
Introduction
Hidradenitis suppurativa (HS) is a chronic, inflammatory, recurrent and debilitation dermatosis of the pilosebaceous unit [1]. It principally affects integrous body areas, such as axillary, inguinal, gluteal, and perianal regions. This condition presents with inflammatory nodules, abscesses and tunnels, oozing and scarring are common phenomena in the course of the disease. Pain and itch are the subjective symptoms which accompany the HS lesions [2]. The age of onset is usually after puberty and before 40 years of age. The prevalence of HS is about 1% in Europe. HS is more common in females, with a female-to-male ratio of 4 : 1 [3]. There have been long-lasting discussions about the aetiology of this disease, although recently an autoimmune background of HS has been pointed out. Moreover, recent studies have shown that pro-inflammatory cytokines play a central role in the pathogenesis of this disease [4].
HS is associated with a variety of comorbidities, such as obesity, metabolic syndrome, cardiovascular diseases, inflammatory bowel disease, e.g. Crohn’s disease and spondyloarthropathy [2]. It has a very negative impact on the functioning and quality of life of patients [5]. Additionally to limited motion and skin flexibility, lesions localized especially in the anogenital region cause an emotional and physical burden, which can lead to many limitations in everyday life, including sexual functioning [6].
Previous studies indicated that depression might be a common comorbidity among HS patients [7]. Moreover, HS was suggested to be associated with an increased risk of anxiety and suicidality [8]. However, studies on the incidence of psychiatric comorbidities in HS patients of different nationalities and of various geographical regions are still limited.
Aim
Therefore, we conducted the current study to evaluate the incidence and severity of depressive and anxiety symptoms among Polish patients suffering from HS.
Material and methods
Study design and participants
This cross-sectional study recruited 114 consecutive HS patients from two different regions of Poland: south-west and south-east Poland. There were 61 (53.5%) females and 53 (46.5%) males with mean age 36.6 ±13.1 years. The data were collected anonymously between September 2020 and September 2021. The study was approved by the Ethics Committee of the Wroclaw Medical University (KB-750/2021).
All subjects were asked to complete a questionnaire with basic demographic data, such as sex, age, education, personal relationships, and employment. The clinical parameters concerning HS, such as duration of the disease and previous treatments were also collected. Moreover, the clinical severity of HS was assessed with Hurley staging and International Hidradenitis Suppurativa Score System (IHS4). According to Hurley staging, the vast majority of patients – 75 (65.8%) subjects presented with Hurley II stage, 25 (21.9%) patients were diagnosed with Hurley I stage and the remaining 14 (12.3%) patients with Hurley III stage. The mean IHS4 severity scoring was 14.6 ±17.0 points. Based on IHS4 scoring, 26 (22.8%) patients suffered from mild HS, 42 (36.8%) from moderate and 46 (40.4%) from severe disease. The characteristics of the studied group were presented in Table 1.
Table 1
Patients’ characteristics
Assessments
All recruited patients filled out validated Polish language versions of the questionnaires. Depression was assessed with Patient Health Questionnaire-9 (PHQ-9) [9]. PHQ-9 is a 9-item scale, which includes questions about feeling sad, depressed, or hopeless, sleep disturbance, lack of energy, appetite changes, problems with focusing on certain tasks as well as thoughts about hurting oneself or death. In each question, based on four-point Likert scale, the patient scores 0 to 3 points (0 points – not at all, 1 point – several days, 2 points – more than half days, 3 points – nearly every day). PHQ-9 total score for nine items ranges between 0 and 27 points. Scores of 5, 10, 15, and 20 represent cut-off points for mild, moderate, moderately severe and severe depression, respectively [9].
The Generalized Anxiety Disorder-7 (GAD-7) was employed to assess the anxiety symptoms [10]. GAD-7 is a 7-item scale assessing both the level of anxiety and the risk of generalized anxiety disorder. The questions included in the survey enable the respondents to evaluate the sense of anxiety, tension, nervousness, the ability to control these feelings, the ease with which they appear, and problems with relaxing. In each question, based on four-point Likert scale, one can get from 0 to 3 points depending on the frequency of the phenomenon (0 points – not at all; 1 point – a few days; 2 points – more than half the days; 3 points – almost every day). The recall period of this instrument is 14 days [10]. Scores of 5, 10, and 15 points represent cut-off values for mild, moderate and severe anxiety, respectively [10].
Statistical analysis
Statistical analysis of the obtained results was performed with the use of the IBM SPSS Statistics v. 26 (SPSS INC., Chicago, IL, USA) software. The minimum, maximum, mean and standard deviation were calculated. Quantitative variables were evaluated using the Mann-Whitney U test and Spearman’s and Pearson’s correlations. For qualitative data, the χ2 test was used. For differences in more than two groups, the Kruskal-Wallis one-way analysis of variance on ranks was used. All analyses were performed as two-sided tests with a significance level of 5%.
Results
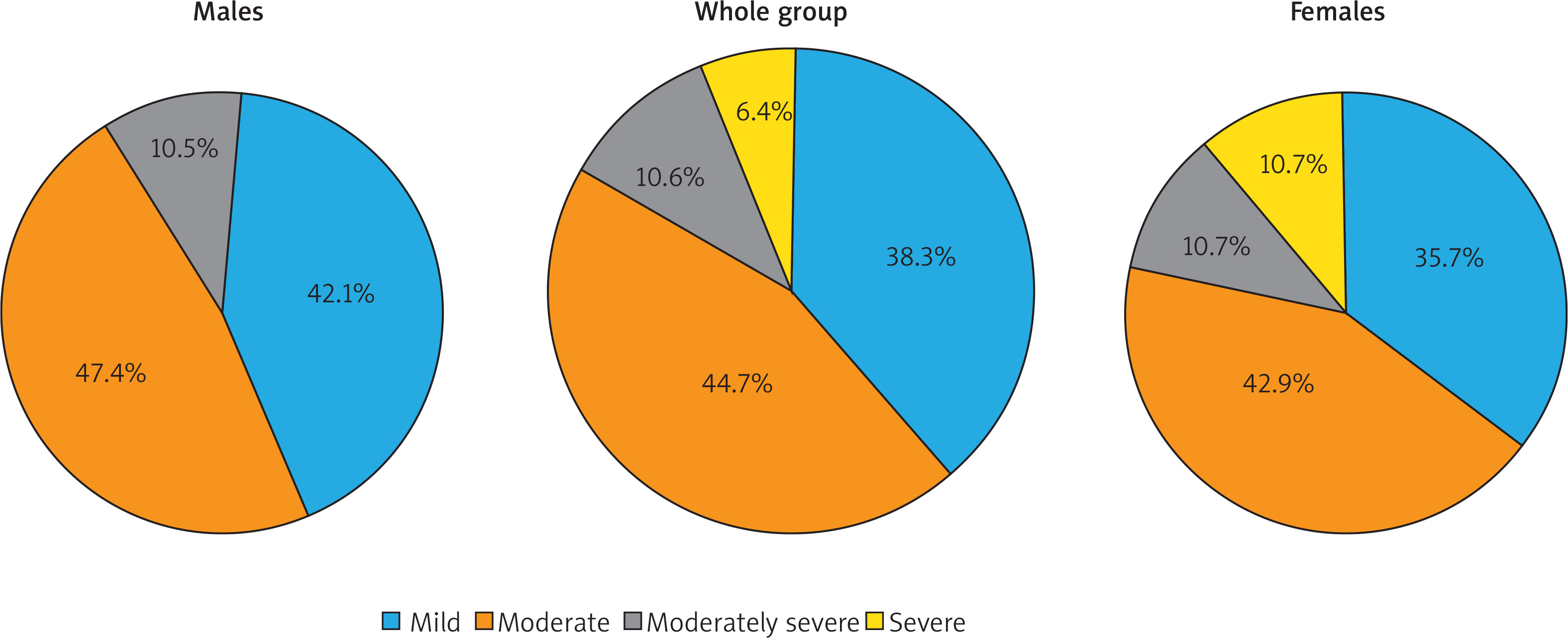
Symptoms suggesting depression were found in 47 (41.2%) patients. There was no significant difference in the incidence of depression between female and male patients – 28 (45.9%) and 19 (35.8%), respectively. Among HS patients presenting with depressive symptoms, 21 (44.7%) patients were diagnosed with moderate depression, followed by 18 (38.3%) subjects with mild depression and 5 (10.6%) patients with moderately severe depression. Only 3 (6.4%) patients presented with severe depressive symptoms. Taking into consideration cut-off points for the different depression severity levels, we were unable to find significant differences between both sexes (Figure 1). The average score of PHQ-9 was 5.6 ±5.7 points (range: 0–27 points) with no significant difference between females and males (6.4 ±6.3 points and 4.7 ±4.4 points, respectively). The incidence and severity of depression did not correlate with the disease severity, assessed with Hurley staging and IHS4. Moreover, there was not any relationship between depression and other studied parameters, such as duration of the disease, number of hospitalizations due to HS, age of patients, personal relationships, education level and employment status of patients (detailed data not shown).
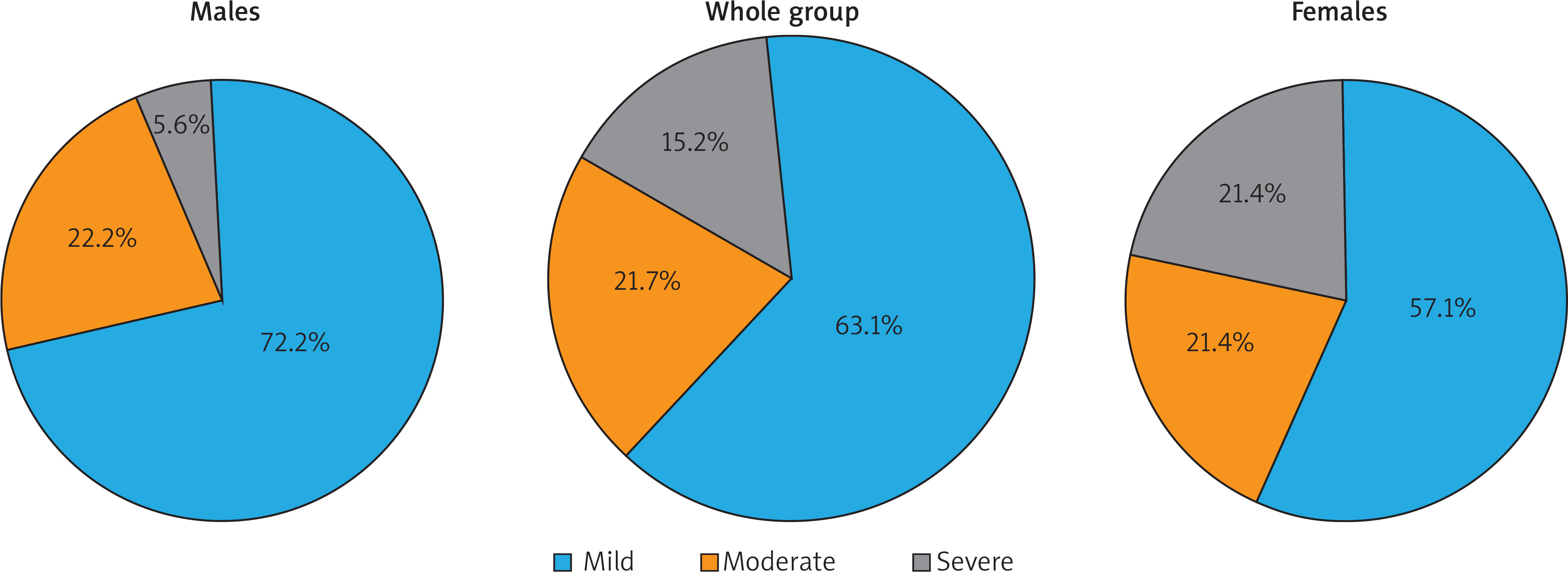
Anxiety was diagnosed in 46 (40.4%) HS patients. Although anxiety, similarly to depression, was more common among female patients (N = 28; 45.9%) than among male patients (N = 18; 34.0%), the difference between both groups did not reach statistical significance. Among all anxiety individuals, the vast majority suffered from mild anxiety – 29 (63.1%) patients. Moderate anxiety was documented in 10 (21.7%) patients and severe one in the remaining 7 (15.2%) subjects. No significant difference in the distribution of various severity levels of anxiety symptoms between females and males was noted (Figure 2). The mean GAD-7 score for the whole group was 4.5 ±5.0 points. The average GAD-7 scores were not significantly different between females and males (5.4 ±5.6 points and 3.5 ±4.0 points, respectively). The prevalence and severity of anxiety did not correlate with the disease severity, assessed with Hurley staging and IHS4. Among all studied relationships between anxiety and demographic and HS clinical data, we found only one weak, albeit significant, correlation between GAD-7 scores and duration of the disease (r = 0.197, p = 0.039).
Discussion
Psychiatric comorbidities seem to be common among patients suffering from chronic inflammatory diseases, including psoriasis, atopic dermatitis and HS [11, 12]. Our study, based on the Polish cohort of HS patients clearly confirmed these findings. Using PHQ-9 and GAD-7 instruments we demonstrated that more than 40% of adult HS subjects suffered from depression and anxiety. The study conducted by our group several years ago showed that more than 20% of HS patients obtained in Beck Depression Inventory (BDI) scores that suggested the co-occurrence of depression [13]. Our current results are in agreement with the study by Kurek et al. [7] who, although using a different instrument – Hospital Anxiety and Depression Scale (HADS), showed a similar prevalence of depression (38.6%) among HS patients. Moreover, they also found a significant correlation between depression and anxiety in this group of patients [7]. The available results on the prevalence of depression and anxiety in HS subjects depended on the instruments used by the authors. Machado et al., in their recent meta-analysis, underlined the heterogeneity of the published results [14]. They found the prevalence of depression in 26.8% of patients in the studies based on screening instruments and 11.9% when the clinical criteria-based diagnosis of depression was considered. The pooled OR for depression was 1.84. In the current study we were unable to find the significant difference between prevalence of depression among female and male patients. This is exactly the same observation as reported in the above-mentioned meta-analysis of 10 published papers [14]. Concerning the anxiety in HS the literature is very limited. Machado et al. [14] found only four such studies and calculated OR as 1.7 after multivariable adjustment for potential confounding variables. Depression and anxiety in HS are not only common phenomena in adults. A recent study showed that 29% of paediatric patients suffering from HS developed symptoms of depression or anxiety [15].
Although both depression and anxiety appeared to be common in our HS patients, there was no correlation with clinical severity of HS. This might be surprising as previously we documented the relationship between BDI scores and Hurley staging [13]. Moreover, Kurek et al. [7] also demonstrated a significant correlation between HADS scores and Sartorius scoring. On the other hand, our results may suggest that having the debilitating disease as HS is, might be sufficient to significantly influence the mental status of those patients. In the majority of analyses, psychological parameters did not depend on the disease duration [7], but we were able to note the correlation between anxiety symptoms (GAD-7 scores) and duration of HS. This can suggest that patients with long-term HS may have a raised level of anxiety.
Thanks to a worldwide utilization of PHQ-9 and GAD-7 scales, it was unchallenging to evaluate the ubiquity of depressive and anxiety symptoms among other dermatoses. A study by Lakshmy et al. [12] revealed that 78.9% of psoriasis patients developed depression and 76.7% suffered from anxiety. In contrast, Kouotou et al. [16] found only 6.1% of cases of depression and 7.7% of anxiety among 181 patients with acne vulgaris.
It is worth mentioning that both chronic inflammatory skin diseases and depression may have a common inflammatory pathway of pathogenesis. Excessive inflammation is well-known in HS with the presence of several proinflammatory cytokines expressed both in the skin and in the periphery. A shared biological mechanism of depression and anxiety in comorbidity with psoriasis, atopic dermatitis and HS have been recently suggested by some authors [17].
We are aware of the limitations of our project. We used only two self-report scales: PHQ-9 for depression and GAD-7 for anxiety assessment. The use of an additional instrument might be of value. Moreover, the screening diagnosis was not confirmed with detailed psychiatric examination. Nevertheless, short, self-assessment tools may help in identifying patients at high risk of developing mental disorders. Ultimately, our study was unable to pinpoint the exact cause of an elevated burden of major depressive disorder or anxiety in our cohort of HS patients.
Conclusions
The results of our study confirm high prevalence of mental disorders among patients suffering from HS. This should be taken into consideration in the holistic approach to these patients. It is of great importance to ascertain a comprehensive geographical distribution of depression and anxiety disorders among HS patients and to investigate further underlying mechanisms of the disease to improve mental health in the context of HS worldwide.







