
A 38-year-old woman was referred to our dermatology department with a 3-month history of disseminated grey-brown macules located on limbs, which extended rapidly to the trunk. She had an occupational history as an orchard farmer and no history of medication. Initially one or two light brown macules appeared on her forearms (Figure 1 A) with mild pruritus and gradually spread and developed into grey-brown patches on the chest and abdomen (Figure 1 B). The oral mucosa and nails were not involved. A biopsy specimen was taken from a macule on her abdomen. Histopathology revealed epidermis atrophy, basal layer vacuolization, lymphocytic band-like infiltrate and marked pigmentation incontinence in superficial dermis (Figures 1 C, D). The routine laboratory data were within normal limits or negative. Based on clinical and histopathologic findings, these clues favour the diagnosis of generalized lichen planus pigmentosus (LPP). Drugs including potent topical corticosteroids, oral steroids, topical calcineurin inhibitors and skin-lightening agents were recommended for LPP. The patient got a relief after 2 months by using topical corticosteroids.
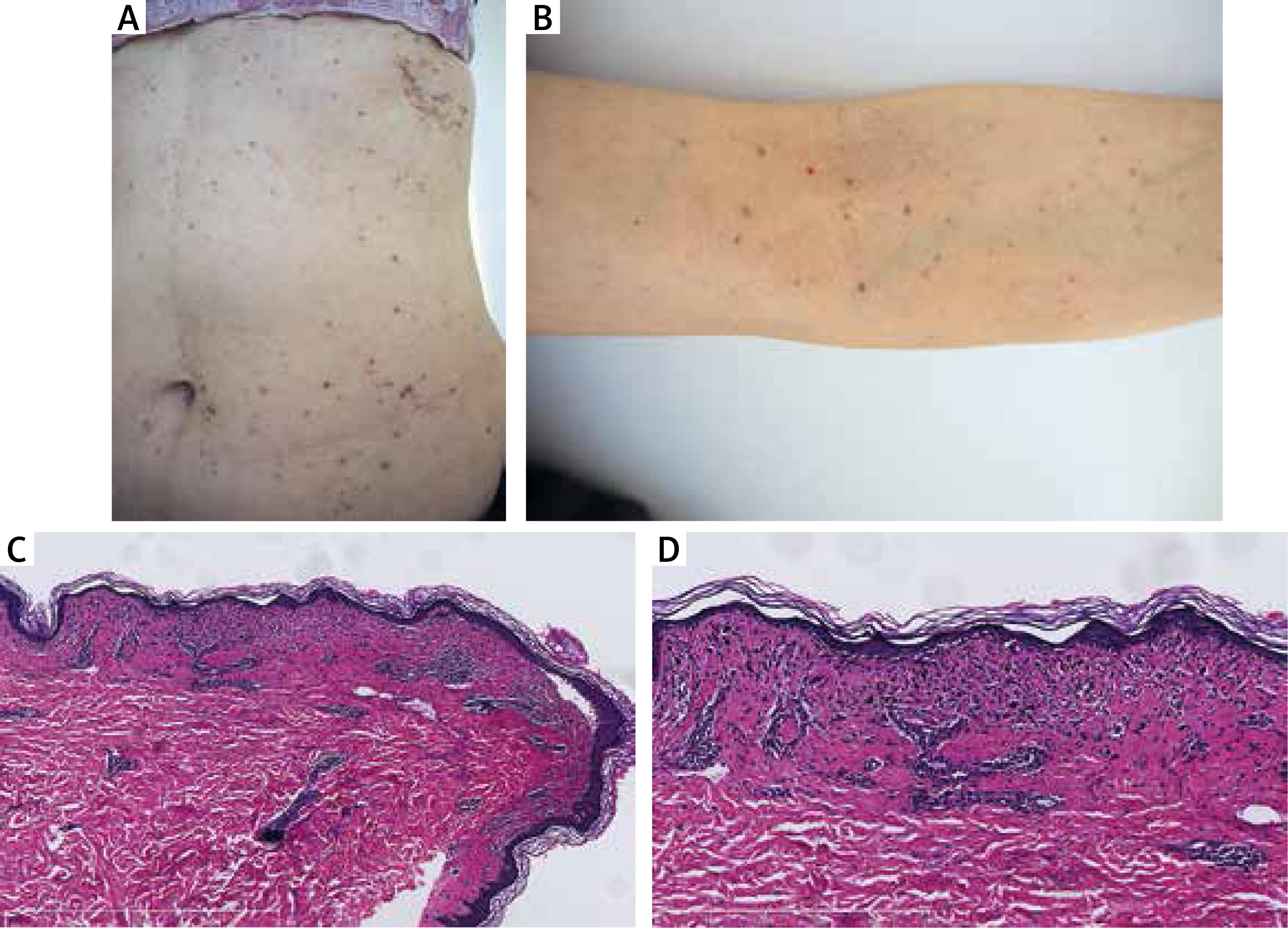
Figure 1
Oval grey-brown patches and macules located on the abdomen (A) and extremities (B). Histopathology of the skin lesions showed thinning of the epidermis, a superficial band-like lymphocytic infiltrate with basal layer vacuolization and pigmentation incontinence in superficial dermis HE ×100 (C) and HE ×200 (D)
LPP, defined as an exclusive form of lichen planus, is a chronic skin disorder of unknown aetiology characterised by irregular brown macules and patches, often confined to sun-exposed area and intertriginous areas [1]. Compared with lichen planus, LPP is usually asymptomatic without involving the scalp, nail and mucosal and shows thinning of epidermis and pigmentary incontinence in histopathology. Considerations in the differential diagnosis include ashy dermatosis, post-inflammatory pigmentation and drug-related dermatoses such as fixed drug-eruptions. Generally, a fixed-drug eruption is pruritic with a short interval after medication intake companying vesiculobullous eruptions [1]. Additionally, a fixed-drug eruption usually shows a well-defined oval or round-shaped oedematous erythema or isolated plaque repeatedly occurring at the same site. The present patient had no history of suspicious or doubtful medication before the onset and the brown macules are quite atypical to post-inflammatory hyperpigmentation. Clinically, ashy dermatosis is more often observed as disseminated macules initially with an asymptomatic active elevated red border and has a chronic course, lacking a well-defined histopathologic feature [2]. In the current patient, the eruptions were asymmetrically diffused over the trunk and flexures, suggesting LPP and not ashy dermatosis.
Furthermore, based on the previous reports, there are five types of eruption distribution of LPP, which include diffuse, reticular, blotchy, linear, and perifollicular distribution [3]. At present, most of these report cases are diffuse and reticular distribution types showing symmetrical distribution over the sun-exposed area. Because of the patient with a long-term history of outdoor occupation, we consulted her whether the lesion area was exposed to the sun during work. However, there was no obvious relationship between sunburn exposure and LPP, because she wore long sleeve overalls on weekdays. Since LPP could be triggered by topical agents, we then consulted her whether the progression of the lesion was related to the exposure to agricultural chemicals. The patient admitted she has used agricultural chemicals before the onset of LPP, but seldom in direct contact with the skin and this did not obviously aggravate the development of lesions during the course of the disease. Therefore, we think the exposure of agricultural chemicals might represent a predisposing causative factor for LPP.
This case exhibited an atypical clinical variety of LPP, including a wide region of grey-brown patches occurring on the trunk and the extremities without involvement of oropharyngeal mucosa. The patients with this type of lesions are prone to have the diagnosis of other pigmentary disease considered. The possible reason could be that the treating dermatologists might not pay attention to screen for LPP. Our case reminds us the atypical generalized eruption distribution of cutaneous pigmentation over the trunk should considered the diagnosis of LPP.







