







In recent years, radial access (RA) has been recommended in guidelines as the preferred access for any percutaneous coronary intervention (PCI). The novel transradial access site, distal radial access (DRA), has gained popularity owing to improved patient and operator comfort, and faster hemostasis with shorter artery gauze compression. Despite the emerging technique and increasing amount of data in favor of preprocedural ultrasonography (pre-US) including DRA [1], the choice of the artery is still based on pulse recognition.
We present an illustrative case of a 75-year-old patient with typical exercise chest pain and a history of anterior myocardial infarction treated with PCI. The patient was admitted for scheduled coronary angiography (CA) via the right transradial approach. The radial pulse was palpated, typically 2 cm proximal to the radial styloid process of the right hand. The radial artery was punctured and cannulated with the standard 6F sheath. Due to pain during engagement, an arteriography of the forearm was taken, revealing a sheath in the narrow (1.5 mm) palmar superficial branch of the radial artery, and a wide radial artery in the anatomical snuffbox (Figure 1 A). CA revealed a critical distal right coronary artery (RCA) lesion and an intermediate left anterior descending (LAD) artery lesion. PCI of the distal RCA with drug-eluting stent (DES) implantation was performed, after the procedure, radial artery gauze compression was used, and the patient was scheduled for the next stage procedure with assessment of the LAD. After 1 month, the pulse in the right radial artery at a typical point was not palpable, whereas the pulse in the snuffbox was palpable. Doppler ultrasonography of the right upper extremity revealed a closed superficial palmar branch which was completely asymptomatic clinically with good flow in the main radial artery in the snuffbox (Figure 1 C, at the top) and ulnar artery (Figure 1 C, at the bottom). The procedure was successfully performed with 6F standard sheath from the snuffbox. Angiography of the upper limb circulation was performed (Figure 1 B), which confirmed a closed superficial palmar branch. Hemostasis was achieved using standard radial artery gauze compression. Ultrasonography after 2 weeks revealed good flow in the main radial artery in the snuffbox, with a lack of flow in the superficial palmar branch.
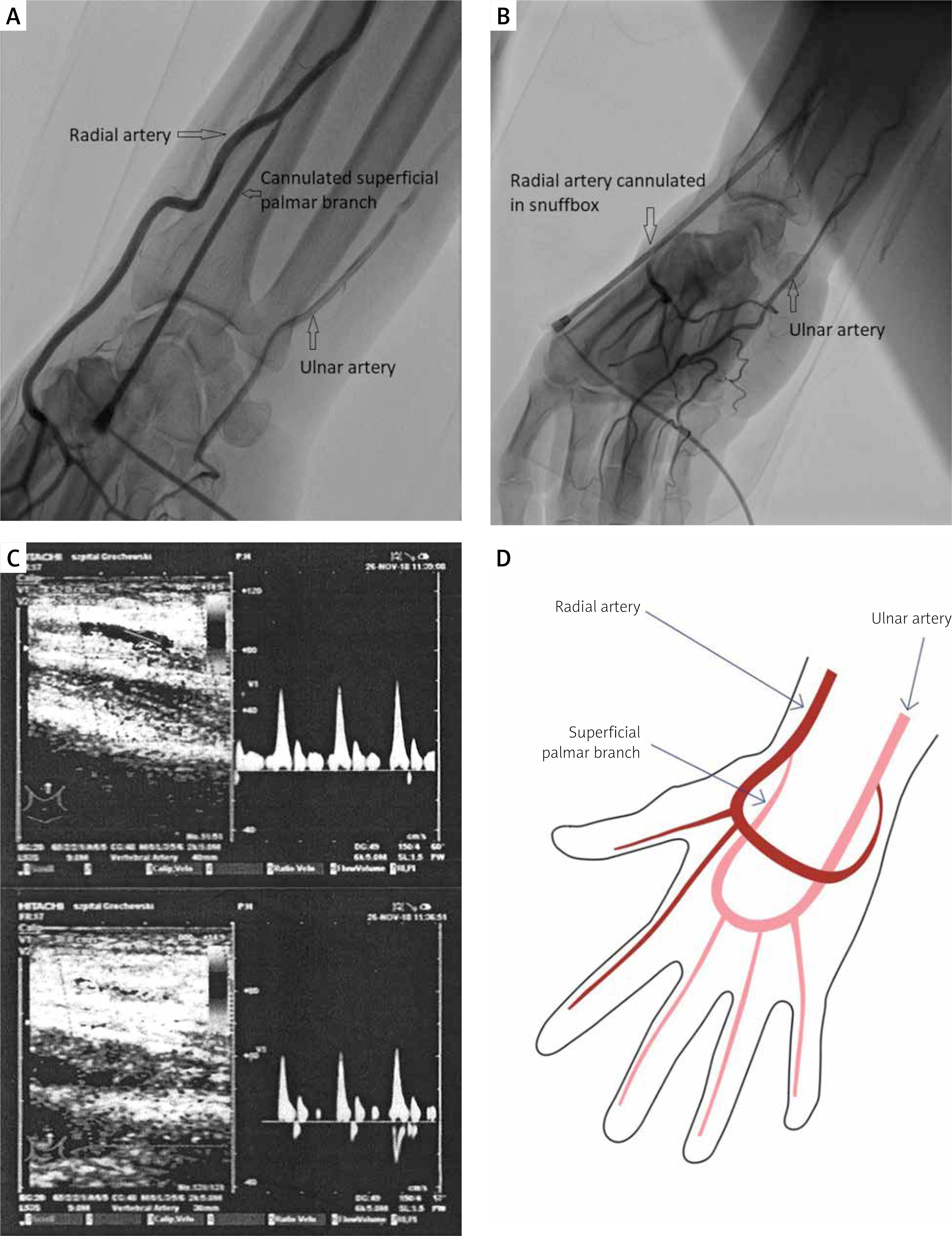
Figure 1
A – Arteriography of cannulated superficial palmar branch. B – Radial artery cannulated in snuffbox. C – Doppler ultrasonography of the right upper extremity with a closed superficial palmar branch, flow in radial artery at the top, flow in ulnar artery at the bottom. D – The palmar arch scheme
Knowledge of the arterial anatomy of the forearm, size, and abnormalities prior to invasive procedures can assist in preventing complications. The superficial palmar branch is usually smaller than 1.7 mm branch diverging lower than the puncture site, not considered to be an access artery; however, in this rare particular case, the superficial palmar branch diverged untypically high [2], with a good pulse recognition initially resulting in misleading puncture. Pre-US before RA is not a routine procedure, but we previously reported the usefulness of ultrasound in assessing the impact of pre-US selection of the dominant forearm artery on the incidence of vascular complications and also on the lower incidence of hand strength reduction [3, 4]. Ultrasound-guided larger diameter artery access was associated with a lower incidence of vascular complications. This case supports pre-US application in selecting between the radial and distal radial approaches.