
Introduction
The large-scale use of direct acting agents (DAA) has been revolutionizing the management of people with hepatitis C virus (HCV) infection. Safe and highly effective regimens allowed successful treatment of a large number of patients with cirrhosis, even in the decompensated stage [1]. The eradication of HCV, known as a sustained virological response (SVR), has been associated with improvement of liver function [2] and high rates of delisting of liver transplant candidates in patients with cirrhosis living with chronic hepatitis C [3].
Despite the high effectiveness of DAA, complications of cirrhosis may not be entirely reversible. Portal hypertension might persist in a large proportion of patients after SVR [4] as well as the risk of hepatocellular carcinoma [5]. Additionally, a few studies have described the occurrence of complications of cirrhosis, such as ascites and hepatic encephalopathy after SVR. Minimal hepatic encephalopathy (MHE) is defined as the presence of cognitive dysfunction in patients with cirrhosis that cannot be clinically diagnosed and must be detected using specific tests [6]. MHE affects 25 to 48% of cirrhotic patients and is associated with daily life accidents, impaired ability to drive, development of overt hepatic encephalopathy (OHE) and death [7]. The correct identification of MHE has therapeutic and prognostic implications. The start of treatment and its reversal have been associated with lower incidence of OHE [8].
Data regarding MHE after DAA therapy in patients with cirrhosis remain scarce. The primary aim of the present study was to describe the prevalence of MHE in patients with cirrhosis due to hepatitis C before therapy and after SVR by DAA. The secondary aims were to describe reversibility and de novo development of MHE after DAA and to evaluate factors associated with this condition.
Material and methods
Study design and population
This prospective observational study on consecutive patients was conducted at the Bonsucesso Federal Hospital (Rio de Janeiro, Brazil). All individuals with chronic hepatitis C and cirrhosis attending the outpatient clinic of the Gastroenterology and Hepatology Unit from January 2016 to June 2017 were eligible. The study protocol was approved by the Bonsucesso Federal Hospital Ethical Committee (IRB number 79666417.9.0000.5253) and all participants signed an informed consent form prior to enrollment in the study.
This study included adults (age ≥ 18 years) with cirrhosis due to chronic hepatitis C, defined by a positive HCV-RNA. Cirrhosis was defined by METAVIR F4 in liver biopsy, liver stiffness measurement (LSM) ≥ 12.5 kPa in transient elastography by FibroScan (EchoSens, Paris, France), a combination of clinical aspects, presence of gastroesophageal varices and/or portal hypertensive gastropathy in gastrointestinal (GI) endoscopy or ultrasonographic imaging (morphological aspects, enlarged portal vein, splenomegaly and/or presence of collateral circulation or ascites). Patients with compensated cirrhosis were classified according to the presence of clinically significant portal hypertension (CSPH), defined as LSM ≥ 25 kPa and/or gastroesophageal varices at endoscopy. Decompensated cirrhosis was defined by a Child-Pugh score ≥ B7 and/or a MELD score ≥ 14 at baseline. In addition, patients with Child-Pugh score A or MELD < 14 with previous complications of cirrhosis (ascites, variceal bleeding) or under treatment for these complications were also considered as having decompensated cirrhosis.
Exclusion criteria were the following: 1) failure of DAA treatment (defined by a detectable HCV-RNA 12 weeks after the end of treatment [EOT]); 2) active alcohol consumption (≥ 20 g/day for women and 30 g/day for men in the last 3 months); 3) HBV or HIV coinfection; 4) hepatocellular carcinoma BCLC stage C or D; 5) previous liver transplantation; 6) pregnancy; 7) chronic persistent hepatic encephalopathy, episode of OHE or treatment for hepatic encephalopathy (with non-absorbable disaccharides or antibiotics, L-ornithine L-aspartate) before antiviral treatment and/or after SVR; 8) gastrointestinal bleeding or bacterial infections (including spontaneous bacterial peritonitis) in the last 4 weeks before baseline; 9) presence of severe comorbidities, such as significant cardio-respiratory diseases, concomitant neurological disease (known dementia, Parkinson’s disease or cerebrovascular disease); 10) current use of psychoactive drugs, such as benzodiazepines, antidepressants or antipsychotics or 11) incapacity to perform psychometric tests.
Data collection
Patients were evaluated just before starting the DAA regimen and from 6 to 18 months after EOT. The following variables were collected before treatment and after SVR: demographic characteristics (age and gender), comorbidities (diabetes mellitus and hypertension), liver disease history (HCV genotype and viral load, antiviral regimen prescribed and previous liver-related complications), closest upper GI endoscopy and LSM by transient elastography, and laboratorial parameters (biochemistry, liver and kidney tests, INR and platelet count).
Psychometric test
The Psychometric Hepatic Encephalopathy Score (PHES) was used to define presence of MHE. PHES is composed of five paper and pencil tests – the digit symbol test, number connection test-A, number connection test-B, serial dotting test, and line drawing test – that evaluate different cognitive domains commonly impaired in patients with hepatic encephalopathy, such as psychomotor speed, set shifting, concentration, attention, visual perception, visual-spatial orientation, and memory. The PHES has been extensively validated and is internationally recommended as the gold standard for the diagnosis of MHE. Normal values for each component of the PHES were derived from a control group composed of 50 individuals without liver disease (as evaluated by a history of known causes of liver disease such as hepatitis B or C, metabolic or alcoholic associated liver disease and, whenever available, aspartate aminotransferase [AST] or alanine aminotransferase [ALT] levels) paired with study group by gender, levels of scholarship (less than 9, 9-13, 13-17 and ≥ 17 years of schooling), and age (within a range of ±5 years). These individuals were evaluated by direct mouth-to-mouth contact and were not selected if they had known psychiatric illness or were regularly using psychoactive medications. Corresponding values of each PHES component in the control group as well as patients with and without MHE are shown in Supplementary Table 1. Values of each individual component of the PHES were compared to normal values and considered abnormal if 1 standard deviation outside of the mean value of the control group as recommended by international guidelines. MHE was diagnosed if 2 or more components were abnormal [9]. All tests were performed by experienced examiners in a suitable environment (a bright, quiet room).
Table 1
Baseline characteristics of patients included in the study (n = 104)
Statistical analysis
Categorical variables were described as frequency and percentage and continuous variables as mean and standard deviation or median and interquartile range (IQR). For group comparison, the chi-square (χ2) test and Student’s t-test or the Mann-Whitney test were used for categorical and continuous variables, respectively. Time-dependent analysis (Cox regression models) was performed to identify factors from baseline and EOT which were associated with MHE. Variables were entered into the multivariate Cox analysis using the backward stepwise selection method. A receiver operator characteristic (ROC) curve was plotted and the optimal threshold of quantitative variables selected in multivariate analysis for prediction of MHE was identified using the point nearest to the upper left corner of the ROC curve. Significance was determined when the p value < 0.05 using two-tailed tests. Statistical analyses were performed using the program IBM SPSS 21 for Windows.
Results
The PHES for MHE diagnosis was determined in 122 HCV-infected patients with cirrhosis before DAA treatment. Median time between MHE assessment and beginning of treatment was 23 days, and that between EOT and reassessment of MHE was 12 months. A total of two individuals were excluded due to treatment failure (non-SVR) and three due to development of OHE [during (n = 2) or after (n = 1) HCV treatment]. Additionally, 13 patients were lost to follow-up and did not perform the PHES after SVR. Therefore, a total of 104 patients [65% female with mean ±standard-deviation (SD) age of 60 ±10; 89% with HCV genotype 1; ALT levels (mean ±SD) 98 ±59; 82% Child-Pugh A and mean MELD of 10 ±4] were included. The mean (±SD) LSM was 22.3 (±14.7) kPa and 22% had LSM ≥ 25 kPa at baseline. Table 1 summarizes clinical, demographic and laboratorial characteristics of patients. Most patients (n = 80; 77%) were treated with sofosbuvir/daclatasvir, 18 of them in combination with ribavirin. Comorbidities were common, with 64 patients with diagnosis of hypertension and/or diabetes mellitus (both conditions in 23 patients). Thrombocytopenia (platelet count < 150 × 109/mm3) was observed in 60 patients and CSPH was diagnosed in 30 out of 71 patients with compensated cirrhosis. Overall, liver function was relatively preserved. Hypoalbuminemia (serum albumin lower than 35 g/l) and hyperbilirubinemia (bilirubin greater than 1.0 mg/dl) were present in 41 (39.4%) and 39 (37.5%) patients, respectively. MELD scores lower than 10 and higher than 14 were observed in 71 and 13 patients respectively.
Prevalence and risk factors associated with MHE before HCV treatment
Seventeen patients (16.3%) were diagnosed with MHE before HCV treatment. Individuals with MHE had a significantly higher altered number of PHES components compared to those without MHE [3 (IQR 2-3) vs. 0 (IQR 0-1), p < 0.0001]. Patients with MHE had more frequently alterations in all five components of the PHES, ranging from 17.6% in the digit symbol test to 88.2% in the line tracing test (corresponding numbers in patients without MHE were 1% and 9.2%, p = 0.013 and < 0.001 respectively).
Factors associated with MHE previous to SVR are shown in Table 2. Prevalence of MHE was similar in patients with decompensated compared to those with compensated cirrhosis (12% vs. 18%, p = 0.43). In addition, considering patients with compensated cirrhosis, the prevalence of MHE of those with CSPH was not significantly different from those without CSPH (20.0 vs. 17.1%, p = 0.75). The following factors were independently associated [hazard ratio (HR) (95% CI)] with presence of MHE before HCV treatment: age (per year), HR = 1.06 (1.02-1.11), p = 0.006, and serum albumin level (per g/l), HR = 0.26 (0.12-0.59), p = 0.001) (Table 3).
Table 2
Clinical features associated with minimal hepatic encephalopathy (MHE) previous to antiviral treatment
Clinical and laboratorial parameters before and after treatment
At the time of MHE evaluation, patients with SVR presented notable changes in liver inflammatory and functional parameters, as shown in Table 4. Overall, patients presented lower levels of aminotransferases, liver stiffness, serum bilirubin and INR, as well as increments in platelet count and serum albumin. Also, there was a decrease in mean Child-Pugh and MELD score levels.
Table 4
Changes of liver function and portal-hypertension related parameters after sustained virological response (SVR)
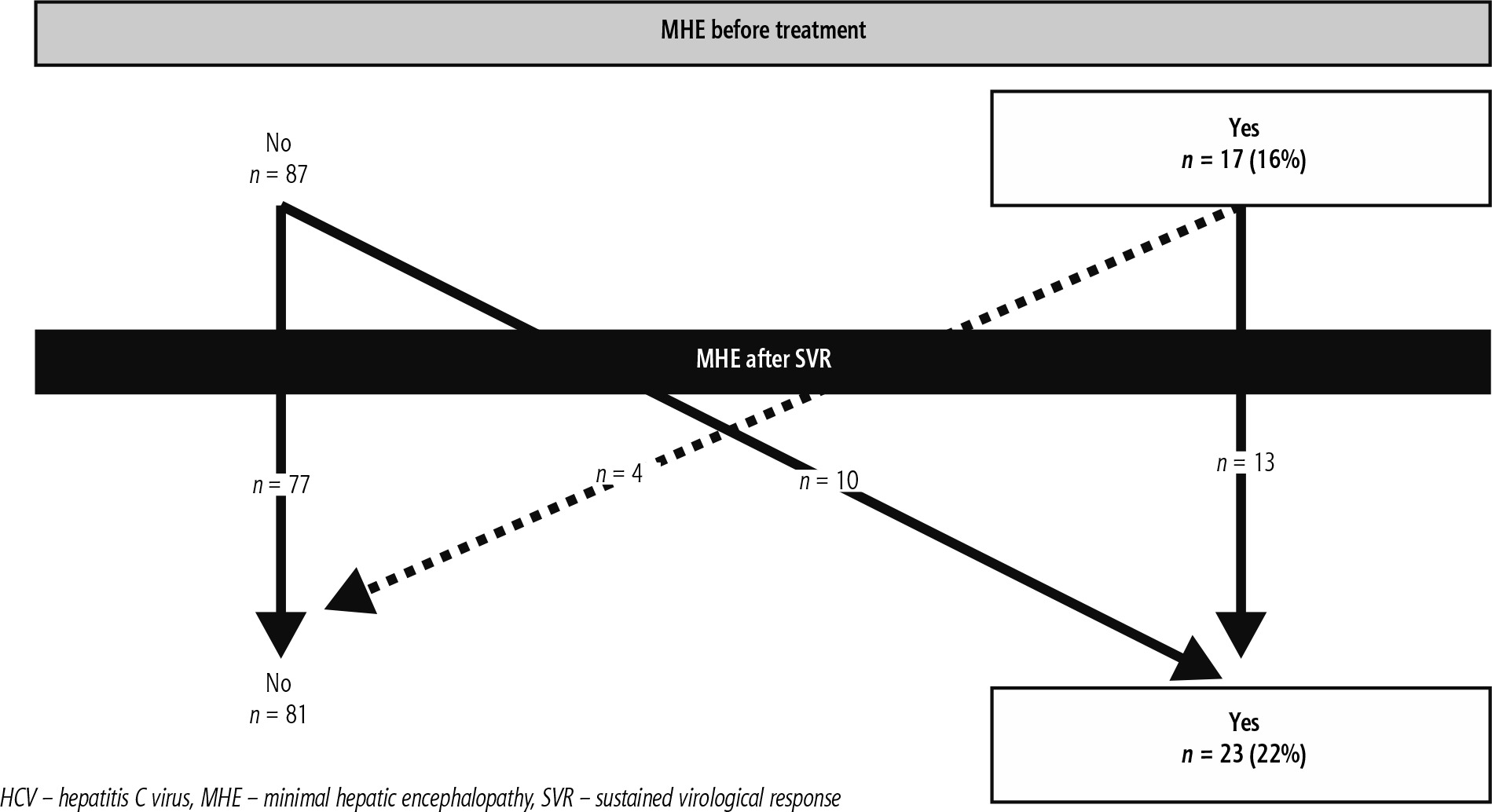
Resolution and development of MHE after SVR
Resolution of MHE after SVR was uncommon since only 4 of 17 patients with MHE before treatment did not have this condition after a sustained virological response. On the other hand, SVR did not hinder patients from developing MHE since it was observed in 10 of 87 patients (11.5%) without MHE before HCV treatment (Fig. 1). Interestingly, patients with newonset MHE after SVR had improvement in liver function parameters, as was observed for the entire population, as shown in Supplementary Table 2.
Prevalence and risk factors associated with MHE after SVR
Minimal hepatic encephalopathy was diagnosed in 23 patients (22.1%) after a median of 12 (7-15) months after EOT. The prevalence of MHE after SVR was similar to that observed before HCV treatment (p = 0.18). Median numbers of PHES components altered in patients with and without MHE after SVR were 3 (IQR 2-4) and 0 (IQR 0-0) respectively, p < 0.0001. Patients with MHE after SVR more frequently had alterations in all five components of the PHES, ranging from 21.7% in the digit symbol test to 78.3% in the line tracing test (corresponding numbers in patients without MHE were 0% and 11.1%, p < 0.001 for both comparisons). Characteristics of MHE after SVR were similar to those before treatment, as evidenced by a comparable number of PHES components affected [3 (IQR 2-3) vs. 3 (2-4)] as well as the PHES components being more frequently altered (number connection test-B and line tracing test altered in 77% and 88% of patients before treatment vs. 70% and 78% after SVR).
Patients with MHE after SVR were significantly older (69 vs. 57 years, p < 0.001); had a higher proportion of hypertension (78% vs. 46%, p = 0.008) and MHE at baseline (57% vs. 5%, p < 0.001) and had significantly lower levels of serum albumin (37 g/l vs. 40 g/l, p = 0.01) (Table 5). Neither parameters associated with portal hypertension (presence of esophageal varices and/or thrombocytopenia) nor severity of liver disease were associated with MHE after SVR. Considering all patients, age [HR = 1.13 (95% CI: 1.05-1.22), p = 0.001], presence of hypertension [HR = 7.81 (1.31-47.6), p = 0.024], presence of MHE before HCV treatment [HR = 30.3 (4.9-200.0), p < 0.001] and serum albumin levels [HR = 0.23 (0.07-0.78), p = 0.019] were independently associated with MHE after SVR. Similar factors were significantly associated with MHE after SVR in a model excluding those patients who had MHE before HCV treatment (Table 6). Best cut-off points of age and serum albumin after SVR for prediction of MHE were 65 years and 30 g/l respectively. The accuracy of the model combining these 3 parameters as categorical variables (age, hypertension and albumin) is shown in Figure 2. Presence of any of these 2 variables was associated with accuracy greater than 80% and both sensitivity and specificity higher than 75% for diagnosis of MHE. Frequency of MHE according to the presence of any of these parameters is shown in Figure 3. In the absence of all these variables, none of the patients had MHE. By contrast, in the presence of any 2 of these factors, frequency of MHE was 42% (11/26 patients), reaching up to 70% in patients with all 3 factors.
Fig. 2
ROC curves for albumin and age at sustained virological response (SVR) as predictors of minimal hepatic encephalopathy (MHE) after SVR
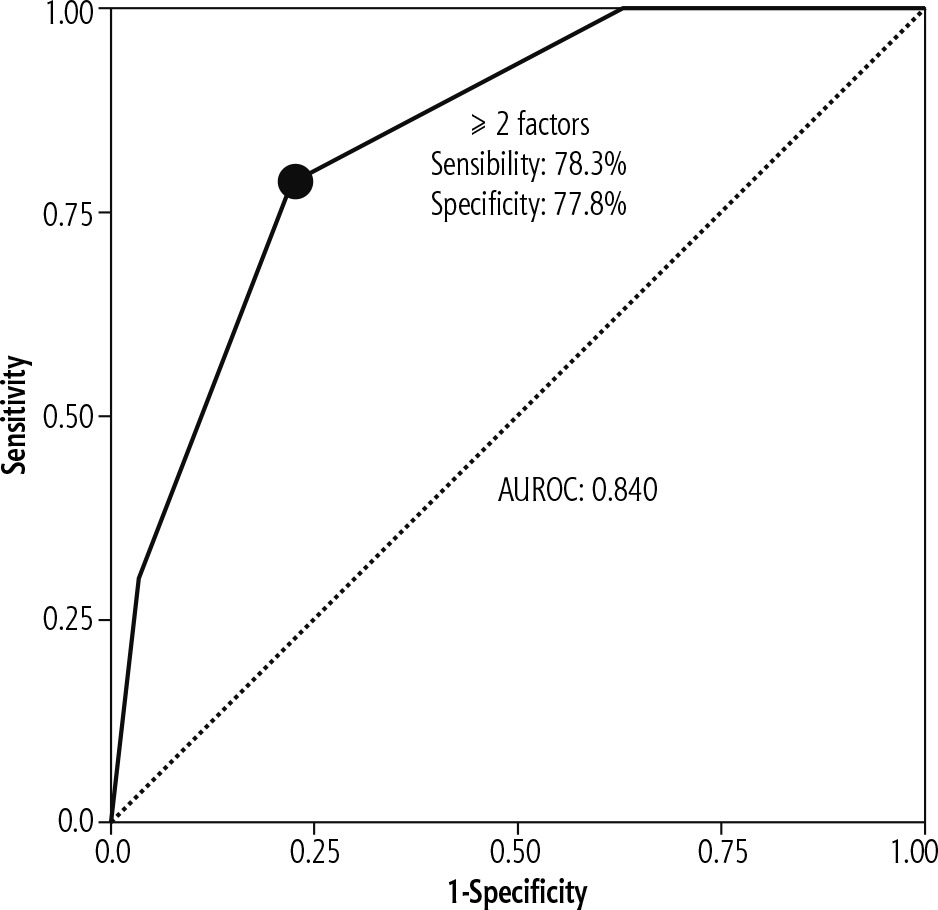
Fig. 3
Probability of minimal hepatic encephalopathy (MHE) after sustained virological response (SVR) according to hypertension, age and albumin
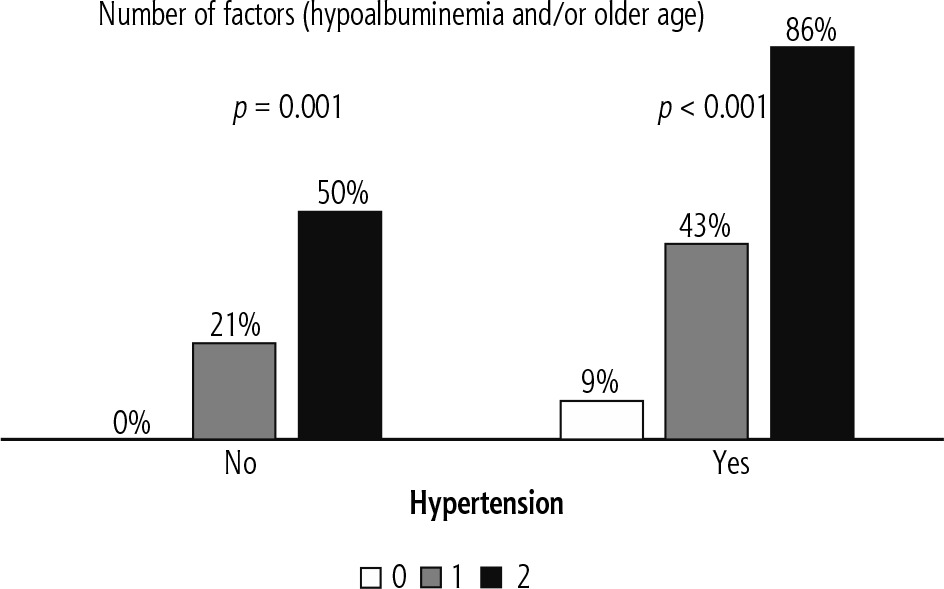
Table 5
Factors associated with minimal hepatic encephalopathy (MHE) after sustained virological response (SVR)
Table 6
Multivariate analysis of predictive factors of minimal hepatic encephalopathy (MHE) after sustained virological response (SVR)
Discussion
The main finding of this prospective study is that MHE in patients with cirrhosis due to hepatitis C is not affected by viral eradication after DAA therapy. Prevalence of MHE remains similar after SVR compared to before HCV treatment. Resolution of MHE after HCV eradication was uncommon and up to a half of patients who developed MHE after SVR did not have this condition before HCV treatment. Older age and lower serum albumin levels were independently associated with MHE before HCV treatment and after SVR. Additionally, history of MHE before HCV treatment and presence of hypertension were associated with MHE after SVR. The lack of a beneficial effect of SVR on MHE occurred despite a clear improvement in parameters related to liver fibrosis, portal hypertension and liver function.
To the best of our knowledge, this is the largest cohort of cirrhotic patients in whom MHE was assessed before HCV treatment and after SVR. Most studies have either included patients without cirrhosis or evaluated neuropsychological function with tests other than the PHES [10, 11]. A single pilot-study from Hernández-Conde et al. assessed MHE before DAA and after SVR using the PHES. However, these authors included a smaller number of patients (n = 64), who were evaluated after a shorter follow-up after SVR (median time of 6 months) compared to our study [12]. Additionally, patients with previous OHE were included and critical flicker frequency (CFF) was also considered as a diagnostic criterion (22). Despite the fact that CFF is a validated diagnostic tool for MHE, the specificity of this method varies from 66% to 92% [13]. These findings may explain some differences between both studies, such as lower reversibility of MHE and higher prevalence of MHE after SVR in the present study. Nevertheless, presence of MHE before treatment was a strong predictor of MHE after SVR in both studies.
Some data suggest that SVR may be associated with improved outcomes in terms of OHE, with lower incidence and higher rate of resolution at follow-up [14]. Nevertheless, some points deserve caution. Patients with cirrhosis still persisted with a significant risk of development of OHE (1%/year), a value very similar to our incidence at 12 months (0.95%). Also, an increased rate of resolution was not observed in patients with MELD > 10 (which comprises a substantial proportion of our study group), and one may speculate whether these patients would also lack improvement in MHE. Finally, the authors did not perform any specific evaluation of cognitive function at any timepoint. Consequently, their conclusions may not apply for MHE after SVR, which highlights the importance of our findings.
It has been previously reported that portal hypertension persists in a substantial proportion of cirrhotic patients after SVR [4]. In populations with relatively well-preserved liver function, like our cohort, presence of spontaneous portosystemic shunts has been associated with hyperammonemia and minimal and overt hepatic encephalopathy [15]. In the present study, we used well-established but indirect criteria for diagnosis of CSPH. Also, we did not specifically evaluate presence of spontaneous portosystemic shunts. No difference was found between MHE frequency in patients with or without CSPH. Besides that, no evaluation of CSPH after SVR was available due to the lack of standardized cut-off values of LSM and platelet count at this timepoint.
Another possible explanation for persistence of MHE after SVR is that its pathophysiology is not associated with liver function changes. It has been previously demonstrated in animal models that astrocyte swelling caused by hyperammonemia leads to increased production of reactive oxygen species, which in turns leads to astrocyte swelling in an auto-amplificatory signaling loop [16]. Oxidative stress is also a feature of hepatic encephalopathy in humans, as evidenced by post mortem analysis of cortical brain tissue [17]. Also, MHE after SVR may reflect persistent damage to central nervous system (CNS). Experimental studies have demonstrated neuronal cell death in patients with cirrhosis [18]. Patients with cirrhosis and hepatic encephalopathy (either minimal or overt) have decreased grey matter density, a marker of brain atrophy and neuronal cell loss, in comparison to patients without hepatic encephalopathy [19]. Additionally, persistent deficits in cognitive performance after liver transplantation are more frequent in patients with MHE previous to surgery [20]. Taken together, these data support the progressive nature of CNS involvement irrespective of improvement of liver function in patients with cirrhosis, which explains the high frequency of MHE after SVR.
Both before and after SVR, type and extension of neurological commitment were almost the same. Patients had multiple domains of cognition affected, mostly those related to attention shift and motor speed, which are traditionally impaired in patients with hepatic encephalopathy. The similarity in cognitive impairment before DAA and after SVR also suggests that cognitive impairment at both timepoints is really related to MHE and not to other possible causes, such as direct involvement of the CNS by hepatitis C virus, mild cognitive impairment or another form of dementia.
Minimal hepatic encephalopathy after SVR was associated with both liver-related and non-related factors. Hypoalbuminemia was strongly correlated with MHE both before DAA and after SVR. Albumin may reflect residual function and capacity of ammonia detoxication by the liver, and normal serum levels have previously been associated with better prognosis in patients with compensated cirrhosis [21]. Apart from oncotic properties, albumin has anti-inflammatory and anti-oxidant effects, which may be beneficial at the neuronal level. Beneficial effects of albumin infusion have been demonstrated in non-cirrhotic patients with neurological disease, such as stroke [22]. A possible protective effect of albumin was also indirectly demonstrated in the ANSWER study, in which patients receiving albumin infusion were less likely to develop OHE, especially those achieving a serum concentration ≥ 40 g/l [23]. The exact mechanism by which patients with hypoalbuminemia are at increased risk for MHE remains unclear.
Older age and hypertension were also associated with MHE after SVR. Aging is associated with diffuse reduction in brain volume and increase in cerebrospinal fluid filled cavities, consistent with brain atrophy [24]. These changes are associated with cognitive impairment and may translate to reduced functional brain reserve and, consequently, render these patients more susceptible to noxious effects of ammonia. Hypertension has many well-known deleterious effects on the brain, especially white matter lesions, possibly secondary to arteriosclerosis, leading to ischemia [25]. Besides exacerbating CNS damage, it may further impair cerebral perfusion, which has previously been demonstrated to be altered in patients with MHE [26]. The reasons why arterial hypertension could predispose to MHE after SVR are unclear. Nevertheless, there are some possible explanations: 1) Patients with and without arterial hypertension may have different thresholds for development of MHE. Before SVR, presence of higher levels of ammonia (as well as other potential substances metabolized by the liver and involved in pathogenesis of HE, including cytokines) may make these differences elusive and irrelevant, accounting for the absence of arterial hypertension as an associated factor for MHE. After SVR, however, ammonia and cytokine levels may decrease to the point that only patients with structural brain damage as a predisposing condition (like those with arterial hypertension) may in fact develop MHE. 2) These patients have another form of cognitive impairment not related to MHE, as an initial form of cerebrovascular dementia. This is unlikely, as the proportion of altered components of the PHES was similar to that observed for patients with persistent MHE (data not shown), suggesting a similar pathophysiologic process.
The main limitations of the present study concern the limited sample size, the relatively short follow-up to detect MHE after SVR and the lack of cerebral imaging before DAA and after HCV treatment. The study had strict inclusion criteria, and DAA regimens have only been available relatively recently in the Brazilian public health system, leading to a limited sample size. We acknowledge that the lack of central nervous imaging did not allow us to characterize cerebral morpho-functional features in patients with MHE or to exclude alternative causes of cognitive impairment. Additionally, we are aware that the present study did not evaluate serum ammonia levels, biomarkers of oxidative stress or spontaneous portosystemic shunts. This is, however, the case in most real-life studies, and incorporation of these tools would translate to less reproducible and applicable information. A potential criticism could be the absence of assessment of the prognostic value of presence of MHE before DAA or after SVR to predict complications of cirrhosis and/or mortality after SVR. Further studies are warranted to better clarify these relevant questions.
Conclusions
Minimal hepatic encephalopathy is frequent in patients with cirrhosis who achieved SVR after DAA. SVR is associated with low probability of resolution of MHE and may not entirely protect patients from developing de novo MHE. Presence of MHE before DAA, older age, hypertension and hypoalbuminemia after SVR are predictive factors for development of MHE after HCV eradication.





