
Introduction
Cutaneous T-cell lymphomas (CTCL) constitute a rare, heterogeneous group of extranodal T-cell lymphomas that primarily originate in the skin [1]. Patients experience a wide range of symptoms, primarily pruritus, cutaneous hypersensitivity, skin irritation, pain and sleep disturbances [1]. All of these symptoms lead to fatigue, which is perceived by more than half of patients diagnosed with mycosis fungoides (MF) and Sézary Syndrome (SS) [2]. Studies that measure quality of life (QoL) in CTCL use a variety of instruments. The most popular and valid instrument is Skindex-29 [1, 3]. However, there is an unmet need for a specific, widely used tool that measures all aspects of QoL in CTCL. Neither Skindex-29 nor the specific MF/SS-CTCL instrument satisfies this need [1, 3–5]. Furthermore, QoL of CTCL patients perceived by doctors has never been previously measured to the best of our knowledge.
Aim
Therefore, the aim of our study was the quantitative and qualitative evaluation of QoL of the Polish CTCL patients and doctors and checking the impact of the disease on their daily functioning.
Material and methods
Study design
Structured anonymous questionnaires have been presented to Polish patients with the diagnosis of CTCL and physicians taking care of them. The study design and results are reported according to the STROBE statement [6].
Setting
Patients with a diagnosis of CTCL were recruited in the 18 Polish outpatient and inpatient clinics. Diagnoses were made according to established clinical, histological and immunohistochemical criteria, and the classification according to the WHO–EORTC criteria [7]. A questionnaire and Skindex-29 survey were administered between January and March 2019 to 67 patients with CTCL and 20 physicians.
Participants
Patients aged 18 years who agreed to participate, were included in the study. Physicians enrolled patients who met the inclusion criteria: patients with MF or SS, which are subtypes of CTCL and were treated in the PL B.66 programme. This includes those who completed treatment in the PL B.66 programme and those who did not qualify for the PL B.66 programme, but from a medical perspective, the use of bexarotene therapy was justified in their case. Moreover, we included patients with primary cutaneous anaplastic large cell lymphoma (pcALCL) or other CTCL subtypes who have experienced the disease. From all of the above groups of patients we have only qualified patients, who have already surpassed radiation and topical therapy steps.
Variables
The questionnaire was designed based on interviews with two medical professionals, experts in the field, and 2 patients in November and December 2018. The questionnaire (Supplementary Information 2, 3) covered various aspects of life, including the diagnostic process, physical domain, emotional domain, health care system, impact on interpersonal relationships, impact on professional work, and sources of support and information about the disease. The questionnaire consisted of various types of questions with different response options, including closed (yes or no), rating on a scale from 1 to 6, and open-ended questions.
Data sources/measurement
Patients have filled the questionnaire and Skindex-29 survey personally during the appointment with the doctor.
Bias
The questionnaires were designed based on interviews with experts in the field and patients. However, they have not yet been validated.
Study size
67 anonymous completed questionnaires from CTCL patients have been collected, and 20 from the surveyed physicians, who have actively participated in the diagnostic and therapeutic process of the patients (11 haematologists, 5 dermatologists and 4 oncologists).
Quantitative variables
The survey includes several quantitative variables, such as the demography of the studied population, questions on various aspects of life of CTCL patients such as: impact of the disease on daily life, physical functioning, emotional and professional aspect, and the Skindex-29 survey.
Results
Sixty-seven questionnaires were collected from the patient group, and 20 were collected from the physician group. Table 1 summarizes the demographics of the patients cohort. The mean age of patients in our cohort was 60 years old and the majority were male (63% of patients). The most common diagnosis among our group was MF (67% of patients). Only 25% of patients have higher education. Most of our patients live in a two-person household with their partner/wife, who also serves as their caregiver for daily activities and treatment (64% of patients). On average, our patients have one child who is no longer dependent on them.
Table 1
Patient demographics
| Variable | Number (%) |
|---|---|
| Sex | |
| Female | 25 (37.32) |
| Male | 42 (62.68) |
| Age, mean | 60 |
| Education | |
| High school or less | 36 (53.74) |
| Associate or bachelor’s degree | 14 (20.89) |
| University graduate or professional degree | 17 (25.37) |
| Place of residence | |
| City >500 000 inhabitants | 17 (25.37) |
| City 200 000-500 000 inhabitants | 12 (17.91) |
| City/Village <200 000 inhabitants | 35 (52.23) |
| Other | 3 (4.49) |
| Employment | |
| Actively working | 29 (43.28) |
| Not working | 37 (55.22) |
| Other | 1 (1.50) |
| Time since onset of symptoms | |
| < 4 years | 31 (46.46) |
| 4–10 years | 28 (41.60) |
| > 10 years | 8 (11.94) |
| Time of CTCL diagnosis1 | |
| < 6 months | 34 (50.74) |
| 6–24 months | 17 (25.37) |
| > 24 months | 16 (23.89) |
| Type of CTCL | |
| MF | 45 (67.16) |
| SS | 12 (17.91) |
| pcALCL or LyP | 8 (11.94) |
| Other | 2 (2.99) |
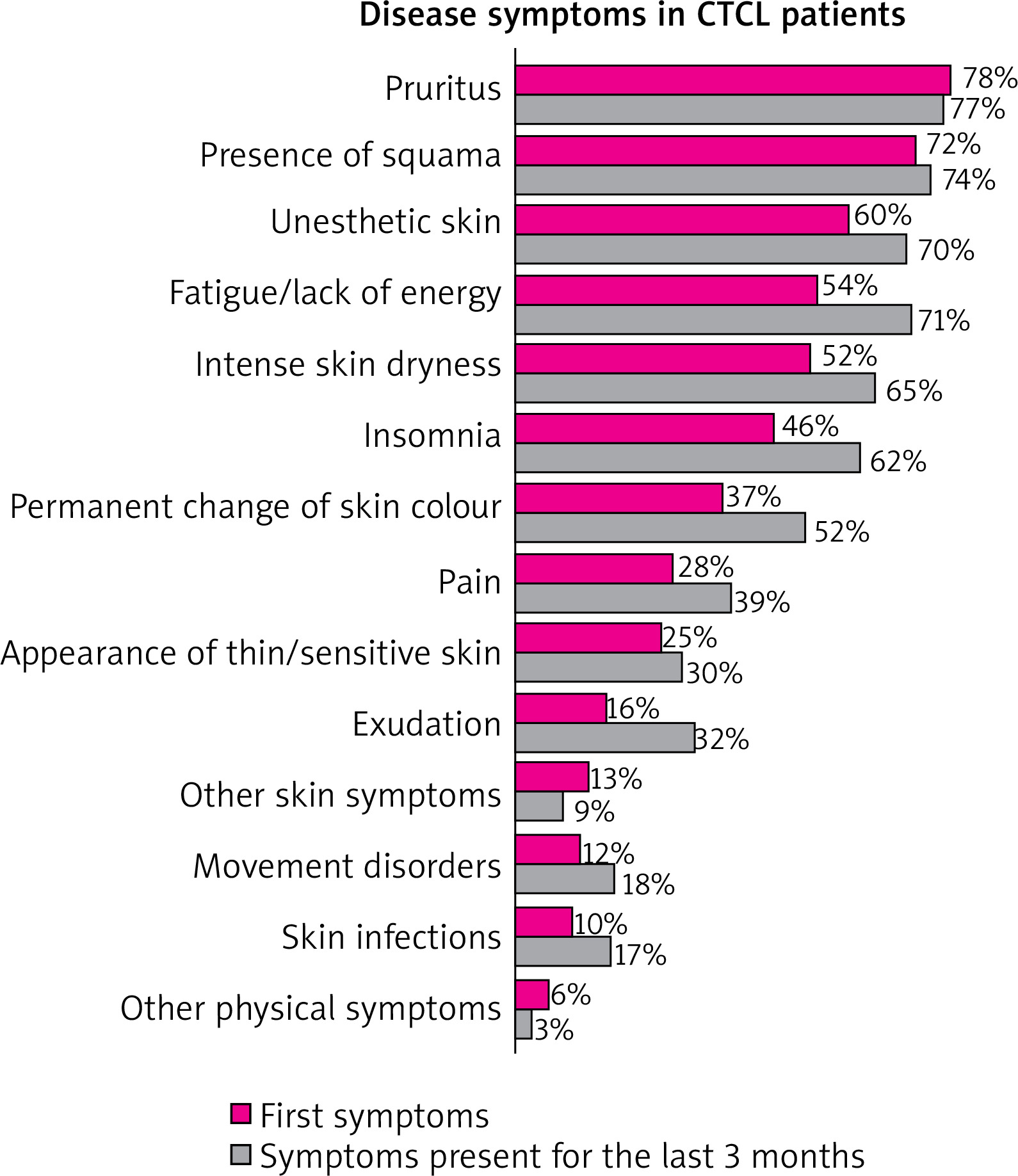
38% of patients find the efficiency of the diagnosis process efficient, while 34% find it inefficient and 28% of patients have been in between. Nevertheless, the majority of patients (70%) believe that the process took too long. Additionally, 74% of patients experienced fear when they were informed about the diagnosis, they “feared the worst”. Despite this fear, 76% of patients trust the doctor and feel that the doctor taking care of them knows what to do at the time of diagnosis. The final diagnosis was made on average after consulting three different doctors/specialists. The disease has lasted on average 2 years and 9 months from the first visit to correct diagnosis, but in as many as 28% of cases, it lasted longer than 2 years. The first symptoms that led the patient to seek medical attention (multiple choice question) were pruritus (78%), presence of squama (72%), and unsightly appearance of the skin (60%). Additionally, they may experience symptoms affecting the entire body, including weakness, lack of energy, and sleep disturbances. Figure 1 displays all patient reported symptoms.
The most significant inconvenience for patients (open-ended question) is related to commuting to another city for a doctor’s appointment (58%) and the amount of time spent on visits and tests. In Poland, doctors who treat CTCLs are typically only found in large cities where academic centres are located. Doctors have responded similarly by pointing to commute to another city (50%) and costs of travel (35%) as the most inconvenient to their patients. 73% of patients do not report any issues with purchasing specialized ointments and care products. More than half of patients (58%) find expenses related to lymphoma treatment as a significant financial burden; however, primarily not related to medicaments but to travel expanses to the doctor as well as days of absence from work. In contrast to the similar answers between patients and doctors regarding the aforementioned issues, only 35% of doctors note that illness-related expenses may be a heavy burden for patients.
Generally, over 80% of patients report a high impact of the disease on their physical domain (ratings 4–6 on a 1–6 scale). In 58% of patients, the disease affected their independence, with 84% rating this impact as high (ratings 4–6). Furthermore, 54% of the participants reported experiencing difficulty falling asleep or having sleepless nights. However, doctors have reported that only 16% of their patients have encountered this issue. 52% of patients had to limit their physical activity, and 64% experienced side effects of the treatment. The doctors have evaluated the rate of side effects similarly to their incidence reported by patients as according to them, 68% of patients experience them. According to 34% of patients, care treatments and dressing changes are not considered burdensome. However, 63% of patients believe that their illness has reduced their available time. On average, they spend 60 min/day on dressing changes and skin care. 34% of patients reported difficulties with dressing themselves, while 55% required assistance from another person. Interestingly, doctors underestimate the percentage of CTCL patients whose disease has reduced their independence: patients’ declarations suggest that up to 58% of patients may have problems with maintaining independence, only 33% in the doctors’ opinion.
The emotional impact of the disease has also been significant, with 78% of patients rating it as high (ratings 4–6 on a scale of 1–6). Most patients strive to maintain a normal life despite their condition: 62% of respondents stated that they do everything they can to enjoy life because they are aware of the severity of their disease. 57% of patients reported that they try to focus on something else when negative thoughts or emotions arise, while 55% stated that they try not to think about the disease. 55% expressed hope that their life will be relatively normal. Despite this, 64% of people miss their previous lifestyle and opportunities, and 46% are afraid for their life and health. While they feel they have full emotional support from their loved ones, 57% require additional professional support from a psychologist or psychotherapist. In general, doctors know their patients’ emotional side well, as in most questions the percentages of the answers have been similar.
Most CTCL patients do not acknowledge the direct impact of the disease on their interpersonal relationships, despite 62% of patients rating it as high. However, approximately 34% of patients withdraw from social life on their own initiative, 31% hide the disease due to reactions of people around, and 24% experience limitations or difficulties in their intimate life. According to the survey, 70% of doctors believe that patients with CTCL frequently experience limitations in their intimate life, compared to only 24% of patients who share this belief. Up to 46% of patients have had their disease misidentified as an infectious disease by others. Public knowledge of cutaneous lymphomas in Poland is limited, with 84% of patients acknowledging this fact. Improving public awareness of the disease would greatly benefit 78% of patients. The lack of social awareness regarding the disease has a significant impact on the well-being of 58% of patients.
High impact of the disease on the professional work has been observed in 61% of patients. In 25% of CTCL cases, the disease affected patients’ professional lives, with 15% stopping work and 10% changing their employment conditions (such as reduced working hours, changing employers, or altering their working methods). Of those affected, 61% experienced a decrease in income, with half of them experiencing a reduction of 50% or more. At the time of the study, only 43% of the studied CTCL patients have been employed. Furthermore, 48% of individuals experience a decrease in productivity or efficiency at work following an illness, while 46% express concern about job security due to their illness. 19% of patients reported experiencing negative attitudes from their colleagues or superiors at work.
When it comes to the sphere of information on the disease, 79% of patients reported receiving sufficient information at the time of diagnosis, scoring 4–6 on a scale of 1–6. However, approximately 40% of patients indicated that they lacked information on topics such as available treatment options, treatment side effects, and other patient experiences. Patients with CTCL generally feel knowledgeable about their disease, with 85% reporting a comprehensive understanding. Despite this, 75% of patients are still seeking information about cutaneous lymphomas, particularly on available treatment options (49%), side effects (33%), stories from other patients (24%), and specialists dealing with cutaneous lymphoma (22%). The most popular sources of information for patients in Poland have been doctors (87%) and the internet (70%). On the internet, patients primarily browse medical portals (68%), blogs/forums (49%), and social networking sites (49%). However, the majority of patients (93%) consider only recognized specialist doctors as reliable sources of knowledge. Patients with CTCL do not typically seek knowledge through formal or informal patient groups (none of the surveyed patients reported doing so), despite their curiosity about the stories and experiences of other patients. On the other hand, according to the survey of doctors, 65% recommend that patients seek information about their disease from patient associations. Most patients have been satisfied with the information and support provided by doctors and medical staff (nurses, physiotherapists). Ratings for support received from doctors were slightly higher than those for staff (91% satisfied vs. 79%). According to the survey, 90% of doctors report that patients with CTCL have been sometimes subject to inaccurate assessment of their condition by others (e.g. different diagnosis, infectious aetiology of the disease), while only 46% of patients with CTCL report experiencing such inaccuracies.
The topics of greatest interest to CTCL patients have remained consistent over time. The top four concerns at the time of diagnosis are the same as the top four at the time of collecting the questionnaire. Patients require information on available treatment options, treatment side effects, other patient’s medically related history, and best lymphoma specialists. The last two topics had been mentioned slightly more often at the time of diagnosis. Doctors pay relatively more attention to the problem of changes in lifestyle, diet, and the use of everyday products compared to patients. These topics are considered important to the doctors as patients often lack knowledge about them. When asked what changes could be made in Poland to improve the lives of CTCL patients, the most common patient responses were: quicker diagnosis, improved access to specialists, more affordable treatment, increased availability of specialist clinics, and the establishment of a patient association or support group.
The Skindex-29 index values indicate the average impact of CTCL on each of the three analysed spheres of life: emotions, symptoms, and functioning. The Skindex-29 values have been presented in Figure 2.
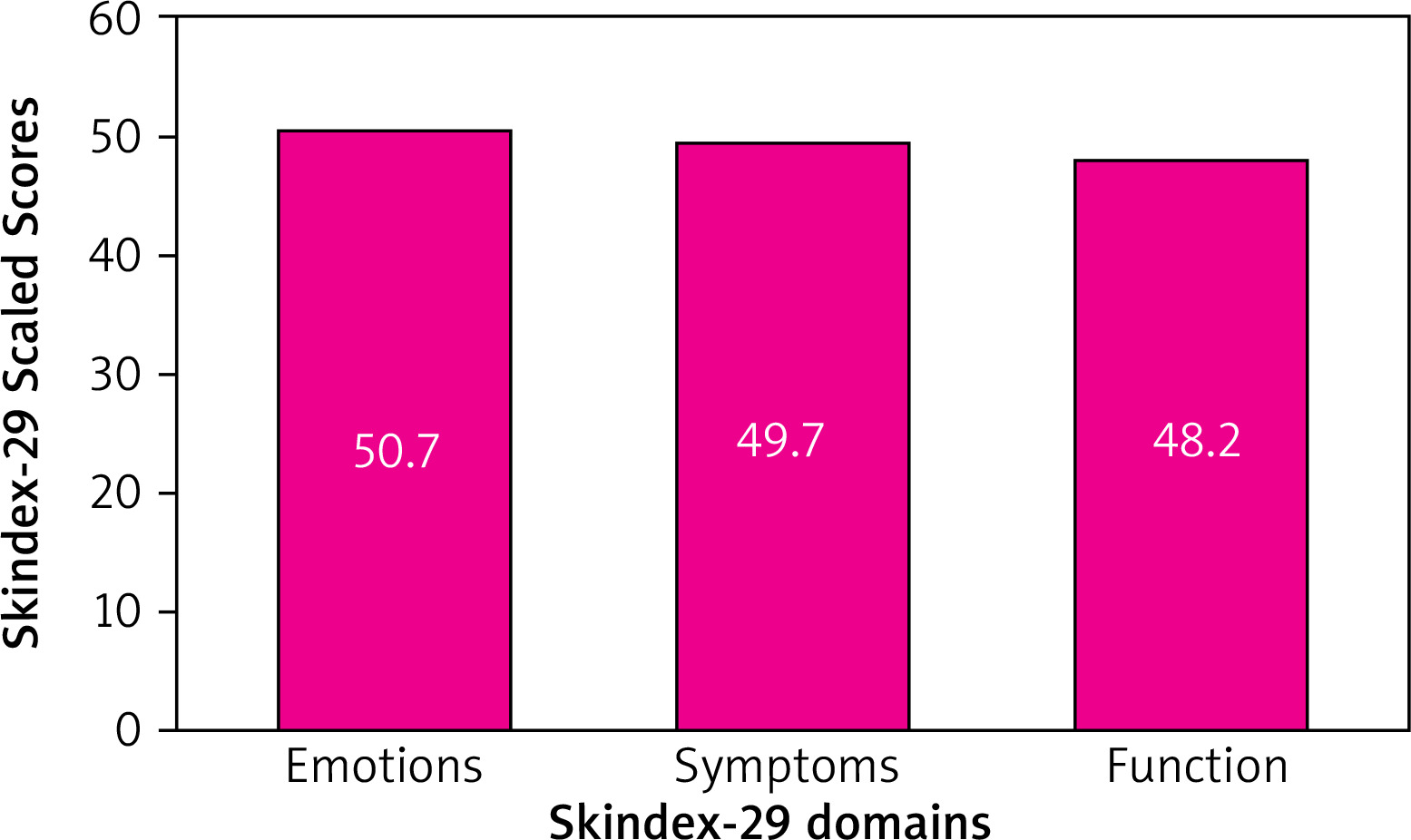
The average score for each sphere was approximately 50 out of 100. When analysing the values obtained from the Skindex-29 questionnaire, divided by patient demographics, a significant difference in the impact of the disease on the lives of patients with CTCL is visible. In our study this impact has been particularly strong in women. The disease primarily affects their emotions and experiencing of disease symptoms. Moreover, the disease has a stronger impact on individuals dissatisfied with their financial situation and non-working patients. Additionally, higher education levels correlate with a stronger emotional impact and perception of disease symptoms.
Discussion
This study presents an in-depth analysis of the QoL of Polish patients with CTCL. Our data support the significant burden of this group of diseases. Cutaneous lymphomas primarily affect the physical and emotional domains of Polish patients, with around 80% of respondents reporting a high impact in these areas. Additionally, we provide the doctor’s perspective, which is mostly consistent with the patient’s perception of their QoL. To our knowledge, the perspective of doctors on this issue has not been previously published, despite its mentions in the literature. It is important to note that Polish doctors have underestimated the impact of the disease on insomnia, sleep disturbances, and the independence of patients (Supplementary Information 1).
According to past reports, predictors of poor QoL in CTCL include advanced stage, SS subtype, and treatment with systemic steroids or interferon [3, 4, 8]. Additionally, newly diagnosed women and those with alopecia have been identified as having particularly poor QoL [4]. Another study has shown that young age of a patient and the presence of skin of colour indicate poor QoL [9]. Patients with advanced disease or involvement of the head/neck, acral or groin/genital sites also experience a significant impact on health-related QoL [10].
In our cohort, pruritus was the most common symptom. Previous studies have also reported pruritus as the most distressing physical symptom, with similar severity across all stages of the disease [11, 12]. In some cases, up to 88% of patients were affected by pruritus, while in our study, up to 80% of patients reported experiencing it [11, 12]. Furthermore, pruritus is strongly correlated with overall QoL [1, 13]. According to a study by Ottevanger et al., it may be used as an overall QoL indicator [13]. The correlation between pruritus and Modified Severity-Weighted Assessment Tool (mSWAT) scores, as well as systemic inflammation parameters, suggests a potential link between pruritus and the inflammatory milieu in MF [14].
The Skindex-29 index values indicate the average impact of CTCL on each of the three analysed spheres of life: emotions, symptoms, and functioning. The average score for each sphere was approximately 50 out of 100. Our results were obtained from a Skindex-29 questionnaire included as part of the interviews with doctors and patients in the exploratory part of this study, however, they do not reflect the results of our questionnaire. According to the interpretation of Skindex-29, our patients have been moderately impacted in the physical domain and significantly impacted in emotional and functional domains, while according to results from our questionnaire, the most affected areas are physical and emotional domain [15]. In the majority of 10 studies reporting Skindex-29, results have been lower than those of our patients, with the exception of two studies [1, 4, 16, 17]. Considering all the aspects analysed in the Skindex-29 index, it is evident that skin sensitivity and itching, which are symptoms not specific to CTCL and are common symptoms in many skin diseases, have the greatest impact on QoL in CTCL. Additionally, patients expressed concern about the potential worsening of their dermatological condition, which has also been described in the literature [1, 3, 4, 8]. The remaining statements received values close to the average scale of our questionnaire. This indicates that despite being the most valid instrument, Skindex-29 may not be an appropriate tool for assessing all the aspects of the QoL of patients with CTCL, as shown by surveys developed in cooperation with doctors and patients [1, 3–5].
Women with CTCL diagnosis have been shown to experience worse QoL, which has been noted by previous researchers [1, 4, 8]. The likely explanation is that women report more physical and emotional symptoms, among which are more intense burning, stinging, and itching, as well as increased feelings of depression, shame, embarrassment, and annoyance due to their diagnosis [4].
The financial burden has been previously shown to impact CTCL patient’s life significantly [4, 18]. In our study, to the majority of patients CTCL is a significant financial burden, however, primarily travel expenses and not the cost of medication contrary to the literature. The likely reason for this difference is that, unlike in the United States, the majority of medications in Poland are funded by the state. Additionally, in our study we have shown that higher education levels correlate with a stronger emotional impact and perception of disease symptoms. In previous studies the patient’s education has not been correlated with the CTCL stage nor severity of the disease [19, 20].
A common issue highlighted in the literature, and also noted by 70% of our patients, is the delayed diagnosis of CTCL [1, 5, 21, 22]. Many patients have thought that earlier diagnosis could have potentially limited the spread of the disease [1, 21, 22]. Regardless of the timing of the diagnosis, patients may experience a range of emotions upon receiving a CTCL diagnosis, including indifference, sadness, or fear [1, 5, 10, 13, 17, 21–24]. Studies have shown that fear is a common response, often accompanied by shock and disbelief [1, 13, 21–23]. Also in our cohort fear has been felt by 74% of patients. However, some patients may feel relief upon receiving a final diagnosis, as noted in several studies, primarily due to the fact that it was not a diagnosis with a worse prognosis [21, 22].
Sleep infringement is another significant symptom that decreases the QoL of CTCL patients [5, 8, 13, 21, 22, 25, 26]. This ranges from difficulties in falling asleep to problems in staying asleep primarily due to itch and worrying about the disease [5]. In our study, more than half of the patients reported this problem, while the percentage of patients who have had problems with sleep in the literature ranges from 25% up to 66% [5, 8, 13, 21, 22, 25, 26]. Although this issue is included in the Skindex-29 questionnaire, it has been omitted in the MF/SS-CTCL instrument [27]. To improve the quality of sleep for CTCL patients, it is important to effectively control and reduce itching [13, 21].
Consistent with previous research, we have identified the need to collaborate with psychologists, psychotherapists, and sexologists, if necessary [1, 3, 13, 21, 28]. In our population, 57% of patients reported the need for psychological or psychotherapeutic support. If significant symptoms are present which may affect daily activities or relationships, a referral should be considered to reduce the burden of the disease [1]. Although this has not been investigated in CTCL patients, supportive care programs have been shown to be effective in other cancer patients and may enhance their QoL [1].
Novel perspectives and concepts have been identified in our study. The literature rarely reports a reduction in available time, despite 63% of patients in our cohort experiencing it [5, 21]. Our findings are consistent with the study performed by Bhat et al., who noted difficulties in travelling for doctor appointments or treatments such as narrow-band UVB therapy primarily due to a significant consumption of time [5]. Other aspects, which have not been previously studied, are the loss of independence, trouble with independent mobility and trouble with dressing themselves. Furthermore, previous studies lacked the perspective of patients on their lifestyle and general attitude towards life. We have shown that 57% of patients try to distract themselves from thinking about the diagnosis, 55% have hope that life will be normal and 64% of patients miss previous lifestyle and/or opportunities. All of these symptoms may reflect a lack of energy and/or fatigue, which often accompanies the everyday life of CTCL patients [1, 5, 8, 18, 21, 22, 29]. This phenomenon has serious repercussions on patients’ work life as many studies have highlighted the decrease in productivity that prevents them from accomplishing everyday tasks [1, 3, 5, 8, 18, 21, 22]. In our study, nearly 50% of patients experienced decrease in productivity. It is noteworthy that while other researchers have overlooked concerns about job security and negative attitudes at work, our patients have reported these issues in 46% and 19% of cases, respectively [22].
Previous studies have identified a lack of social awareness leading to withdrawal from social life [5, 13, 18, 21, 22]. In our cohort, this was observed in 84% of patients. Importantly, over 70% of our respondents acknowledged that improving this area would enhance their QoL. Unfortunately, the stigmatization of patients with skin diseases is still prevalent. According to a recent survey, 88.1% of participants found their skin disease embarrassing in their personal life, and 83% found it embarrassing in their work life [30]. To cope with the burden of CTCL, it is beneficial from the patients’ perspective to have sufficient information about the disease, actively search for it, accept the illness, and seek support from family and friends [20, 21]. In our study, 40% of patients reported lack of information about the disease, while in Abraham et al.’s study nearly all patients reported the same issue [22]. Doctors should consider a patient’s perception of their illness and coping mechanisms as studies have shown that recognizing maladaptive coping may improve adherence to treatment [20, 21].
As it has previously been shown, Skindex-29 does not analyse several skin symptoms frequently seen in CTCL patients, such as skin breaks (fissuring, sores, lacerations) or skin flaking [5]. Furthermore, Skindex-29 is highly specific to the skin symptoms and does not ask about lack of understanding in the community, the feeling of hopelessness and otherness, the available time reduction, deterioration of productivity nor the lack of independence caused by the disease. We have demonstrated that patient outcomes are impacted by a lack of community understanding. Unfortunately, the MF/CTCL specific instrument is not up to the task either [27]. Several important aspects have not been addressed in this questionnaire, including the length of time it took to receive a diagnosis, sleep issues, the need for professional help from a psychologist, psychotherapist or sexologist, concerns about job security, negative attitudes in the workplace, and a lack of information about the disease [27]. It is important to provide a comprehensive overview of all relevant aspects to ensure that patients receive the best possible care.
Conclusions
This is the first study to report an in-depth analysis of the QoL of Polish patients with CTCL and the first study to report the doctor’s perspective. The study shows that the disease affects most aspects of CTCL patients’ life. Importantly, Polish doctors have underestimated the impact of the disease on several areas of life, such as insomnia, sleep disturbances, and patient independence. The absence of research on doctors’ understanding of their patients’ makes it difficult to identify areas where changes could be made to enhance the patient-doctor relationship and collaboration. Understanding a patient’s QoL is crucial for medical professionals to provide appropriate and interdisciplinary long-lasting treatment, including addressing their emotional needs by referring them to a psychiatrist or psychologist to support them if necessary [20]. Finally, it should be noted that while Skindex-29 is a commonly used and validated tool, it may not fully capture all aspects of QoL for patients with CTCL. We have also shown that the MF/CTCL instrument is not sufficient either and there still remains a high need for a validated tool covering all important aspects of CTCL patients’ QoL.







