
Introduction
Vitiligo is a skin pigmentation disease that causes the destruction or loss of function of skin melanocytes through many mechanisms. The global prevalence of vitiligo is 0.06–2.28%. More than a half of these cases occur before the patient reaches the age of 20 years [1]. In addition, children with vitiligo often have anxiety, an inferiority complex, and depression due to their unusual appearance. Therefore, these patients, encouraged by their parents, eagerly seek treatment to improve their body image, aesthetic appearance, and general health. The pathogenesis of vitiligo remains undetermined, and the optimal treatment option remains unelucidated. When treating children, dermatologists must carefully choose treatment methods to achieve the best effects and reduce the likelihood of side effects because children’s skin has different structures and responds differently to medications than adults.
Aim
We aimed to investigate the clinical effect and influencing factors of a 308-nm excimer lamp combined with 0.03% tacrolimus ointment for treating children with non-segmental vitiligo.
Material and methods
In this study, we analysed clinical data, including patients’ characteristics (Table 1), the frequency of the 308-nm excimer lamp treatment, dose, and adverse reactions, in 73 children with non-segmental vitiligo who received treatment between June 2018 and December 2020. Vitiligo is an acquired, idiopathic pigmentation disorder of the skin. For each patient, a standardized evaluation included careful examination in both daylight and using Wood’s lamp. The patients were treated with 0.03% tacrolimus ointment twice a day and with a 308-nm excimer lamp once a week. Initially, we tested the minimal erythema dose (MED). The lowest possible treatment dose was set to avoid phototoxic reactions. Starting from the second treatment, the dose of each treatment was determined by referring to the duration of the previous treatment and subsequent erythema. If the erythema disappeared within 24 h after the previous treatment, the next dose was increased by 50 mJ/cm2. If the erythema was present for 48 h after the previous treatment, treatment was stopped until the reaction subsided and then continued by delivering 80% of the previous dose. If blistering and burning pain occurred, treatment was stopped until the reaction disappeared, MED was re-measured, and treatment was resumed according to the revised plan. One course of treatment included 20 sessions with the 308-nm excimer lamp therapy, with 1-month interval between two courses. Treatment with tacrolimus ointment was continued between the two courses. The lesions were irradiated once weekly, and any adverse reactions were recorded. During the 308-nm excimer lamp treatment process, patients, families, and therapists were required to wear goggles for personal protection.
Table 1
Patients’ characteristics
Observation criteria, evaluation criteria, and efficacy determination
The efficacy of treatment was assessed based on the following endpoints: the percentage of skin repigmentation, the response rates of the vitiligo lesions at various sites, and recurrences were also noted. Treatment efficacy assessment based on clinical examination and photography evaluation (Canon EOS 750D, Tokyo, Japan) was done in a blinded manner at the baseline pretreatment visit and once a month thereafter until the end of the study (Figure 1). The percentage of skin repigmentation assessment was performed by two physicians who did not follow the course of phototherapy. Repigmentation was graded on a 6-point scale as follows: 0 for no repigmentation, 1 for poor up to 25% of the affected area, 2 for 26% to 50%, 3 for 51% to 75%, 4 for 76% to 99%, and 5 for 100%. In cases of disagreement between the two physicians, a second evaluation was done together. If disagreement persisted, the lowest evaluation grade was chosen. Treatment efficacy was scored in four grades according to the 6-point scale: Return to Normal, Significant Improvement, Partial Improvement, or No Improvement. “Return to Normal” was defined as repigmentation of grade 5. “Significant Improvement” was defined as repigmentation of grade 3 or 4. “Partial Improvement” was defined as repigmentation of grade 1 or 2. “No Improvement” was defined as repigmentation of grade 0 or expansion of the affected area was noted. The efficiency rate was calculated as follows: Efficiency rate = (number of “Return to Normal” cases + number of “Significant Improvement” cases)/total cases × 100%.
Figure 1
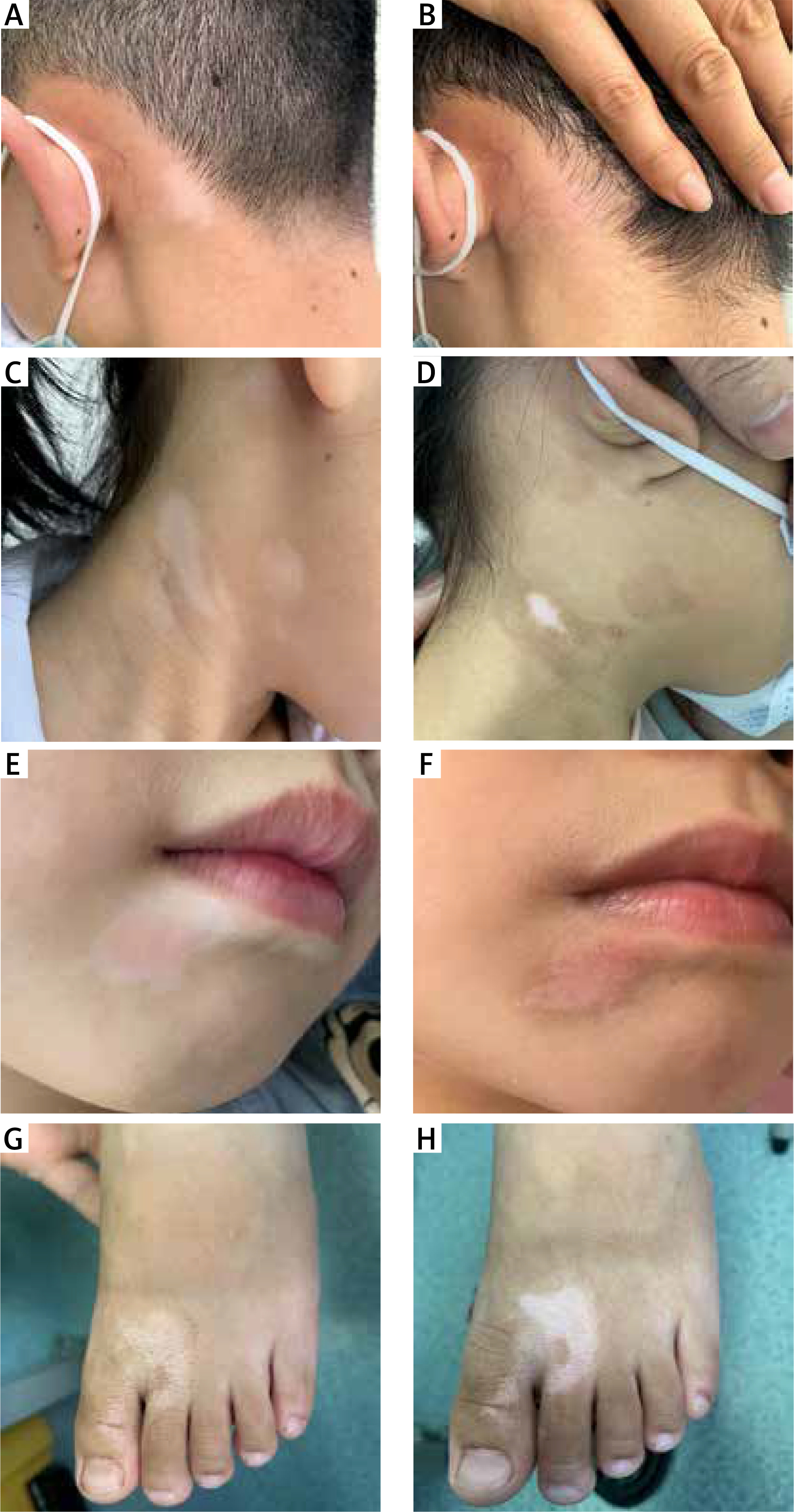
A – Patient showing a vitiligo lesion on the neck before the excimer lamp treatment. B – The same patient showing that the skin had returned to its normal colour after two courses of treatment. C – Patient showing multiple vitiligo lesions on the neck before the excimer lamp treatment. D – The same patient showing significant improvement after two courses of treatment. E – Patient showing a vitiligo lesion on the face before the excimer lamp treatment. F – The same patient showing partial improvement after two courses of treatment. G – Patient showing a vitiligo lesion on the foot before the excimer lamp treatment. H – The same patient showing no improvement with expansion of the affected area after two courses of treatment
Results
Post-treatment findings
The clinical characteristics of 73 patients with 105 leukodermas are summarized in Table 2. The onset ages of the patients ranged from 3 to 13 years (median: 9 years). The median disease duration was 7 months (range: 1–22). The mean onset of action was 16.2 ±2.1 days. The most common site was trunk (36.2%), and other involved locations were the face and neck (24.8%), hands and feet (20.9%), arms and legs (18.1%). The median number of treatment sessions was 36 (range: 4–78), and the median duration of treatment was 10.5 months (range: 1–24). Treatment was effective in 86 leukodermas with an efficiency rate of 81.9%. Thirty-eight leukodermas were fully cleared after treatment, with a clearance rate of 36.2%.
Table 2
Clinical parameters of 73 patients with non-segmental vitiligo in this study
The treatment was most effective in the face and neck areas, followed by the trunk, limbs (arms and legs), and extremities (hands and feet), in that order. The efficiency rate of the face and neck treatment was significantly higher than that of the limb and extremity treatment. The Kruskal-Wallis rank-sum test results indicated that the efficiency rate of the face and neck was significantly different from that of the limbs (p = 0.022, p < 0.05; Table 3). In multivariable analysis, patients with non-segmental vitiligo with a short disease duration showed a better response (Table 4). After 15 weeks of treatment, the efficiency rate decreased. After the first course of treatment, radiation therapy was suspended for 1 month, during which 0.03% tacrolimus ointment was applied twice a day. The second course of treatment exhibited a high-efficiency rate followed by recovery. Treatment was discontinued after pigmentation normalized completely. However, recurrence was observed in 3 cases, with an average recurrence time of 207.6 days.
Table 3
Efficacy and cumulative dosage according to the site of the lesion
Table 4
Prognostic factors influencing the response of patients with non-segmental vitiligo (n = 73)
Adverse reactions
Adverse reactions included local blisters (1, 0.9%), pruritus (23, 21.9%), peeling (26, 24.8%), burning sensation (14, 13.3%), and erythema (15, 14.3%). Blisters were treated with mupirocin ointment; the symptoms of other adverse reactions were relieved by applying emollient. The minimum erythemal dose was re-measured, and a modified regimen was continued in the treatment group; thereafter, no further blistering was observed.
Discussion
In recent years, treatment with a 308-nm excimer lamp has been gradually promoted as an option for treating various skin diseases. The 308-nm excimer lamp is a type of the excimer lamp that uses xenon chloride as the irradiation source. Importantly, it has a single wavelength and a high energy output and is considered the best ultraviolet lamp for vitiligo treatment. Vitiligo is characterized mainly by the destruction of melanocytes in the epidermis. However, because hair follicles have the same immune privilege as other privileged body parts that contain melanocytes, such as the brain, eyes, and inner ear, melanocytes in hair follicles are usually retained. Melanocyte stem cells in hair follicles can be used to replenish the epidermis of vitiligo lesions with newly differentiated functional melanocytes [2]. Therefore, there are two main objectives when treating vitiligo: suppression of autoimmunity and promotion of hair follicle melanocyte regeneration.
Studies have confirmed the role of cytotoxic T cells in the pathogenesis of vitiligo [3, 4]. A 308-nm excimer lamp can induce local infiltration T-lymphocyte apoptosis [5], promote Langerhans cell antigen uptake, and influence the downregulation of cytokines activity [6], such as interleukin and tumour necrosis factor, thus reducing the damage to melanocytes. Studies have reported an increase in the expression of tyrosinase and microphthalmia-associated transcription factor during irradiation with a 308-nm excimer lamp. These can stimulate the directional differentiation of epidermal melanocytes and were found to be significantly increased in cells, especially those in the hair root sheath outside the hair follicle, to produce more melanin [7]. These are then delivered to the skin site with pigment loss [8]. It is widely believed that tacrolimus plays a therapeutic role as an immunomodulator by inhibiting calcineurin in T cells, preventing the production and release of various pro-inflammatory cytokines [9]. Tacrolimus also inhibits the synthesis and release of tumor necrosis factor-α (TNF-α) and interferon-γ (IFN-γ), thus directly enhancing the proliferation of melanocytes [10] and promoting their migration by increasing the production of stem cell factors [11]. Our results suggest that the concurrent treatment of topical tacrolimus seemed to have contributed to a high repigmentation rate. However, further controlled clinical trials are needed to confirm these observations. Patients with non-segmental vitiligo with a short disease duration showed a better response to topical tacrolimus and the 308-nm excimer lamp than patients with a longer disease duration. Hence, early detection and early treatment are imperative for better treatment outcomes. The total number of combination treatments was positively correlated with the efficacy, which is consistent with the results of relevant studies [12]. Three patients with complete pigment regeneration experienced a recurrence of lesions 6 months after discontinuation of treatment. In recent years, tissue-resident memory T cells have been discovered to be long-lived non-migratory memory cells residing in most non-lymphoid tissues (including skin) and are actively involved in the long-term process of reversing vitiligo [13]. It has been suggested that some patients may need to undergo treatment for an extended period to recover and maintain remission even after the skin lesions achieve a normal colour. However, maintenance therapy remains controversial, and studies with larger sample sizes and analyses are required to determine its impact.
Long-term irradiation using a 308-nm excimer lamp has some limitations, and the following should be considered: first, this treatment affects the healthy skin adjacent to the affected area; second, patients usually need to go to the hospital for treatment which adds to the time and the economic cost required of patients; finally, the impact of long-term treatment is still unknown. The DNA damage induced by this monochromatic irradiation has not been adequately probed. Some studies indicate that the excimer lamp is a non-coherent light source [14]. It remains unclear whether this may cause the modalities to affect the skin differently. Shorter wavelengths are believed to have more significant risks of erythema as well as carcinogenesis [15]. Multiple animal experiments have confirmed that UV, directly and indirectly, induces DNA lesions, which cause genetic mutations and trigger inflammation and immunosuppression, promoting tumour growth [16]. However, there is no evidence of the precise risks of UV. Moreover, long-term follow-up data on patients treated with 308-nm excimer lamps are lacking. Thus, there is no unified consensus on the specific implementation of maintenance therapy. In our study, after 15 weeks of treatment, the increase in efficiency rate slowed, which may be due to an increased inflammatory response to the increased light tolerance of human melanocytes following long-term irradiation using a high-purity ultraviolet lamp. Therefore, the curative effect is often reversed after suspending radiation therapy. Adverse reactions were mild and were relieved with appropriate treatment. One case with a local blister occurred during the summer. The case was a five-year-old male with leukoderma on the left forearm. It cannot be ruled out that an increase in sun exposure during outdoor sports increases the influence of skin phototoxicity. To reduce the occurrence of such adverse reactions, in addition to selecting the minimum amount of erythema and increasing the treatment dose carefully, we suggest that family members should be instructed on the application of sunscreen to the excimer light treatment area daily in summer. We observed that patients typically experienced only a slight heat sensation during treatment. These treatments were well tolerated, especially by children.
This study has several limitations. The study’s sample size was relatively small, and some patients’ data may have been missing or incomplete. Therefore, more studies with a low risk of bias and larger sample sizes are needed to verify the results of our analysis. We believed the study was a supplement to the experience of treating children with vitiligo.







