
INTRODUCTION
Emollient therapy is the baseline stage of treatment for atopic dermatitis (AD) patients [1, 2]. The disease itself is associated with skin barrier abnormality, especially with lack of important lipids in stratum corneum (SC), filaggrin deficiency and lack of microbiome diversity. It is followed by loss of natural moisturizing factor (NMF), and increased transepidermal water loss (TEWL) [1, 3]. Emollient products can satisfy the endogenous deficiencies of atopic skin, while exogenous factors such as the environment, climate, or lifestyle are equally important factors influencing the symptoms of the disease [2–5]. Nowadays emollient preparations are constructed to fulfill lipid deficiencies and limit TEWL, as well as to possess hygroscopic properties and counteract microbiome dysbiosis [2–5]. The main role of the emollients is to restore skin barrier defects and make it functional again [1–3].
Due to the genetic mechanisms of inflammation in AD (such as filaggrin (FLG) mutation) stratum corneum lipids lack essential fatty acids, cholesterol and ceramides, and a ratio of those compounds is insufficient [3, 5]. The lipid metabolism in the SC is disturbed, resulting in formation of pro-inflammatory markers such as arachidonic acid and other eicosanoids. Not only genetic factors are causing those deficiencies, also environmental factors (stress, pollution, microbiota) have that influence. What is more interesting, it is suggested that the main cause might be the synergism of both genetic and environmental factors, which may contribute to the development of AD symptoms. Currently, research is underway to find the specific gene and protein that influences the impaired lipid metabolism in SC. Reports from studies on mice indicate a significant influence of PPARδ signaling, which results in shortened lipid chains. Also, the influence of the OVOL1, a protein regulating expression of filaggrin, may have an impact on its deficiency and impaired lipid metabolism [6].
Authors report that lipids in SC constitute 15% of the dry weight of SC, of which 50% are ceramides, 24% cholesterol and 20% fatty acids. In atopic dry skin, the content of fatty acids is increased and of ceramides is decreased, which translates into an increase in TEWL. Deficiency of filaggrin, a protein that strengthens and connects corneocytes, followed by lack of NMF components that hydrate SC causes the production of certain amino acids [3]. Unfortunately, this is an ineffective attempt to retain water in the epidermis and causes the previously mentioned disturbance of the lipid ratio and increased TEWL [3, 5]. The relationships described above constitute the etiology of dry, atopic skin and pruritus [3].
Another interesting phenomenon is a disturbance in the proportions of key ceramides, i.e. an increased level of ceramide AS (alpha-hydroxyacyl sphingosine – a ceramide composed of an α-hydroxy fatty acid and sphingosine) and decreased levels of ceramides EOS (esterified omega-hydroxyacyl sphingosine – containing an omega-hydroxy fatty acid esterified with linoleic acid and sphingosine), EOH (estrified omega-hydroxyacyl 6-hydroxysphingosine – similar in structure but containing 6-hydroxysphingosine), and NP (non-hydroxyacyl phytosphingosine – composed of a non-hydroxylated fatty acid and phytosphingosine). Additionally, there is a predominance of short-chain ceramides, which causes imbalance and disruption of the lipid barrier and correlates with xerosis [5, 7]. Therefore, there is a concept made by some authors that the ideal appropriate ratio in emollients that can replace lipids topically should be 3 : 1 : 1 or 1 : 1 : 1 for ceramides, fatty acids and cholesterol, respectively [3]. Regarding this theory, more and more attention is being paid to the content of important lipids in emollients.
The most important and primary function of moisturizing products is to stop water loss [1–3]. Reducing TEWL rebuilds the normal epidermal barrier by maintaining moisture in the epidermis [2, 3]. Thanks to this, the process of proper exfoliation of the epidermis is normalized and the skin becomes smooth [3, 5]. In consideration of the components of emollients, the sealing component creates a film that prevents moisture loss, the moisturizing component directly delivers moisturizing ingredients to the epidermis, as also to the dermis, and the occlusive component normalizes the exfoliation process of dead epidermis cells by filling the gaps in the epidermal barrier [1, 3, 5]. It is worth adding that if the composition of the lipid component of the preparation is similar to the lipids in the SC, it can be expected that the lipids inside keratinocytes will also be supplemented, which will contribute to achieving internal, lasting skin hydration and restoration of the skin barrier function [3, 5].
Emollients mainly consist of occlusive substances, e.g. paraffin, moisturizing substances (humectants) e.g. glycerin and urea, as well as sealing substances (lipids) e.g. triglycerides, ceramides and cholesterol [1–3]. Humectants are important components of emollients that easily penetrate the epidermis thanks to their small molecules. Glycerin and urea (particle size 200–300 Da) are the most frequently used humectants, as they effectively complement NMF. However, humectants should not be applied alone, since they may increase TEWL; thus, they must always be combined with an occlusive component. Glycerin is a forceful humectant with a present effect even when the product has been washed away from the skin, therefore, it is readily used in emollients [3]. Paraffin, functioning as an occlusive agent, forms a film over the SC and reduces TEWL most effectively when applied within 3–5 minutes after bathing. The discontinuation or removal of paraffin results in the loss of these effects, which constitutes its main drawback [1–3]. On the other hand, paraffin-based products should permit limited water vapor transmission to prevent bacterial overgrowth; therefore, they are frequently combined with humectants [3]. Triglycerides, like other lipids, play a key role in the construction of the epidermis and are readily used due to these properties, as well as their wide prevalence and cheap production, when compared with ceramides [5].
New findings in the field of emollient therapy have proposed exact combinations of ingredients e.g. glycerin with urea (in concentration less than 5%) or lipid components such as triglycerides, ceramides, and cholesterol, with promising results. Products containing these ingredients strengthen the epidermal barrier and help prevent irritation [4, 5]. In one study, the content of ceramides in emollients was analyzed, providing evidence that formulations containing ceramides reduce the severity of atopic dermatitis symptoms more effectively than emollients with other types of moisturizers. According to this proof, combinations of humectants, lipids and occlusives with ceramides reduce SCORAD and have an anti-inflammatory influence on the skin [8]. The concentration of individual ingredients in the emollient is not delivered by the manufacturer, therefore, unfortunately, it is difficult to select the appropriate one with the recommended lipid and humectant content. Only approximate estimations can be made based on the order of ingredients listed on the product label. All components included in the formulation must be listed on the packaging in accordance with the INCI (International Nomenclature of Cosmetic Ingredients) requirements.
Currently, the market offers new categories of emollients with additional anti-inflammatory and anti-pruritic properties, referred to as “emollients plus”. These products contain active agents like bacterial lysates, saponins, flavonoids and riboflavins, which additionally support the protection of the skin barrier. Lysates derived from Aquaphilus dolomiae or Vitreoscilla filiformis have been shown to improve atopic skin lesions by beneficially modulating the microbiome [1, 2]. Riboflavins used in emollients plus contain extracts from protein-free oat plantlets, which have anti-inflammatory and immunomodulatory effects [9].
The above studies and new findings in the field of emollient therapy show that certain combinations of moisturizing, sealing and occlusive ingredients such as additive emollient plus ingredients result in better control of atopic dermatitis symptoms.
OBJECTIVES
Our study aims to review emollient products available on the Polish market in terms of the content of main groups of ingredients and their combinations in compositions due to recommendations from the literature.
MATERIAL AND METHODS
We investigated emollient products from the four largest and most popular Polish online pharmacies in March 2023. The products were searched by the word “emollient” and secondly checked on the manufacturer’s website if they are intended for atopic skin. The compositions found have been collected and tested in accordance with the INCI based on the CosIng (Cosmetic Ingredients) database. The amount of the ingredient in each emollient was estimated only assuming that the ingredients are arranged in the order from the largest amount to the least amount on the product’s label. Furthermore, products intended solely for hair care namely conditioners and masks, were excluded from the analysis, as these are often labeled “emollients” by manufacturers.
RESULTS
531 emollients were included in the study. Urea was found in 13.9% (n = 74) of preparations. The combination of urea and glycerin was present in 10.9% (n = 58) of the tested preparations. Glycerin with other ingredients (including paraffin, as a frequent additive) was present in 398, which is 75% of the products. Paraffin itself was present in 24.3% (n = 129). Sealing ingredients, such as ceramides were contained in 9.4% (n = 50), triglycerides in 30.7% (n = 163) and cholesterol in 5.6% (n = 30).
The combinations among individual ingredients (in the groups of humectants, occlusive and sealing substances) were also checked. The combination of glycerin with paraffin and lipids was present in 24.3% (n = 129) with triglycerides, 7.2% (n = 38) with ceramides and 4.5% (n = 24) with cholesterol. The combination of urea with paraffin and lipids was: 3.6% (n = 19) with triglycerides; 2.1% (n = 11) with cholesterol and 1.9% (n = 10) with ceramides.
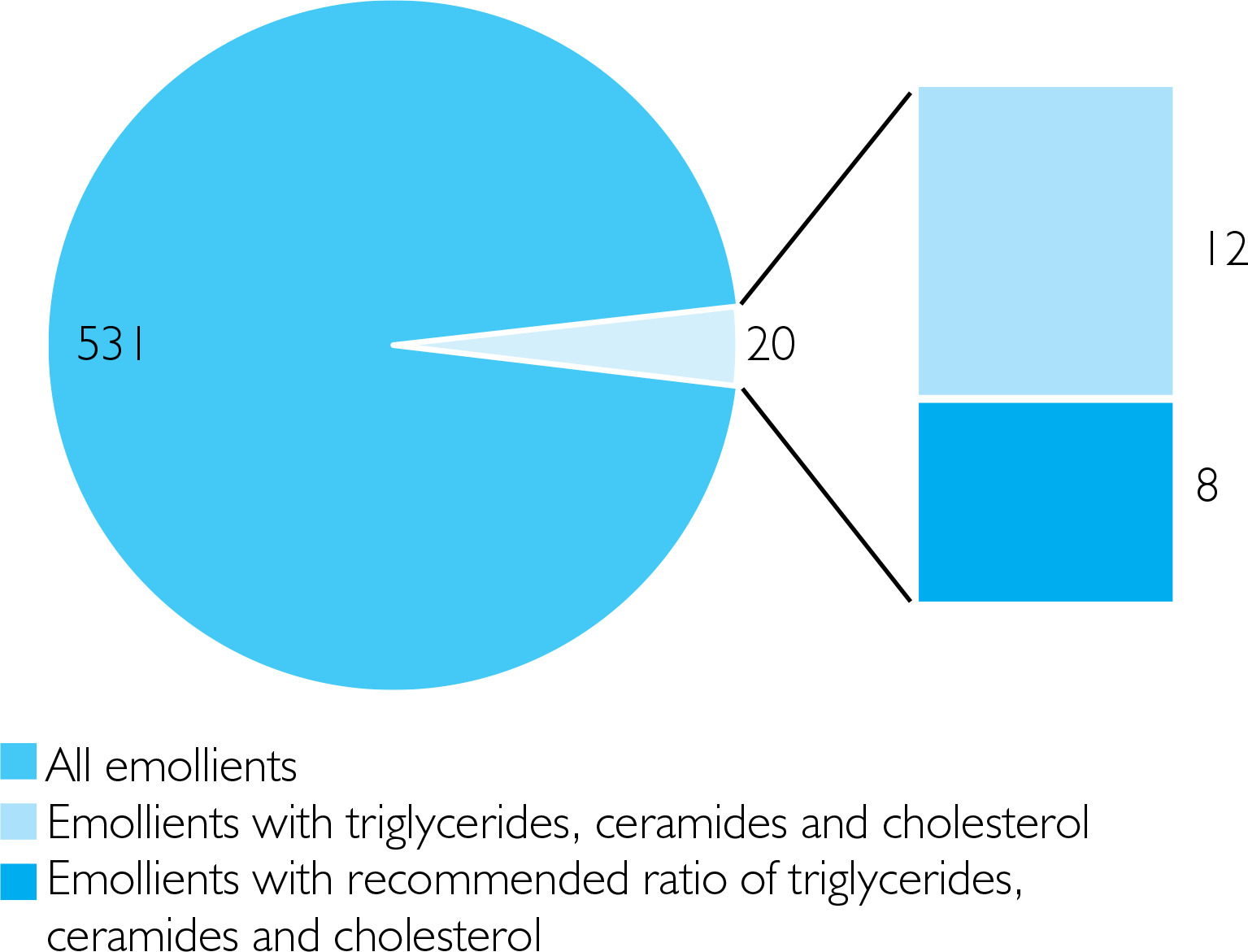
Our study also counted how many products on the Polish market contain appropriate and recommended lipid content. It was shown that among 531 products, only 20 (which is 3.8%) contain essential lipid components. The estimated amount in the composition for ceramides, triglycerides and cholesterol was consistent with the recommended one (3 : 1 : 1) only in 8 products, which is 1.5%.
531 emollient products were also checked for other substances belonging to the main ingredient groups. The most common humectants included: panthenol 23% (n = 122), propylene glycol 18.6% (n = 99), sodium hyaluronate 10.5% (n = 56) and pentylene glycol 10.5% (n = 56). Among the most common lipids were: helianthus annuus seed oil 16.4% (n = 87), prunus amygdalus dulcis oil 10.4% (n = 55) and cannabis sativa seed oil 10% (n = 53). The most common occlusive substances are: cetearyl alcohol 31.6% (n = 168), butyrospermum parkii butter 26.2% (n = 139), dimethicone 16.6% (n = 88), caprylyl glycol 16.4% (n = 87), cocoa butter 13.7% (n = 73) and squalane 12.2% (n = 65).
According to figure 1, the data indicate a market-wide quantitative predominance of emollient products containing glycerin. Triglycerides rank second, followed by paraffin in the third place. It can therefore be stated that the most common ingredients represent three major categories of well-designed emollients namely, occlusive, sealing, and moisturizing substances indicating that this principle is largely maintained among emollient products available on the Polish market. However, delving deeper into the individual combinations of the main groups of ingredients in table 1, it is shown that approximately 40% of all emollients on the market contain the recommended combinations. The remaining approximately 50% of emollients on the market contain other substances in unpredictable combinations.
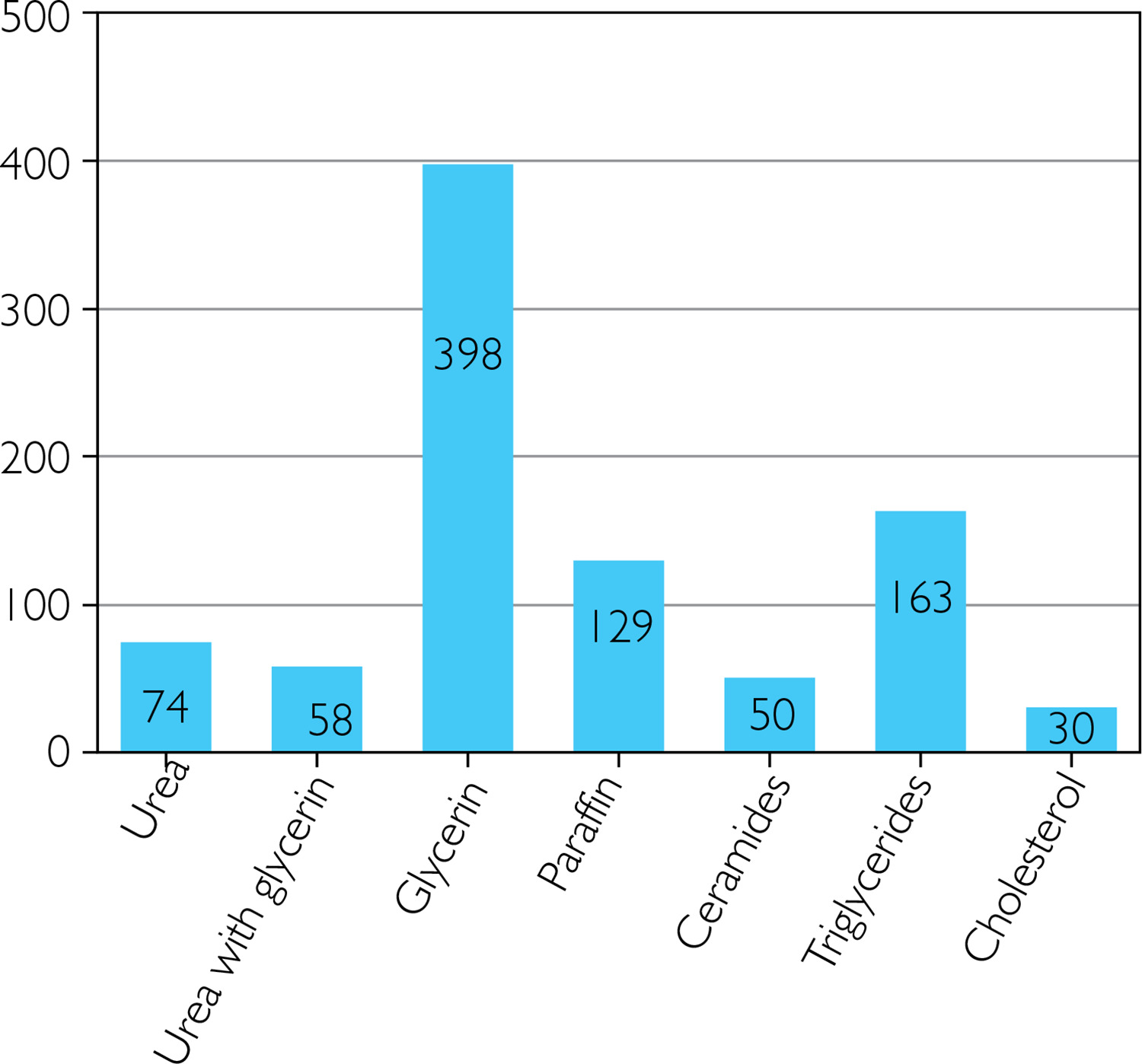
Table 1
Combinations of recommended ingredients in emollient products included in the analysis
Based on this observation, we decided to investigate which additional compounds are incorporated into these formulations and may still fulfill the criteria of a well-designed emollient. As shown in table 2, the group of humectants displays limited diversity due to the overwhelming prevalence of glycerin (present in 75% of all products shown in figure 1). Other frequently used humectants include panthenol (23.0%) and propylene glycol (18.6%), both recognized in the literature as hygroscopic agents with barrier-enhancing properties [2, 9]. Among lipids, there is greater diversity, mainly concentrated in vegetable oils and fats, e.g. sunflower seed oil, sweet almond oil and cannabis sativa seed oil. The group of occlusive substances includes cetearyl alcohol, Butyrospermum parkii (shea) butter, caprylyl glycol, dimethicone, cocoa butter, and squalane, which are frequently used as alternatives to paraffin. Despite the impression that more than a half of the market does not meet the principle of composing emollients (table 1), which is the content of a moisturizer, sealant and occlusive agent, table 2 shows that some other substances are used to fulfill these functions.
Table 2
Other ingredients identified in the analysis, divided by the main compound categories of emollients
As our study showed, among lipids, triglycerides occur in the vast majority of products, compared to ceramides and cholesterol. This shows that, unfortunately, most products will not contain the recommended ratio for lipids. However, the study did not include products containing fatty acids other than triglycerides, so in terms of ratio (3 : 1 : 1), it may actually be even less favorable. In fact, out of 531 emollients, only 20 had all three groups of recommended lipids (i.e. ceramides, triglycerides and cholesterol), and only 8 had the appropriate ratio (fig. 2). This estimation was made by the authors, as manufacturers do not disclose the concentrations or percentages of individual ingredients. In most of these formulations, triglycerides appeared among the first components in the list, whereas ceramides and cholesterol were positioned near the end, indicating that, despite their presence, the ceramide content may be insufficient to effectively restore skin lipid deficiencies.
CONCLUSIONS
Thanks to the development of biotechnology, we are now able to learn about the physiological mechanisms causing pruritus, xerosis and the inflammatory processes occurring in atopic dermatitis [1, 2, 10]. This also leads to understanding the mechanisms by which properly designed emollients can influence the management of the disease [1–3]. Therefore, the development of this branch has an impact on the emergence of new treatment guidelines, including those for atopic dermatitis, in which increasingly sophisticated emollient formulations such as “emollients plus” with additional anti-inflammatory and immunomodulatory properties are being introduced [3, 11].
Given our understanding of AD pathogenesis and the established role of filaggrin deficiency in atopic skin, the design of a synthetic filaggrin suitable for incorporation into emollient formulations represents a promising direction for the future research. Unfortunately, the filaggrin molecule is currently too large to traverse the epidermal barrier and enter keratinocytes, highlighting the need for continued research in this field [12].
Patient’s education in the field of proper emollient therapy is an important factor guaranteeing the effectiveness of AD treatment [1, 2]. Continued education is also essential for healthcare professionals involved in the management of skin diseases, as they may not always remain fully informed about newly released products. Special attention should be paid to avoiding first-generation emollients with a high content of occlusive agents, such as paraffin. According to current consensus statements, the formulation of an effective emollient should include not only occlusive, but also moisturizing and sealing ingredients. These recommendations have led to the development of more advanced cosmetic formulations tailored to patients’ needs. In light of current scientific advances, further research on emollient composition is warranted to identify the most beneficial combinations of ingredients that can best compensate for lipid deficiencies in the SC.
On the other hand, we need to remember about haptens present in emollients, such as fragrances and preservatives as the main allergenic ingredients causing contact dermatitis (CD) [1, 2, 12]. According to Kordus and Śpiewak, emollients available on the Polish market frequently contain parabens, patch-test-listed fragrances, and strong allergens according to the European Union regulations. The authors emphasize that selecting an emollient from the multitude of available preparations carries a high risk of CD [13].
The results of our study indicate the need for the further research, as many aspects remain insufficiently understood, including the proportions and relative amounts of key ingredients such as lipids. In the future, it may be advisable to include information about the percentage composition or lipid ratios on product packaging, which would facilitate the selection of the most appropriate formulations by both patients and physicians. Continued research on emollient formulations available in individual markets could contribute to the development of more comprehensive international consensus statements regarding emollient therapy. As demonstrated by our findings, despite numerous reports highlighting the beneficial effects of ceramides, cholesterol, and urea, particularly in combination with glycerin, there appears to be limited interest among Polish cosmetic manufacturers in producing formulations containing these ingredients.
The main limitation of our study is the lack of knowledge of the concentrations of individual ingredients, e.g. for urea, we are not sure whether all counted products containing urea contain it in < 5%, as mentioned in the recommendations from the literature. Moreover, some products contain several ingredients, e.g. glycerin and paraffin, so the groups are not completely separated and reading the results should take into account knowledge of the construction of emollient products. Please remember that when testing all products, we relied only on the manufacturer’s description regarding the composition and purpose of the cosmetic. The ratio for lipids was only estimated due to a lack of information about the concentration of ingredients from the manufacturer. Some of the ingredients may belong to two different groups, e.g. to occlusion or to lipids, hence our classification is based only on CosIng database.
As authors analyzing the results of the study, we see that the collaboration between physicians treating patients, emollient manufacturers and regulatory bodies is very needed to best care of patients in the field of emollient therapy. Knowledge of the proper use of emollients in daily care of atopic skin is still necessary and should be provided by healthcare workers. It is often very difficult to implement and incomprehensible to patients, therefore our task as doctors is to teach patients how to live with atopic dermatitis so that they can best reduce the symptoms of the disease and extend the time of its remission. It is worth emphasizing that the recommendations regarding emollient therapy are supported by many years of research and for years we have been trying to gain knowledge on how to fill the missing links in atopic skin.










