
Basal cell nevus syndrome (BCNS) is a rare autosomal dominant disorder, and is believed to be caused by mutations in the PTCH gene at locus 9Q22.3-Q31. It is a complex syndrome and consists of multiple odontogenic keratocysts, multiple basal cell nevus (cancer) of the face and neck, punctate depression of the palm and sole, abnormal skeleton and rib, calcification in the brain and various other defects [1, 2]. Now we are reporting a case of BCNS seen in our department recently as follows: female, 20 years old, with typical clinical manifestations of BCNS: multiple and scattered pigmented nevus on the face (Figure 1 A), small depression on the palm (Figure 1 B), multiple cysts on the upper and lower jaw, calcification of cerebral falx and tentorium, sternum deformity, rib bifurcations, scoliosis, deviation of the right eye with decreased vision. The mother presented with multiple cysts of the upper and lower jaws, bifurcated ribs, scoliosis and scattered small depressions in the palm (Figure 2).
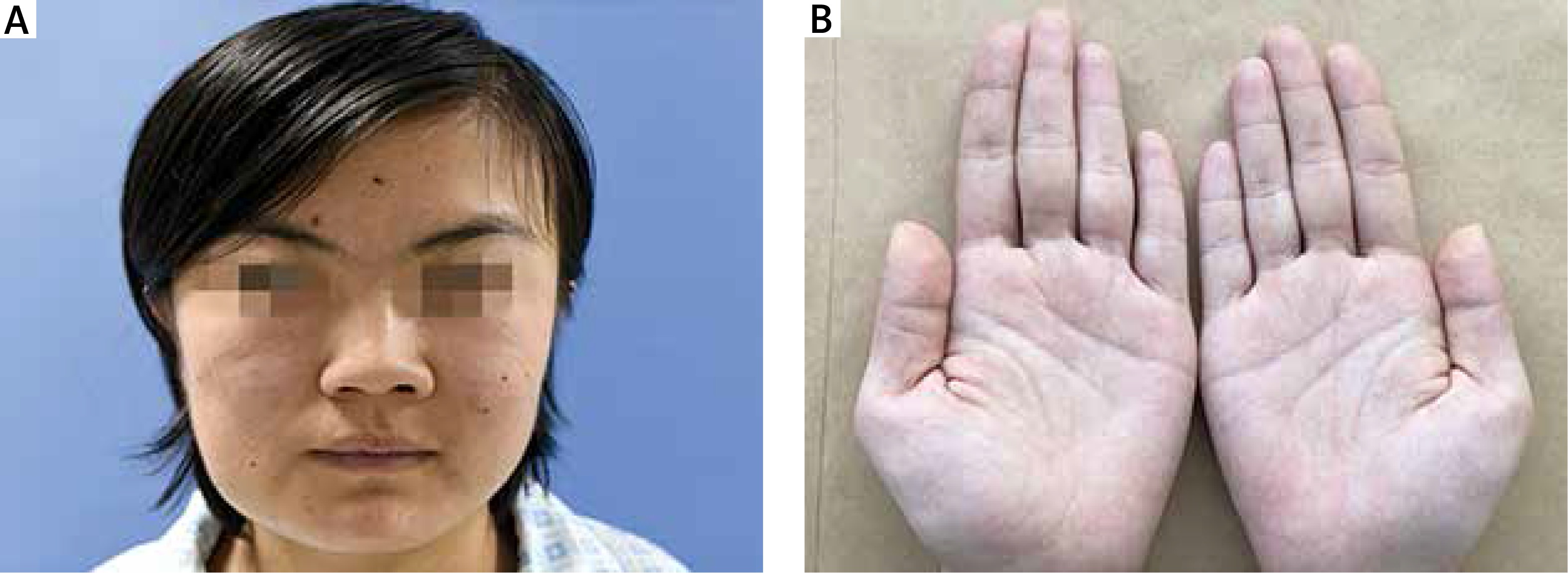
Figure 1
A – Multiple and scattered pigmented nevi on the face of patients. B – Small depressions in the palm of the patient

As early as 1894, Jarisch and White described patients with features typical of the autosomally inherited syndrome now known as basal cell nevus syndrome (BCNS, also known as Gorlin syndrome). In 1960, Gorlin and Goltz first systematically described the disease [3], believing that the disease is a special disease in its genetic form. The incidence rate is about 1/56000 [4], and the incidence rate of male to female is approximate [5]. At the gene level, the hedgehog signalling pathway is the main signalling pathway involved in the pathogenesis of BCNS [6, 7]. PTCH1 and G protein couple, together with the secondary receptor smoothed (SMO), regulates the hedgehog signalling pathway, which leads to the growth of basal cell carcinoma [8]. With the deepening of research, PTCH1 is considered as a new diagnostic standard [9], which plays an important role in the pathogenesis of BCNS, especially in patients younger than 20 years old. However, the PTCH1 gene cannot be detected in all patients, and PTCH2 and SUFU genes can be detected in a few patients [9].
BCNS can be accompanied by more than 100 kinds of symptoms and signs, mainly involving the skin, central nervous system, bone system, etc. Basal cell nevus (cancer) is a common clinical manifestation among patients with BCNS, and it cannot be ignored clinically, and can occur in all age groups, especially before the age of 35. About 10% of BCNS patients, especially those with dark skin and limited sunlight, have not developed any basal cell cancer; clinically, it is often multiple, occurs in the face and back, but also in other parts of the body [10]. Surgical treatment, microsurgery, photodynamic therapy, laser therapy and local chemotherapy are commonly used in the treatment of basal cell nevus (cancer) [11]. The latest research shows that photodynamic therapy is a good non-cicatricial treatment, and red light (635 m) and blue light (400 mm) have a good therapeutic effect [10]. For a long period of static state of asymptomatic nevus can be regularly followed up, regular follow-up, carried out, and close observation should be carried out to reduce some risky factors. However, if the nevus suddenly increases, any local ulcer, surface crack and other phenomena occur, the chance of canceration is relatively high, and timely treatment should be started, requiring surgical treatment. With the continuous development of new and old technology, there are various treatment methods for basal cell nevus (cancer). In addition to the commonly used treatment methods, we should improve the patients’ awareness of prevention, that is, try to reduce the sun exposure, and do a good job of sunscreen (sunscreen, sunglasses, sunscreen clothes) when going out.







