

Purpose
Cervical cancer is the fourth most common cause of cancer incidence and mortality among women worldwide [1]. In India, cervical cancer is the second most common cancer among women, with around 123,992 new cases and 77,348 deaths per year accounting for 25% of global burden [2]. The possibility of advanced stages at presentation is due to age-standardized ratios of incidence and mortality, which are 14.9 and 2.9 per 100,000, respectively. However, this may also indicate delayed treatment time or sub-optimal access to treatment [3].
Worldwide, the average age at diagnosis of cervical cancer is 53 years. This early age generates proportionally a greater loss of life years [4]. In India, the current standard of care for locally advanced cervical cancer includes chemoradiotherapy and brachytherapy. It provides a 5-year overall survival of 83.5%, 80.6%, 66.0%, and 37.1% for stage I, II, III, and IV, respectively [5].
Brachytherapy plays an important role in the treatment of carcinoma cervix in terms of overall survival and local control, and it is usually delivered together with external beam radiation therapy (EBRT) or after completion of treatment. The administration of brachytherapy towards the end of treatment course allows for adequate tumor shrinkage, and hence smaller brachytherapy treatment volumes.
Brachytherapy has been compared with various conformal techniques, such as stereotactic body radiotherapy (SBRT) and intensity-modulated radiotherapy (IMRT); however, these techniques have not been proven to be a significant substitutes to brachytherapy [6]. A study by Barrett O’Donnell et al. evaluating SBRT, IMRT, and brachytherapy as boost in locally advanced cervical cancer among 15,905 patients found no significant difference in overall survival (HR = 1.477, CI = 0.746-2.926). A significant detriment to overall survival was seen in patients with IMRT boost (HR = 1.477, CI = 1.3-1.628). However, only 0.8% received SBRT, 9.2% received IMRT boost, and 90.5% of patients underwent brachytherapy in this study [7]. Therefore, SBRT and IMRT boost cannot be an alternative to brachytherapy. Studies have shown that overall treatment time (OTT) in carcinoma cervix starting from the beginning of EBRT to the end of brachytherapy should be less than 56 days, as it was found to negatively influence cause-specific survival and pelvic control rate [8]. The possible reasons for an increase in OTT could be multiple, including poor access to brachytherapy, inadequate maintenance of brachytherapy skills, insufficient training during residency, etc. [9]. A recent study showed that India has only one brachytherapy unit for every 42,93,031 population, with 21 states having a deficit of the same. They also reported that among 613 medical colleges in India, only 104 have brachytherapy facilities [10]. The 2023 update of IAEA directory of radiotherapy centers shows that India has 450 RT centers, with 692 MV therapies and 318 brachytherapy units. There are around 28 brachytherapy centers in Karnataka. Among these, 19 are present in Bangalore [11].
In this study, we presented the findings of a tertiary hospital serving as a dedicated referral center for patients diagnosed with locally advanced gynecological malignancies, specifically focusing on brachytherapy. Our department has observed a significant increase in patients’ referrals from other healthcare facilities for brachytherapy.
Material and methods
Study design and participants
This was a retrospective study to evaluate 130 patients diagnosed with locally advanced gynecological cancer referred for brachytherapy from January 2021 to January 2023. Inclusion criteria were all patients with a histologically proven diagnosis of locally advanced gynecological malignancy (squamous cell carcinoma, adenocarcinoma, or adenosquamous carcinoma), post-radical EBRT with concurrent chemotherapy referred for brachytherapy. Exclusion criteria were patients previously treated with brachytherapy, re-irradiation to the pelvis, recurrent gynecological cancer, or medically unfit for anesthesia.
Patients’ parameters, including age, tumor histology, tumor stage, treatment, EBRT technique, EBRT dose, chemotherapy drug and cycles, pre-brachytherapy disease status, and overall treatment time were recorded. Brachytherapy details, including date of procedure, technique, dose, fractions, dose-volume parameters of high-risk clinical target volume (HR-CTV), and organs at risk (OARs) were also documented.
Brachytherapy procedure
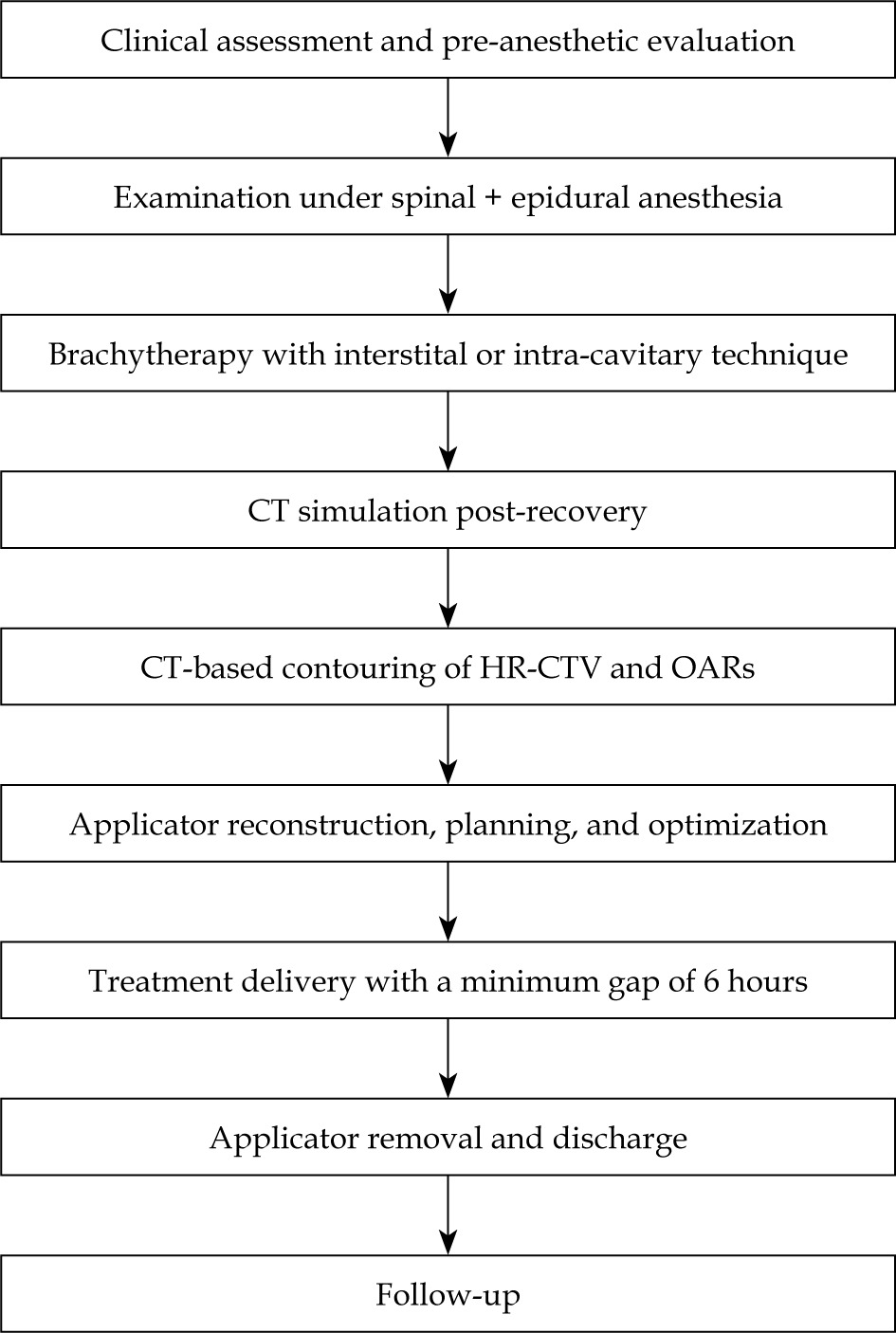
According to the department protocol (Figure 1), after completion of EBRT, patients were referred for pre-anesthetic examination. After anesthetic clearance, they were planned for interstitial or intra-cavitary brachytherapy under combined spinal and epidural anesthesia. All patients underwent examination under anesthesia (EUA) for a thorough assessment of the disease and its extensions. All patients were catheterized using a 14-Fr Foley catheter, and the bulb was inflated with 7 cc distilled water. A central tandem was applied in all patients with an intact uterus. Patients were considered for ISBT if they presented with a narrow vagina, bulky lesion of more than 4 cm, inability to enter cervical os, extension of the disease to lateral parametrium, or lower one third vaginal involvement. Guide needle was inserted to ascertain the depth of insertion and the coverage of beyond the disease. ISBT was performed using Syed-Neblett template insertion of needles through the perineum. Intra-cavitary brachytherapy was done using a Fletcher-Suit applicator. Post-procedure, computed tomography (CT) scan was performed for all patients, with 3 mm slice thickness. Bladder protocol was followed by filling 50 cc of normal saline administered through a Foley catheter prior to the scan. HR-CTV was contoured, including gross residual disease at the time of brachytherapy, cervix, and all suspected areas of residual disease at clinical examination and/or MRI (Figure 1). Organs at risk, including the bladder, rectum, and sigmoid were contoured. A dose of 6 Gy in 4 fractions or 7/7.5 Gy in 3 fractions was prescribed to HR-CTV based on EBRT dose and disease status at EUA. Treatment planning was done using HDR plus version 3.0.5 treatment planning system, delivered with BEBIG multisource brachytherapy unit. Inverse planning was performed with graphical optimization technique. Treatment planning aimed at delivering a minimum of 85 Gy to at least 90% HR-CTV (D90) after converting the total EBRT and brachytherapy dose to an equivalent dose of 2 Gy per fraction (EQD2) . Dose constraints for 2 cc volume of OARs were 75 Gy, 85 Gy, and 75 Gy for the rectum, bladder, and sigmoid, respectively . After approval of the plan, the treatment was delivered with a gap of minimum 6 hours for a dose of 6 Gy in 4 fractions or 7/7.5 Gy in 3 fractions. Following treatment, the applicator was removed, and the patient was discharged after 24 hours of observation for any complications. There was no complication observed in any of the patients treated. All toxicities were recorded according to national cancer institute common toxicity criteria for adverse events v. 5.
Results
Patients’ characteristics
Most of the patients (n = 130) were referred from nearby districts (89.4%). The mean age at diagnosis was 53 years. 77.27% of the patients were more than 45 years of age; 85.6% of the patients were diagnosed with carcinoma of the cervix, 1.5% with carcinoma of the vault, and 12.8% with carcinoma of the vagina. Most of the patients presented with an advanced stage of the disease. There were 3 (2.27%) stage I patients, 37 (28.03%) stage II, 89 (67.42%) stage III, and 3 (2.27%) stage IV patients. Majority of the cases presented with squamous cell carcinoma (85.6%), followed by adenocarcinoma (10.6%) and adenosquamous carcinoma (3.78%) (Table 1).
Table 1
Baseline characteristics
The median time interval between the last fraction of EBRT and the first evaluation at our hospital was 19 (range, 13-28) days (IQR). All patients received external beam radiotherapy with concurrent chemotherapy in their respective hospitals before being referred to our institution. EBRT doses varied between 45-50.4 Gy in 25-28 fractions, with concurrent chemotherapy as indicated. Patients with stage IIIC2 were given extended field radiotherapy. In the current study, 96.96% of the patients received cisplatin, and the remaining (3.03%) received carboplatin as concurrent chemotherapy. EBRT was applied using conformal techniques in 78 patients (59.09%), and in the remaining 54 (40.9%) patients, 2D technique was administered (Table 1). The median time between the completion of chemoradiation and the brachytherapy procedure was 25 (range, 19-33) days (IQR) (Table 2).
Table 2
Median time for referral
| Parameter | Median | Interquartile range (IQR) |
|---|---|---|
| Time to our hospital | 19 days | 13-28 |
| Time to brachytherapy | 25 days | 19-33 |
All patients underwent brachytherapy after completion of their EBRT, using either intra-cavitary or interstitial brachytherapy technique, receiving the prescribed dose of 6 Gy in 4 fractions or 7/7.5 Gy in 3 fractions with an interval of minimum 6 hours between fractions. On clinical examination, 80.4% (n = 106) had parametrial involvement. Among the 130 patients, 8 (6.08%) underwent intra-cavitary brachytherapy, whereas the remaining 124 patients (93.93%) underwent ISBT. 86 patients (66.15%) received a dose of 7 Gy in 3 fractions, 28 patients (21.5%) received 6 Gy in 4 fractions, and the remaining 16 patients (12.3%) received 7.5 Gy in 3 fractions. The mean HR-CTV volume was 37.3 ±11.09 cc. The D90 and D100 HR-CTV mean EQD2 dose was 28.34 ±2.78 Gy and 14.58 ±2.53 Gy respectively. The mean bladder, rectum, and sigmoid volumes were 150.2 ±89.1 cc, 38.8 ±18.09 cc, and 20.4 ±12.34 cc, respectively. The mean EQD2 dose to 2 cc of the bladder, rectum, and sigmoid was 18.31 ±5.19 Gy, 14.14 ±5.76 Gy, and 17.43 ±4.75 Gy, respectively (Table 3). The mean overall treatment time was 63.5 ±14.7 days. After 3-month follow-up, the patients were assessed for clinical and radiological response. 65 of the patients (49.24%) showed a complete response, whereas 56 (42.42%) achieved partial response. However, 8 of the patients (6.06%) had stable disease and 3 (2.27%) had progressive disease. At the end of the 3-month follow-up, no grade 3 or 4 toxicities were reported.
Table 3
Dosimetric parameters of brachytherapy
Discussion
The present study aimed at presenting the experience of a hospital serving as a referral center for brachytherapy in locally advanced gynecological cancer, with benefits and challenges associated with this role.
Brachytherapy alone had shown to improve cancer-specific survival and overall survival in locally advanced cervical carcinoma [12]. The American Brachytherapy Society (ABS) guidelines strongly recommend the use of brachytherapy as one of the treatments in locally advanced cervical cancer [13]. Brachytherapy has evolved from 2D to 3D, with image-guided brachytherapy showing major improvements in both local control and reduced normal tissue toxicity [14, 15]. In our study, all patients underwent image-guided brachytherapy as recommended, allowing maximum dose optimization to the tumor and minimum dose to OARs.
Although brachytherapy is strongly advised in the management of LACC, it is not without disadvantages. These include its invasive nature, intensive resource requirements, technical complexities, need for inpatient care, and preference for performing it in women with a good performance status [16]. These aspects are often considered as drawbacks by many medical centers. However, in our hospital, we have successfully embraced these challenges and implemented brachytherapy as a part of our comprehensive treatment approach for locally advanced gynecological malignancies. Although brachytherapy in cervical cancer is well-established, its application remains underutilized. A study by Ting Martin Ma et al. evaluating underutilization of brachytherapy in LACC reported that the reason for the same is widely recognized by ABS members, with inadequate training during residency and insufficient maintenance. Another factor contributing to the underutilization of brachytherapy is the non-availability of required equipment and infrastructure [8].
Our institute serves as a referral center for brachytherapy in locally advanced gynecological cancer patients from surrounding districts of Bangalore. The current study involved patients diagnosed with locally advanced gynecological carcinoma, who were referred from nearby hospitals post-EBRT and concurrent chemotherapy for brachytherapy. All the patients received external beam radiotherapy via 2D or conformal technique to a minimum dose of 45 Gy with concurrent cisplatin or carboplatin weekly, according to the current guidelines. A meta-analysis by Green et al. showed an improved overall survival and progression-free survival in patients treated with concurrent chemoradiotherapy in locally advanced cervical cancer [17]. In accordance with the American Brachytherapy Society guidelines, we have diligently followed the recommended treatment approach for our patients. To ensure the safety of critical structures, the mean dose to 2 cc volume of the bladder, rectum, and sigmoid were kept well within the tolerance doses of < 90 Gy, 70 Gy, and 70 Gy, respectively [18].
The completion of concurrent chemoradiotherapy in cervical cancer is recommended to be within 56 days [19, 20]. In the present study, the mean overall treatment time was 63.5 ±14.7 days, and only 27.27% of patients completed their treatment within the recommended OTT of 56 days. After a period of three months, we evaluated the response of these patients both clinically and radiologically, and observed that 49.24% of patients exhibited a complete response to the treatment, indicating a significant improvement in their condition. Additionally, we found that 42.42% of cases experienced a partial response demonstrating a noticeable reduction in the severity or extent of their condition. Also, in 3 patients, we observed progressive disease requiring the need for further investigation to understand factors contributing to treatment resistance.
At the end of the three months follow-up period, no patient reported experiencing grade 3 or 4 genitourinary or gastrointestinal toxicities, indicating that the treatment protocol used in our institute had a favorable safety profile.
The present study has a few limitations, firstly being that only patients referred to a single-institute were considered. Secondly, follow-up time was short, and hence local control and overall survival could not be evaluated.
Conclusions
This study demonstrates the importance of brachytherapy centers in India and difficulties associated with the same. Brachytherapy is a proven and effective treatment option in locally advanced gynecological cancer, and its availability can improve outcomes and reduce healthcare burden. However, due to its limitations, healthcare policy-makers should prioritize efforts to expand the access to brachytherapy by promoting referral to expert centers that specialize in IGBT. This also needs a well-defined workflow and appropriate allocation of resources to minimize overall treatment time. Furthermore, efforts should be made to develop the expertise in brachytherapy across all regions to increase the access to this crucial component of cancer treatment.