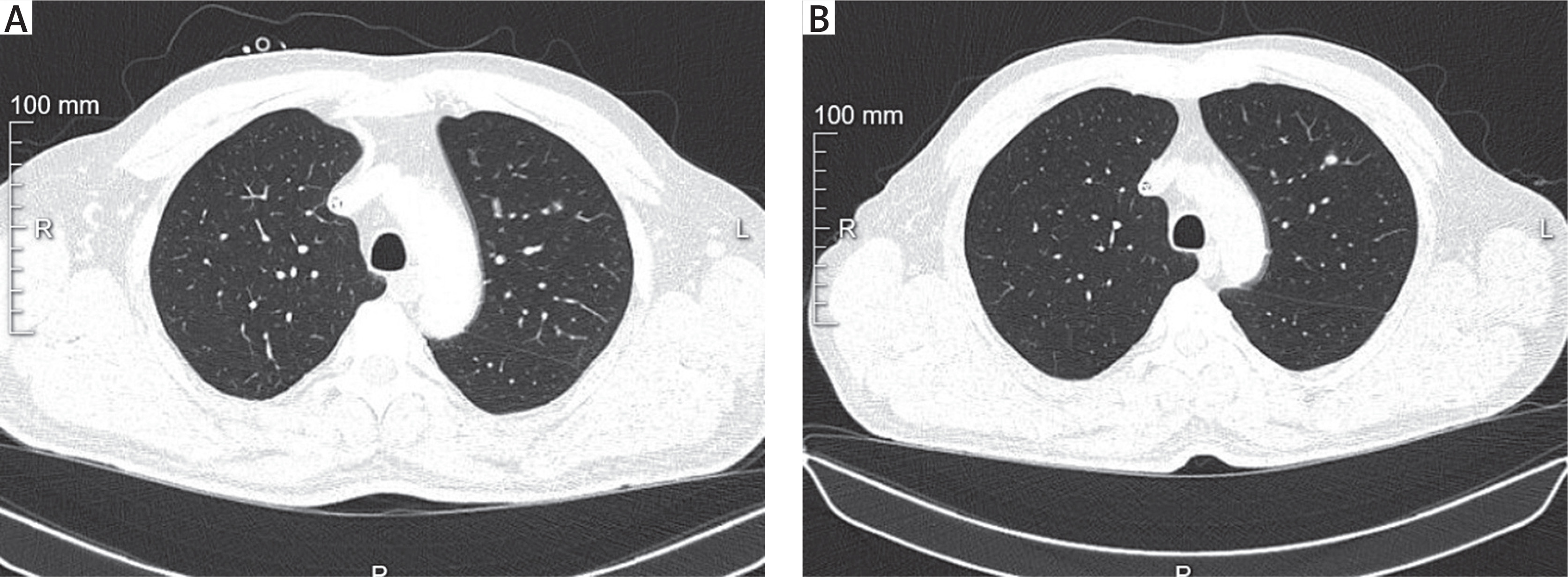
Surgical indication: Suspected pulmonary adenocarcinoma. Positron-emission tomography computed tomography (PET-CT) revealed a 5 mm nodule in the upper lobe of the left lung with SUV 1.3 (possibly underestimated due to respiratory motion). Preoperative CT showed a solid 5 mm nodule in segment 1 of the left lung with interval growth compared to 2023 CT (when the patient underwent gastrectomy for gastric cancer).
Lesion location: Segment S1+2 of the left lung; 5 mm diameter; deep parenchymal location; no enlarged lymph nodes on CT (Figure 1).
Procedure: Approach: Uniportal VATS, 3 cm incision in the anterior axillary line in the 4th intercostal space.
Dissection of segmental vessels and bronchus: Following anatomical landmarks, the A1+2a+b artery was divided with an endostapler, and the V1 vein was divided with a harmonic scalpel. The A1+2c artery was clipped with Hem-o-lok clips and divided with a harmonic scalpel. In intraoperative examination of the lymph node from the B1+2 bronchial region, no malignant cells were detected. The B1+2 bronchus was divided with an endostapler after bronchoscopic confirmation. Finally, the V1+2 vein was divided with an endostapler.
Intersegmental plane: Identified using the inflation–deflation method. Lymphadenectomy: Radical lymphadenectomy of stations 5, 6, 7, 9, 10L, 12L, and 13L. Operative time: 2 hours and 10 minutes (skin incision to dressing). Assistance: Third-year thoracic surgery resident. Intraoperative complications: None.
Outcomes. Uncomplicated postoperative course. The chest drain was removed on postoperative day 1. The patient was discharged on day 2.
Final histopathology: Lung adenocarcinoma, NOS, G1, pT1aN0M0 PL0 (AJCC 8th edition), R0. Tumor size: 0.5 cm. Pleural surface: smooth. Pleural involvement: absent. Tumor distance from pleura: 0.7 cm. Bronchial resection margin: negative; closest distance from tumor: 1.5 cm. Parenchymal resection margin: negative; closest distance from tumor: 1.5 cm. Vascular resection margin: negative; closest distance from tumor: 1.5 cm.
Anatomical segmentectomies are a valuable option for resecting indeterminate pulmonary lesions when minimally invasive diagnosis is infeasible or challenging (as in this 5 mm lesion), particularly if the lesion is deep within the parenchyma, allowing for lung tissue preservation. This should be considered especially in patients with prior oncologic surgery or borderline pulmonary function.
S1+2 segmentectomy is regarded as one of the most technically demanding types of segmentectomies. The added challenge in this case was the presence of a junior resident as an assistant – a factor that often prolongs procedures. The operation was completed smoothly, without conversion, with a full lymphadenectomy, and within a time comparable to the median operative times reported in the literature [5]. This demonstrates the potential for maintaining high oncologic standards while training young surgeons in minimally invasive techniques.
In summary, we believe that apicoposterior segmentectomy of the left lung via the uniportal VATS technique is safe when performed with caution and thorough anatomical knowledge.









