
Introduction
Inborn errors of immunity (IEI) are a group of over 400 diseases caused by germline variants affecting single genes [1]. Early recognition of IEI is crucial before patients experience severe infections or deterioration in quality of life [2]. Lack of knowledge and awareness leads to delays in diagnosis [2]. Although IEI is categorized as a rare disease, it is believed to be more common than previously thought [3]. To raise awareness, the Jeffrey Modell Foundation (JMF) developed the “10 warning signs” for both children and adults [3]. Additionally, since 1999, the European Society for Immunodeficiencies (ESID) has developed a long-term project for the diagnosis, classification, and management of IEI [4].
Although IEI is considered rare, its incidence varies by region [5]. The frequency is thought to be higher in countries like Turkey, where consanguineous marriages are common [5]. For example, the prevalence of IEI is 0.97 per 100,000 in Sri Lanka and approximately 6 per 10,000 in the United States [6, 7]. In a study conducted by Kılıc et al., the prevalence in Turkey was reported as 30.5 per 100,000 [8]. Previous studies have shown that awareness of IEI is low among physicians [5, 9, 10].
Aim
In this study, we hypothesized that the awareness and diagnostic confidence regarding IEI among pediatricians and pediatric residents in Turkey would be suboptimal, thereby highlighting the need for additional education and systemic support.
Material and methods
Between August and October 2024, surveys were sent via email and phone to pediatricians and pediatric residents working in various regions of Turkey. Those who agreed to participate were included in the study.
In the first part of the survey, participants were asked about their age range, gender, institution, and professional experience. Age ranges were defined as 25–30, 31–40, 41–50, and > 50 years. The second part focused on participants’ awareness of IEI and knowledge of the 10 warning signs. Questions also covered laboratory tests used in the diagnosis and treatment approaches of IEI.
Participants were asked multiple choice questions and were instructed to select one or more laboratory tests they considered appropriate from the questionnaire.
Statistical analysis
Descriptive data were expressed as percentages. Numerical variables were presented as mean and standard deviation if normally distributed, or as median and interquartile range otherwise. The χ2 test was used to compare frequencies between groups. A p-value < 0.05 was considered statistically significant. Data analysis was conducted using SPSS version 22.0.
Results
A total of 164 participants, the majority of whom were female (54.9%), took part in the study. Most participants were aged 31–40 years (45.1%) and the majority were pediatric specialists (70.8%). Table 1 summarizes participants’ demographic characteristics, including age, experience, gender, and workplace. Most participants reported that they did not follow IEI cases (57.3%) and had not diagnosed any immunodeficiency (69.5%). About half of the participants stated that they had difficulty managing immunodeficiency cases. Three-quarters of them indicated the need for postgraduate training on IEI diagnosis, management, and treatment. When asked to rate their competence in recognizing immunodeficiency on a 0–10 visual analog scale, the median score was 4, indicating low self-confidence.
Table 1
Characteristics of the participants
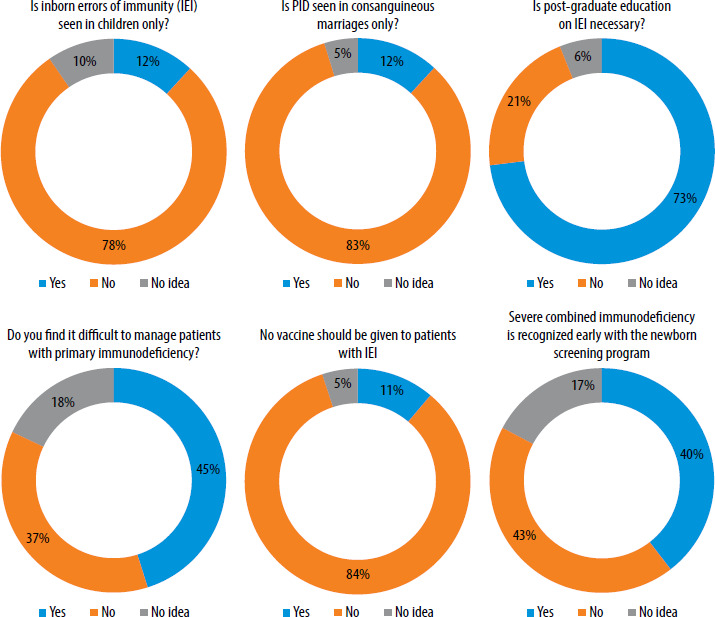
Most participants (78%) were aware that IEI is not limited to childhood and 83% recognized that it is not only caused by consanguinity. Additionally, 82.9% believed that pediatricians in general are insufficiently informed about IEI. Regarding newborn screening, nearly half of the participants (47.6%) emphasized the importance of including IEI (Figure 1).
Figure 1
General information about inborn errors of immunity IEI – inborn errors of immunity, SCID – severe combined immunodeficiency
Among the pediatric warning signs, the most frequently recognized were recurrent otitis media (87.7%), persistent candidiasis (86.4%), and recurrent skin abscesses (82.7%). The least recognized signs were ≥ 2 months of antibiotic use (59.3%) and intravenous antibiotic treatment for infections (60.5%).
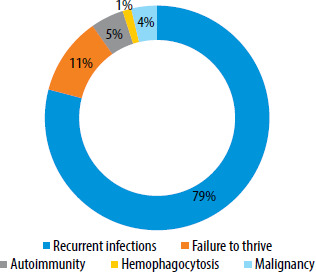
In adults, the most common indicators of IEI were opportunistic infections (83.3%), unexplained skin lesions or wounds (79.5%), and chronic fungal infections (77.9%). Less commonly linked signs included a single episode of pneumonia per year and hyperplasia of secondary lymphoid organs. The participants were also questioned about the most common clinical presentations of IEI (Figure 2).
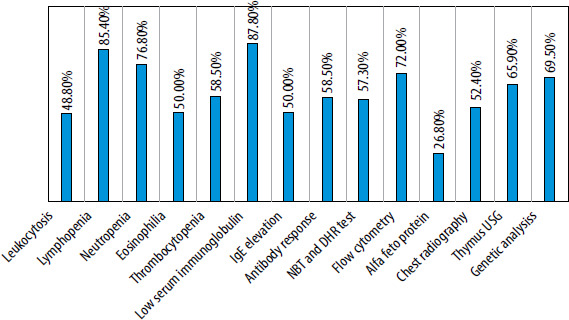
The most frequently cited diagnostic laboratory findings were low serum immunoglobulin levels (87.8%), lymphopenia (85.4%), neutropenia (76.8%), and flow cytometry for T and B cell counts (72%). The least helpful ones were alpha-fetoprotein levels (26.8%), leukocytosis (48.8%), and eosinophilia (50%) (Figure 3). The most well-known treatment was hematopoietic stem cell transplantation (85.2%), followed by antimicrobial prophylaxis (84%) and immunoglobulin replacement therapy (81.5%). Enzyme replacement and gene therapy were the least recognized treatment options.
No significant difference was found when professional experience and participants’ self-sufficiency were evaluated (p = 0.95), and no difference was found when the institution and competence were evaluated (p = 0.87).
Discussion
This study aimed to assess the awareness of pediatricians and residents in Turkey. Given that IEI primarily affects children and can cause morbidity and mortality if undiagnosed, this research is highly relevant.
The majority of SCID (severe combined immunodeficiency) cases are sporadic and lack a family history that would allow early detection [11]. Most participants in this study acknowledged that IEI is not exclusive to consanguinity and that it should be included in newborn screening programs.
In a study from Turkey, 29.7% of pediatricians reported feeling anxious when treating IEI patients [5]. Similarly, in our study, half of the participants expressed difficulty in managing PID/primary immunodeficiency cases. Four out of five respondents stated that pediatricians in Turkey are not sufficiently knowledgeable about IEI, and 75% highlighted the need for postgraduate education. Professional organizations that support immunology education hold significant responsibility in addressing this gap. In a Peruvian study involving pediatricians and residents, 39.8% of participants were familiar with the JMF’s 10 warning signs. The most commonly known signs were related to infections. In our study, 59.3% of participants claimed to know the 10 warning signs, with the most frequently cited being the same as in the Peruvian study. The observed differences in awareness levels between our study and the Peruvian study may be partially explained by contextual factors such as differences in pediatric training curricula, national public health priorities, accessibility of clinical immunology services, and the relative visibility or prevalence of IEI within each country’s healthcare system.
In another study by Veramendi-Espinoza et al., half of the participants had worked in an immunology unit [12]. In contrast, a study in Brazil reported that 72.2% of pediatricians had received IEI-related education during residency, and 75.9% had received it post-residency [13]. In our study, 24.4% of participants stated they had not worked in an immunology unit during their training.
Participants identified low immunoglobulin levels, lymphopenia, and flow cytometry as the most useful diagnostic tools. A previous study in Turkey reported similar findings, highlighting immunoglobulin levels and antibody responses as essential [5]. Thrombocytopenia, a symptom of Wiskott-Aldrich syndrome, was recognized as important by more than half of our participants. The least known lab marker was alpha-fetoprotein.
A significant proportion of participants disagreed with the statement that no vaccines should be administered to patients with IEI, indicating an awareness that vaccination decisions should be individualized. This perspective aligns with current international guidelines, which emphasize that immunization in IEI patients should be based on the specific nature and severity of the immune defect. While live attenuated vaccines (e.g., BCG, MMR, OPV, varicella) are contraindicated in patients with severe combined immunodeficiency (SCID) and certain other combined defects due to the risk of vaccine-associated disease, inactivated vaccines are generally considered safe and beneficial for many other IEI subtypes [11, 14]. Studies have shown that, when appropriately selected, vaccines can provide critical protection against preventable infections in immunocompromised patients [2, 3]. The individualized approach to vaccination is therefore essential and should be guided by comprehensive immunological evaluation, as recommended by expert consensus and societies such as the IUIS and ESID [1, 2]. Despite the development of clinical immunology in Turkey, access to pediatric immunology and allergy specialists remains uneven across regions, with some areas lacking specialists entirely. Moreover, the absence of adequate laboratory infrastructure for immunological testing in certain hospitals limits the diagnostic capacity of physicians, particularly in underserved regions.
This study’s strength lies in its coverage across all regions of Turkey. Its main limitation is the small number of participants. Repeating the survey with a larger sample could provide further guidance. In addition, a pilot study was not conducted before the questionnaire was applied to the participants.
Our study revealed that most pediatricians and residents feel inadequate in diagnosing and managing IEI and expressed a need for further training. Enhancing education can improve awareness and management, enabling early diagnosis and preventing complications.










