






Almost one fourth of the Polish population use tobacco products every day (30% of men and 21% of women) [1]. It is one of the most documented carcinogenic factors and it harms nearly every organ in the body. The skin manifestations of tobacco usage include yellow discoloration of fingernails, oral and gingival pigmentation, black hairy tongue, precocious skin aging and skin cancers [2]. Chronic ultraviolet exposure could also have a devastating effect on the skin leading to skin aging and cutaneous carcinogenesis [3]. The association of chronic tobacco usage with other skin damaging factors, like ultraviolet radiation, may cause extreme skin changes. We present an accumulation of skin disorders in a heavy smoking farmer, who due to his outside work was regularly exposed to sunlight, suffering from Favre-Racouchot disease (FRD), cutis rhomboidalis nuchae and skin carcinomas. The occurrence of all the above-mentioned diseases have a strong correlation with both UV radiation and smoking.
A 70-year-old Caucasian man was admitted to our department for the treatment of squamous cell carcinoma (SCC). Besides the ulceration on the lower lip, he complained of recurrent bilateral lesions on the face and increased marking of the skin on the neck. The lesions were not associated with any sensation, like pain or itch, but their increasing number started to make the patient concerned. He had no comorbidities. All his life he worked as a farmer and was a heavy cigarette smoker with 80 pack years. A year and a half before he had undergone an excision procedure of basal cell carcinoma (BCC) on his left temple area.
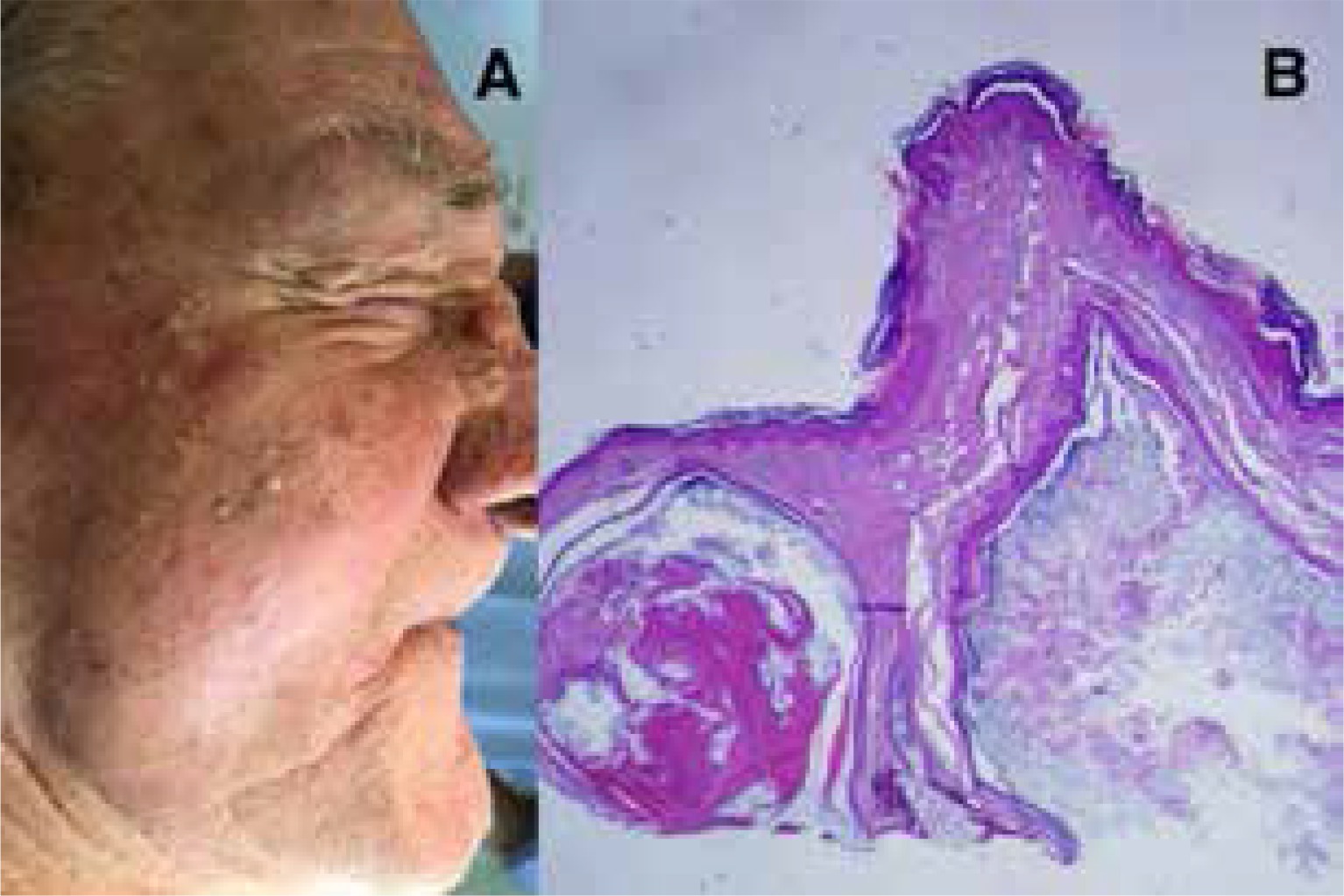
On admission, psychical examination revealed bilateral comedones on the man’s cheeks with multiple black- and whiteheads (Figure 1 A), an ulceration on the lower lip (Figure 2 A), telangiectasias, and generally damaged skin. Additionally, his bulbous nose was erythematous, with multiple yellow papules, nodules and cystic lesions. The skin on the patient’s neck presented deep wrinkles and leathery texture (Figure 2 B). The treatment consisted of surgical excision of the lip ulceration and extraction of bilateral comedones. The shave biopsy of the biggest nose lesion was taken to exclude possible rosacea. In the histopathological examination of the biopsy, structures resembling epidermal cyst were found (Figure 1 B), while examination of the ulceration confirmed SCC cut out with negative margins. The lymph nodes ultrasonography did not show any pathological changes. The patient was instructed to cease smoking and to avoid excessive sun exposure.
Figure 1
A – Multiple open and closed comedones, papules, cystic lesions and a nodule on the nose. B – The shave biopsy from the biggest nodule on the nose. The open epidermal cyst picture supports the diagnosis of the Favre-Racouchot disease

Favre-Racouchot disease, also known as senile comedones or nodular cutaneous elastosis with cysts and comedones, was firstly described in 1888 but was not well defined until 1951. It is a quite common, slowly progressive, underdiagnosed condition affecting up to 6% of Caucasian men older than 50 years of age [4]. However, there are reports of the disease occurrence in other ethnic and age groups [4, 5]. The pathogenesis is yet to be fully explained. Ultraviolet radiation (UVR) and chronic sun exposure serve the main role in the development of cutaneous atrophy with disrupted keratinization of the pilosebaceous follicle. Patients usually have a history of prolonged occupational or recreational outdoor activities. It is also believed that radiation therapy, physical agents and smoking may play a significant role in the development of FRD [6–8].
The disease is usually symmetrical, affects especially the face, periorbital and temporal areas [9], although there are cases of involvement of other sun exposed sites like the trunk, limbs, earlobes and neck [10]. It is clinically characterized by large, non-inflamed, black, white or yellow comedones, deep wrinkles, furrows and waxy plaques on affected zones. During the severe course, multiple papules and nodular cysts appear. The affected skin is frequently atrophic and has a yellowish colour [11]. Routinely, patients do not tend to complain about any associated subjective sensation like pain or itch, however, aesthetics could be the main problem. Additionally, the strong association between the risk factors of FRD and cutis rhomboidalis nuchae was reported. It is a sun-induced alteration of the skin in which UVR causes elastin and collagen fibres to degenerate. Due to those changes, skin acquires a leathery aspect and yellowish, extensively marked and wrinkled surface [12]. Although there are no many cases described, it is believed that those two diseases could occur together as they did in our patient [4]. Furthermore, other solar-induced disorders like SCC, BCC or actinic keratosis could coexist [4].
Habitually, the diagnosis of FRD is made on the clinical basis through a thorough examination but sometimes the biopsy is required. The histopathological examination usually presents signs of epidermal atrophy, basophilic degeneration and elastosis. The open or closed comedones often contain sebum, a large number of bacteria (mostly P. acnes), hair shafts and eosinophilic horny material. They are not inflamed, and this distinguishes them from acne comedones. The other characteristic feature is the shrinkage or even absence of sebaceous glands [4, 13]. The differential diagnosis should include colloid milium, actinic comedonal plaques, syringoma and trichoepithelioma.
No standard management for FRD can be found in the literature. The important part of the process is to avoid excessive sun exposure and discontinue smoking. During the conservative treatment, topical retinoids like tretinoin or tazarotene gel are commonly used. The exfoliative actions, the ability to cause expulsion of lesions and to reduce “aged” appearance of the skin made them a popular option for mild courses. Although the retinoids have been proven useful, in more severe cases doctors tend to use them as a complement to other techniques [10]. Invasive treatment involves use of carbon dioxide laser, comedo extraction and plasma exeresis. Surgical excision is reserved for severe cases with functional impairment or when the associated malignancy cannot be excluded. The invasive treatment is usually effective, and due to higher compliance, has better clinical outcome. However, if the risk factors persist, the lesions of FRD tend to relapse after 1 year [10].
In conclusion, we presented a rare case of the coexistence of FRD, cutis rhomboidalis nuchae and skin cancers as a result of the carcinogenetic factor accumulation in 1 patient. This case seems to be a perfect example of chronic, multifactorial skin damage. In such patients, the thorough examination, quick treatment and patients’ education are keys in the holistic management.