
INTRODUCTION
Dermatology, the branch of medicine dedicated to diagnosing and managing skin conditions, spans a diverse array of disorders, from widespread issues like acne vulgaris to life-threatening malignancies such as melanoma. Over the last several decades, there has been a remarkable evolution in this specialty, driven by deeper insights into disease mechanisms, advances in diagnostic tools, and the development of novel therapeutic approaches [1].
Skin cancer, encompassing both melanoma and non-melanoma variants, continues to pose a substantial public health challenge on a global scale. Contemporary research has emphasized the refinement of early detection methods alongside the exploration of groundbreaking treatments aimed at optimizing patient prognoses [2]. Likewise, the therapeutic landscape for chronic inflammatory diseases such as psoriasis and atopic dermatitis has dramatically shifted, largely due to the introduction of biologic agents and small molecule inhibitors that target specific immune pathways [3, 4].
Increasingly, dermatologists have recognized the diagnostic value of cutaneous symptoms as indicators of systemic diseases. These manifestations often necessitate a collaborative, multidisciplinary approach for accurate diagnosis and effective management [5]. Simultaneously, cosmetic dermatology has seen surging demand, particularly for non-invasive procedures like injectables and laser-based therapies, fueling continued innovation in aesthetic treatments [6].
The science of wound healing has similarly advanced, focusing on the development of sophisticated wound dressings, the application of bioengineered tissue products, and the use of growth factors to accelerate recovery [7]. In the realm of trichology, research into hair disorders – such as alopecia areata and androgenetic alopecia – has expanded therapeutic possibilities through new treatment modalities [8].
Pediatric dermatology remains an essential subspecialty, tackling conditions that predominantly affect younger populations, such as atopic eczema, diaper dermatitis, and genetically inherited skin diseases [9]. Moreover, the integration of telemedicine into dermatological care has gained momentum, offering unprecedented opportunities to extend specialized services to remote and underserved communities [10].
Through this systematic literature review, we aim to synthesize recent advancements across ten pivotal dermatologic domains. By analyzing current research trends, this work seeks to illuminate the dynamic progression of dermatologic science and its growing impact on clinical care and patient outcomes.
METHODOLOGY
In order to conduct a comprehensive and highquality systematic review on recent advancements in dermatological research, a systematic and structured methodology was implemented. The steps undertaken are detailed below to ensure transparency, reproducibility, and scientific rigor.
Database selection and search strategy
A systematic search was conducted across four major biomedical and clinical databases: PubMed, Scopus, Web of Science, and Embase. These databases were selected based on their broad coverage of peerreviewed medical literature, ensuring the inclusion of high-impact and up-to-date studies. The search focused on articles published between January 2018 and March 2024 to capture the most contemporary advancements in dermatology.
A combination of Medical Subject Headings (MeSH) terms and keyword strategies was employed to optimize search sensitivity and specificity. Key search terms included but were not limited to: “dermatological advancements”, “skin cancer treatment”, “psoriasis therapies”, “atopic dermatitis management”, “biologic therapies”, “neuroendocrine signaling in skin”, and “vitamin D metabolism in dermatology”. Boolean operators (AND, OR) were utilized to strategically combine terms and refine search outcomes.
Eligibility criteria
To ensure the inclusion of relevant and scientifically sound studies, explicit inclusion and exclusion criteria were established:
Study selection process
The selection of studies was carried out in a multiphase screening process:
Title and abstract screening: All identified articles were initially screened by reviewing titles and abstracts. Studies clearly failing to meet the inclusion criteria were excluded at this stage.
Full-text assessment: Eligible articles proceeded to a full-text review to evaluate their methodological quality, relevance, and contribution to dermatological advancements.
Final inclusion: Only studies satisfying all inclusion criteria and demonstrating significant clinical or research contributions were incorporated into the final synthesis.
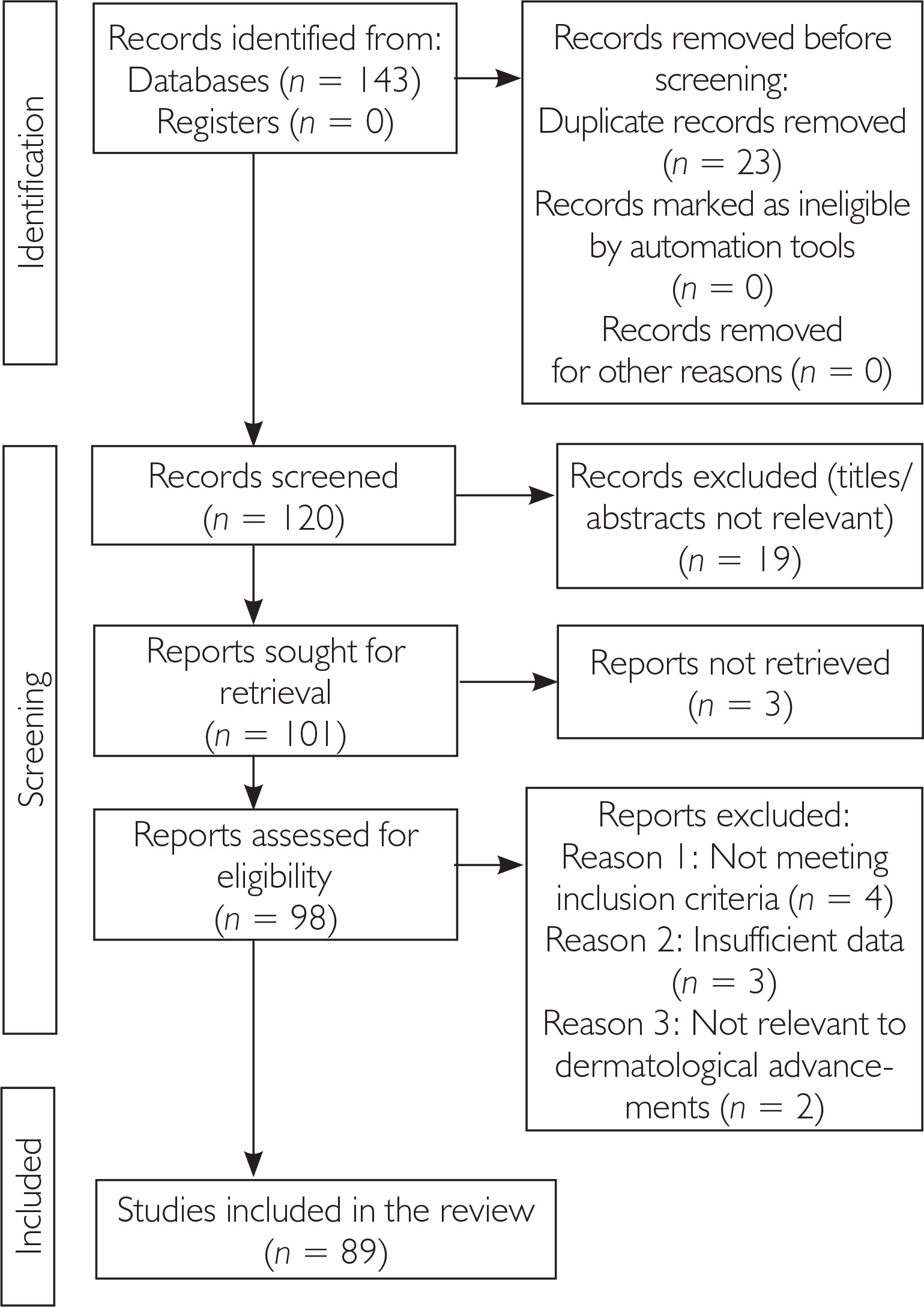
The study selection procedure is depicted through a PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart, illustrating the number of articles retrieved, screened, excluded, and ultimately included.
Quality assessment
To enhance the reliability of this review, a quality appraisal was conducted for all included studies.
For randomized controlled trials (RCTs), the Cochrane risk of bias tool was applied.
For systematic reviews and meta-analyses, the AMSTAR 2 (A Measurement Tool to Assess Systematic Reviews) checklist was utilized.
Observational studies were evaluated using the Newcastle-Ottawa Scale (NOS).
Studies deemed to have a high risk of bias or significant methodological flaws were excluded, thereby ensuring that the synthesized findings are based on robust and credible evidence (fig. 1).
RESULTS
The systematic search across PubMed, Scopus, Web of Science, and Embase identified 143 records. After duplicate removal and title and abstract screening, 120 articles were selected for full-text assessment. Following thorough evaluation against eligibility criteria, 89 studies were included in the final synthesis. Quality appraisal indicated that the majority of the studies exhibited moderate to high methodological rigor, ensuring the reliability of the evidence presented.
Substantial progress has been observed across several dermatologic fields. In skin oncology, the introduction of advanced diagnostic technologies such as dermoscopy, reflectance confocal microscopy, and artificial intelligence-assisted imaging has markedly improved early detection rates for melanoma and non-melanoma skin cancers. Therapeutic strategies have expanded with the use of immune checkpoint inhibitors, BRAF/MEK inhibitors, and research into vitamin D-related pathways, significantly enhancing patient survival outcomes.
Research into neuroendocrine signaling has advanced the understanding of the skin’s role as an endocrine organ. Neuropeptides and localized hypothalamic-pituitary-adrenal axis-like activity are now recognized as key contributors to inflammatory responses and disease exacerbation, particularly under chronic stress, offering new potential therapeutic targets.
The management of acne vulgaris continues to evolve, with traditional treatments like topical retinoids and systemic antibiotics being complemented by emerging therapies such as photodynamic therapy, nitric oxide-releasing agents, and laser-based interventions. Similarly, psoriasis treatment has been transformed through the introduction of biologics targeting tumor necrosis factor-α (TNF-α), interleukin-23 (IL-23), and interleukin-17 (IL-17), alongside new topical agents like roflumilast, expanding options for patients with varying disease severity.
Atopic dermatitis has benefitted from the development of biologic therapies like dupilumab and investigational agents targeting IL-13 and IL-31, as well as topical Janus kinase inhibitors like ruxolitinib, offering new hope for those with moderate to severe disease. The clinical recognition of cutaneous manifestations as indicators of systemic diseases such as lupus erythematosus, diabetes mellitus, and autoimmune disorders has been strengthened, emphasizing dermatology’s critical role in early systemic diagnosis.
In cosmetic dermatology, there is continued growth in minimally invasive rejuvenation techniques including microneedling, chemical peels, and injectables. Advances in laser technologies are providing improved outcomes in photoaging and pigmentation treatments. In the field of wound healing, the application of advanced dressings, growth factors, tissue engineering, and adjunctive therapies such as negative pressure wound therapy (NPWT) and hyperbaric oxygen therapy (HBOT) has resulted in enhanced healing rates for chronic wounds.
Therapeutic strategies for hair disorders have diversified, with new modalities like JAK inhibitors and prostaglandin analogs showing promise for conditions such as alopecia areata and androgenetic alopecia. Finally, teledermatology has emerged as a powerful tool for increasing access to dermatological care, with AI integration poised to further enhance diagnostic capabilities despite ongoing concerns regarding data security and diagnostic accuracy.
To summarize the main thematic findings of the review, table 1 present an overview of advancements across the core areas evaluated.
Table 1
Summary of key dermatological advancements
DISCUSSION
Advances in the detection and management of skin cancer
Skin cancer remains one of the most prevalent and life-threatening malignancies worldwide, with various forms such as melanoma, basal cell carcinoma (BCC), and squamous cell carcinoma (SCC) presenting unique clinical challenges [11]. The urgent need for earlier diagnosis and more effective therapies has driven substantial innovation in recent years, fundamentally transforming the clinical approach to skin cancer.
Early diagnosis continues to be the cornerstone of effective skin cancer management. Dermoscopy, a noninvasive imaging technique, has become indispensable for clinicians by allowing enhanced visualization of subdermal skin structures, thereby facilitating the distinction between benign and malignant lesions [12]. Recent integration of artificial intelligence (AI) technologies into dermoscopic analysis has further improved diagnostic precision, offering automated lesion assessment with impressive accuracy [13]. Complementing dermoscopy, reflectance confocal microscopy (RCM) provides real-time, cellular-level imaging of skin lesions, enabling detailed morphologic evaluation without the need for invasive biopsy [14]. Moreover, advancements in portable imaging devices and smartphone-based dermoscopy systems are expanding diagnostic accessibility even in remote or resource-limited settings, broadening the reach of early detection programs.
Beyond diagnosis, the therapeutic landscape for skin cancer, particularly metastatic melanoma, has evolved dramatically. Targeted therapies such as BRAF inhibitors and immune checkpoint inhibitors have redefined survival expectations for patients with advanced disease [15]. Additionally, localized treatment strategies, including intralesional oncolytic viral therapy and intralesional immunotherapies, offer the benefit of tumorspecific targeting with reduced systemic toxicity [16]. Mohs micrographic surgery (MMS) remains the gold standard for the treatment of non-melanoma skin cancers, ensuring optimal tumor clearance and tissue conservation through meticulous margin assessment [17]. Innovations such as frozen-section immunofluorescence mapping have further refined MMS, enhancing its ability to identify and excise tumor margins with greater precision [18].
Particularly in the management of metastatic melanoma, immunotherapy has revolutionized treatment paradigms. Agents like pembrolizumab and ipilimumab, which inhibit immune checkpoints such as programmed cell death protein 1 (PD-1) and cytotoxic T-lymphocyte-associated protein 4 (CTLA-4), have demonstrated remarkable survival benefits by reinvigorating anti-tumor immune responses [19, 20]. Combination strategies employing dual immune checkpoint blockade or pairing immunotherapy with targeted agents have further elevated response rates and durability of remission, albeit at the cost of increased immune-related adverse effects that require vigilant management [21].
Vitamin D signaling has also emerged as an intriguing area of research in melanoma biology. Traditionally recognized for its role in calcium regulation, vitamin D now appears to influence cellular proliferation, differentiation, and apoptotic pathways relevant to melanoma progression [22, 23]. Activation of the vitamin D receptor (VDR) within melanoma cells modulates gene expression linked to growth control and immune surveillance, offering potential protective effects [23]. Recent investigations suggest that vitamin D deficiency may be associated with poorer melanoma outcomes, prompting interest in vitamin D supplementation as an adjunct to conventional therapies [22].
Experimental approaches exploring vitamin D analogs, designed to maximize anti-cancer efficacy while minimizing hypercalcemic risks, have demonstrated promising results in preclinical studies [24]. Furthermore, combination therapies integrating vitamin D analogs with immune checkpoint inhibitors are under investigation, aiming to potentiate therapeutic responses and overcome resistance mechanisms [22]. Although clinical evidence remains preliminary, the expanding understanding of vitamin D’s role in melanoma offers exciting new therapeutic possibilities [25].
Neuroendocrine regulation of skin physiology and pathology
The skin is increasingly recognized not merely as a passive barrier but as an active neuroendocrine organ, capable of sophisticated communication with the nervous, endocrine, and immune systems [26]. Recent discoveries have emphasized the role of neuropeptides – such as substance P, calcitonin gene-related peptide (CGRP), and vasoactive intestinal peptide (VIP) – produced by keratinocytes, melanocytes, and resident immune cells, in orchestrating diverse physiological processes crucial to skin health [27, 28].
Contemporary research highlights how neuropeptides influence both innate and adaptive immune responses within the skin, modulating the activity of T cells, macrophages, and dendritic cells [28]. This intricate signaling network plays a pivotal role in inflammatory pathways implicated in skin diseases such as psoriasis, atopic dermatitis, and rosacea [29]. Notably, neuropeptide-mediated modulation of cytokine release and leukocyte recruitment has been identified as a key driver of cutaneous inflammation, opening new targets for anti-inflammatory interventions. Furthermore, neuropeptides contribute critically to wound healing, nociception, and responses to ultraviolet (UV) radiation exposure, underscoring their centrality to maintaining skin integrity [30, 31].
A major conceptual advance has been the identification of a local hypothalamic-pituitary-adrenal (HPA)-like axis within the skin [29]. Local production of corticotropin-releasing hormone (CRH) and subsequent cortisol synthesis modulate immune responses and barrier homeostasis, mirroring systemic HPA functions at the cutaneous level [28]. Dysregulation of this local axis has been implicated in a range of dermatological disorders, including inflammatory and autoimmune conditions, suggesting that therapeutic targeting of the cutaneous HPA system may offer novel treatment avenues [28].
The impact of psychological stress on skin health has become increasingly evident, with chronic stress shown to disrupt neuropeptide balance and exacerbate inflammatory dermatoses [27]. For example, stress-induced upregulation of substance P has been associated with the worsening of psoriasis and atopic dermatitis, linking emotional well-being directly to skin disease progression [32]. Emerging therapies aimed at modulating neuropeptide pathways, such as substance P receptor antagonists and CRH inhibitors, are being explored as potential strategies to break the vicious cycle of stress-induced skin inflammation.
The therapeutic implications of these findings are profound. By targeting neuroendocrine circuits at the molecular level, new treatments may offer more personalized and effective options for patients suffering from chronic inflammatory skin conditions [28]. As research into skin neuroimmunoendocrinology advances, it holds the promise of novel interventions that could not only alleviate dermatologic symptoms but also address underlying systemic dysregulation, ultimately leading to improved patient quality of life [28].
Evolving strategies for acne vulgaris management
Acne vulgaris remains one of the most widespread chronic inflammatory skin conditions, significantly impacting both physical appearance and psychological health worldwide. Effective therapeutic strategies address the complex pathogenesis of acne, which includes follicular hyperkeratinization, microbial colonization, sebum overproduction, and inflammation [33].
Topical agents continue to serve as the primary treatment option for patients with mild to moderate disease severity. Retinoids such as tretinoin and adapalene, by promoting normalized keratinocyte differentiation, play a central role in minimizing comedone formation and preventing follicular obstruction [34]. Benzoyl peroxide, known for its potent antimicrobial and anti-inflammatory properties, remains a mainstay of therapy either alone or synergistically with other agents [35]. Inflammatory lesions are often managed with topical antibiotics like clindamycin and erythromycin, although concerns regarding antimicrobial resistance necessitate their use predominantly in combination regimens [36].
For individuals with moderate to severe acne or those who fail to respond to topical therapies, systemic interventions are indicated. Oral antibiotics such as doxycycline and minocycline exert both antimicrobial and anti-inflammatory effects and are commonly prescribed; however, prudent use is recommended to mitigate the risks of resistance and microbiome disruption [37]. Hormonal therapies, particularly combined oral contraceptives containing estrogen and progestin, offer effective control in female patients by decreasing androgen-driven sebaceous activity. Recent studies have also explored the potential use of anti-androgen agents like spironolactone as adjunctive systemic therapies, particularly in hormonally influenced acne, further broadening treatment options [38].
Emerging therapeutic modalities have shown promising efficacy. Photodynamic therapy (PDT) leverages light-activated photosensitizers to selectively target and destroy Cutibacterium acnes while reducing inflammation [39]. Similarly, advancements in laser and light-based technologies, including fractional lasers and intense pulsed light (IPL) devices, have provided alternative avenues for both acne lesion clearance and scar management [40]. Additionally, innovative topical agents, including nitric oxide-releasing formulations and novel retinoid derivatives with enhanced tolerability, are undergoing clinical evaluation and represent a promising frontier in acne therapy [41]. Ongoing research into probiotics and microbiome-modulating treatments offers another exciting direction, targeting dysbiosis as a contributing factor in acne pathogenesis.
Targeted therapeutic innovations in psoriasis treatment
Psoriasis is a chronic, immune-mediated dermatosis characterized by erythematous plaques covered with silvery scales, with its pathophysiology rooted in complex immune dysregulation [42]. The past decade has witnessed transformative advancements in psoriasis management through targeted modulation of specific immunological pathways. Central to psoriasis development is the aberrant activation of innate and adaptive immune cells, particularly T lymphocytes and dendritic cells, which drive keratinocyte hyperproliferation through the release of key pro-inflammatory cytokines, including TNF-α, IL-23 and IL-17 [43, 44].
Biologic therapies have revolutionized the management of moderate to severe psoriasis by selectively inhibiting these critical mediators. Anti-TNF-α agents, including etanercept, adalimumab, and infliximab, were among the first biologics approved, demonstrating significant efficacy in plaque clearance and patient-reported outcomes [45]. Subsequent biologic innovations have targeted the IL-17 pathway, with agents like secukinumab and ixekizumab offering superior clinical responses and durable disease control [46]. Furthermore, inhibitors of IL-23, such as ustekinumab, guselkumab, and risankizumab, have emerged, offering potent and selective suppression of upstream psoriasis drivers [47]. In parallel, small molecule inhibitors provide oral alternatives for patients seeking non-injectable treatments. Janus kinase (JAK) inhibitors such as tofacitinib and baricitinib target intracellular cytokine signaling pathways, showing efficacy particularly in psoriatic arthritis [48].
Phosphodiesterase-4 (PDE4) inhibitors like apremilast act by modulating cAMP levels, providing modest efficacy with a favorable safety profile. The therapeutic landscape has been further enriched by the approval of roflumilast, a next-generation topical PDE4 inhibitor specifically indicated for plaque psoriasis. By increasing intracellular cAMP, roflumilast downregulates pro-inflammatory cytokine production and mitigates keratinocyte proliferation [49]. Phase 3 clinical trials have confirmed its efficacy in achieving significant improvements on the Investigator’s Global Assessment (IGA) scale, demonstrating notable reductions in erythema, scaling, and plaque thickness [50]. Unlike earlier topical agents, roflumilast is well tolerated even on sensitive skin areas such as intertriginous zones, making it a versatile addition to the therapeutic armamentarium (table 2). Integrated into contemporary clinical guidelines, roflumilast offers a practical solution for patients with mild to moderate disease burden who may wish to avoid systemic immunosuppression [51].
Table 2
The biologic therapies for psoriasis, including their targets, clinical efficacy, and common side effects
Breakthroughs in atopic dermatitis therapeutic strategies
Atopic dermatitis (AD) is a chronic, relapsing inflammatory skin disorder characterized by pruritus, eczematous lesions, and profound impacts on patient quality of life. Recent insights into its pathogenesis have highlighted a multifactorial etiology involving skin barrier dysfunction, immune dysregulation, and genetic susceptibilities.
Mutations in key barrier-related genes, notably filaggrin, compromise epidermal integrity, facilitating increased transepidermal water loss and heightened allergen penetration. Concurrently, immune dysregulation characterized by dominant T-helper 2 (Th2) responses, alongside contributions from Th22 and Th17 pathways, perpetuates inflammation and disrupts skin homeostasis. Environmental factors, including microbial imbalance, pollution, and allergen exposure, further exacerbate disease manifestations [52, 53]. Management traditionally relies on restoring the skin barrier and suppressing inflammation. Topical corticosteroids and calcineurin inhibitors remain foundational therapies for acute disease control. However, concerns about adverse effects with chronic steroid use have accelerated the search for safer and more targeted interventions [53].
The advent of biologic therapies has significantly altered treatment paradigms for moderate to severe AD. Dupilumab, anti-alpha subunit of the IL-4 receptor, has shown robust efficacy in reducing disease severity and improving patient-reported outcomes [54]. Additional biologics targeting IL-13 and IL-31 pathways, such as tralokinumab and nemolizumab, are in late-stage development and promise to expand therapeutic options [4]. Beyond biologics, systemic small molecule inhibitors offer promising alternatives. JAK inhibitors like baricitinib and upadacitinib have demonstrated significant reductions in Eczema Area and Severity Index (EASI) scores and pruritus severity [4]. Similarly, crisaborole, a PDE4 inhibitor, offers a nonsteroidal topical option for mild to moderate disease control [4, 49].
A particularly notable recent advancement is the approval of topical ruxolitinib, a selective JAK1/ JAK2 inhibitor, for the treatment of mild to moderate AD. Ruxolitinib suppresses inflammatory cytokines such as IL-4, IL-13, and interferon γ (IFN-γ), directly addressing the underlying immune dysregulation characteristic of the disease. Phase 3 trials have demonstrated significant improvements in EASI scores and pruritus reduction compared to vehicle cream, validating its efficacy [4].
Importantly, ruxolitinib cream offers a favorable safety profile with minimal systemic absorption, making it a particularly attractive option for long-term management in patients concerned about systemic side effects. Its availability broadens the range of individualized treatment approaches and offers new hope for patients refractory to conventional topical therapies [4].
Dermatologic indicators of systemic diseases: diagnostic and prognostic relevance
The skin often functions as a visible window into systemic health, with cutaneous manifestations serving as vital diagnostic and prognostic markers of underlying systemic diseases. Dermatologic signs associated with systemic conditions are diverse, encompassing autoimmune diseases, metabolic disorders like diabetes mellitus, and connective tissue diseases such as lupus erythematosus [55]. Timely recognition of these manifestations is critical as early dermatologic clues can precede systemic involvement and significantly impact clinical outcomes.
In systemic lupus erythematosus (SLE), dermatologic manifestations are among the most frequent clinical features, with approximately 85% of patients displaying cutaneous involvement during the disease course [56]. Cutaneous lupus erythematosus (CLE) comprises several distinct clinical variants, including acute cutaneous lupus erythematosus (ACLE), which presents with transient erythematous macules and papules typically distributed in a malar pattern, and chronic cutaneous lupus erythematosus (CCLE), characterized by discoid lesions that frequently result in scarring and dyspigmentation [57]. Subacute cutaneous lupus erythematosus (SCLE) presents with nonscarring, psoriasiform, or annular plaques, frequently associated with significant photosensitivity [58]. Emerging data highlight the importance of differentiating CLE subtypes accurately as specific patterns correlate with distinct systemic disease activity and prognostic outcomes.
In diabetes mellitus (DM), a range of dermatologic abnormalities reflect both the microvascular and macrovascular complications inherent to chronic hyperglycemia. Diabetic dermopathy, marked by atrophic, hyperpigmented patches predominantly on the shins, is among the earliest and most common findings [59]. Other important cutaneous manifestations include necrobiosis lipoidica diabeticorum, characterized by shiny, atrophic plaques with a yellowish center [60], and diabetic foot ulcers, which significantly increase the risk of infection and limb amputation if not promptly managed [59]. Additionally, fungal infections such as candidal intertrigo are more prevalent among diabetic patients due to immune dysfunction and altered skin barrier properties, necessitating vigilant dermatologic surveillance [59].
Autoimmune diseases are another major domain where skin involvement is often prominent. In dermatomyositis, classic features such as heliotrope rash and Gottron’s papules are considered hallmark diagnostic signs and are frequently accompanied by proximal muscle weakness [61]. Scleroderma, a disease of fibrosis and vasculopathy, manifests dermatologically through features like sclerodactyly, Raynaud’s phenomenon, and painful digital ulcers [62]. Autoimmune blistering disorders, including pemphigus vulgaris and bullous pemphigoid, involve mucocutaneous blister formation and can lead to significant morbidity if diagnosis and immunosuppressive treatment are delayed [58].
The recognition and management of cutaneous manifestations of systemic diseases demand a collaborative, multidisciplinary approach. Dermatologists often work closely with rheumatologists, endocrinologists, and internists to optimize diagnosis, monitor disease progression, and tailor therapy [63]. Management strategies range from systemic immunosuppressants and targeted biologics to adjunctive topical and supportive therapies aimed at reducing skin morbidity, enhancing quality of life, and preventing systemic complications. Moreover, the integration of dermatologic findings into systemic disease scoring systems, such as the Systemic Lupus International Collaborating Clinics (SLICC) criteria for SLE, underscores the critical diagnostic weight of cutaneous presentations [64].
Contemporary trends and innovations in cosmetic dermatology
Cosmetic dermatology has experienced tremendous growth, propelled by technological innovation, greater societal acceptance, and patient demand for minimally invasive procedures to enhance aesthetic appearance. Current trends emphasize not only cosmetic outcomes but also patient safety, natural results, and minimal recovery times [65]. Advancements continue to refine procedural techniques, enhance device technologies, and expand the therapeutic arsenal available to dermatologists.
Minimally invasive skin rejuvenation procedures, such as microneedling, chemical peels, and microdermabrasion, are increasingly sought after for their effectiveness combined with low risk profiles. Microneedling, or collagen induction therapy, utilizes fine needles to create controlled dermal injury, thereby stimulating neocollagenesis and improving skin texture, elasticity, and tone [66, 67]. The integration of adjunctive agents, such as platelet-rich plasma (PRP) or topical growth factors with microneedling, has been shown to further augment clinical outcomes [68]. Chemical peels employ exfoliative agents like alpha-hydroxy acids (AHAs) and trichloroacetic acid (TCA) to enhance cellular turnover, reduce fine lines, ameliorate pigmentation disorders, and even treat early photoaging signs [65]. Meanwhile, microdermabrasion mechanically exfoliates the epidermis, promoting smoother, more luminous skin through safe and minimally painful procedures [65].
Injectable treatments continue to dominate the nonsurgical cosmetic sector. Botulinum toxin injections, by transiently inhibiting acetylcholine release at the neuromuscular junction, effectively attenuate dynamic facial lines, such as glabellar frown lines and crow’s feet [69]. Dermal fillers, particularly hyaluronic acid-based products, provide volumetric enhancement and soft tissue augmentation for areas like the lips, cheeks, and nasolabial folds. Newer generations of dermal fillers are engineered with varying crosslinking densities, providing enhanced durability, tissue integration, and customized aesthetic outcomes based on facial anatomy [65].
Laser and energy-based devices have similarly transformed cosmetic dermatology, offering highly targeted treatment of photoaging, dyschromia, vascular lesions, and unwanted hair. Fractional CO2 and erbium lasers deliver precise dermal remodeling with reduced downtime compared to traditional resurfacing methods. Intense pulsed light (IPL) therapies effectively target vascular and pigmented lesions while improving overall skin tone and texture [70]. Emerging technologies such as picosecond lasers and combination radiofrequency-microneedling devices are expanding therapeutic possibilities for scar revision, skin tightening, and even tattoo removal [65, 70].
Patient education and informed consent are critical in cosmetic dermatology practice to align patient expectations with achievable outcomes and to minimize dissatisfaction or medicolegal risk [65]. Recent emphasis on individualized aesthetic assessment and combination therapy planning seeks to achieve natural, harmonious results that respect facial proportions and aging physiology, rather than aiming for exaggerated corrections [65]. Ongoing research into safety optimization, product innovation, and minimally invasive techniques continues to drive the field forward [67 , 70].
Cutting-edge advances in wound healing and tissue regeneration
Wound healing is a complex, dynamic biological process encompassing inflammation, tissue proliferation, and remodeling, all aimed at restoring the structural and functional integrity of injured tissue. Despite major advancements in wound management strategies, chronic wounds such as diabetic ulcers, venous ulcers, and pressure injuries continue to present major clinical and economic challenges worldwide [7, 71]. As such, substantial efforts have been directed toward developing more effective, targeted therapies to enhance wound healing and reduce associated morbidity.
Advanced wound dressings form a critical component of modern wound care protocols. Hydrocolloid dressings provide a moist environment conducive to autolytic debridement, while foam dressings offer superior absorption for exudative wounds and protect against mechanical trauma [72]. Hydrogels maintain hydration of dry wounds, thereby promoting epithelial migration and tissue repair. Antimicrobial dressings impregnated with agents like silver, iodine, or polyhexanide reduce bacterial colonization and biofilm formation, supporting improved healing outcomes in contaminated wounds [73].
Growth factors are integral mediators of the wound healing cascade. Platelet-derived growth factor (PDGF), transforming growth factor-β (TGF-β), and vascular endothelial growth factor (VEGF) orchestrate critical processes such as fibroblast recruitment, angiogenesis, collagen deposition, and epithelialization [74]. Therapeutic approaches including recombinant growth factor formulations and autologous PRP applications have demonstrated efficacy in accelerating healing, particularly in non-healing chronic ulcers. Emerging strategies also involve sustained-release delivery systems for growth factors, aiming to optimize their bioavailability and therapeutic action at the wound site.
Tissue engineering offers transformative potential for wound healing through the application of biomaterial scaffolds, cellular therapies, and bioactive agents. Biodegradable scaffolds composed of collagen, hyaluronic acid, or synthetic polymers provide structural support for cellular infiltration, neovascularization, and extracellular matrix deposition [75]. Cellular therapies utilizing mesenchymal stem cells (MSCs) or keratinocyte cultures offer regenerative capabilities through paracrine signaling and differentiation into tissue-specific lineages. The advent of 3D bioprinting techniques to create custom-designed skin substitutes represents an exciting frontier in wound management [7].
Adjunctive technologies such as NPWT and HBOT have become standard adjuncts in complex wound care. NPWT promotes wound contraction, angiogenesis, and granulation tissue formation by applying controlled subatmospheric pressure to the wound bed. HBOT enhances tissue oxygenation, improves neutrophil bacterial killing capacity, and stimulates angiogenesis, making it a valuable adjunct in ischemic or refractory wounds [76]. The development of portable NPWT systems and advanced HBOT protocols continues to expand access and optimize therapeutic outcomes for patients with chronic wounds.
Advances in the diagnosis and management of hair disorders
Hair disorders represent a diverse group of conditions affecting the scalp and hair follicles, encompassing diseases such as alopecia areata, androgenetic alopecia, and hirsutism. These disorders frequently have profound psychosocial impacts, contributing to reduced self-esteem and diminished quality of life in affected individuals [8]. Recent years have witnessed notable strides in understanding the pathogenesis of these conditions and in expanding available therapeutic options, offering renewed optimism for patients and clinicians alike.
Alopecia areata is a non-scarring autoimmune condition characterized by sudden, patchy hair loss resulting from immune-mediated destruction of hair follicles. Advances in research have shed light on its immunopathogenesis, implicating T-cell infiltration and aberrant cytokine signaling, particularly the roles of interferon-γ and IL-15, in disease progression [48]. Therapeutic strategies traditionally include topical corticosteroids and intralesional steroid injections for localized disease, with systemic agents such as oral corticosteroids and methotrexate reserved for extensive involvement [8]. The emergence of Janus kinase (JAK) inhibitors has revolutionized management, with agents like tofacitinib and baricitinib showing significant efficacy in clinical trials [48]. Ongoing investigations into targeted immunotherapies, including monoclonal antibodies against IL-2 and IL-15 receptors, highlight a promising frontier for achieving long-term disease control with reduced systemic toxicity [58].
Androgenetic alopecia, commonly known as male- or female-pattern hair loss, is a progressive condition driven by genetic susceptibility and androgen-mediated miniaturization of hair follicles. Research has underscored the critical roles of androgen receptor sensitivity, 5α-reductase enzyme activity, and alterations in the scalp microenvironment in the pathophysiology of this disorder [8]. Standard treatments such as topical minoxidil and oral finasteride aim to prolong the anagen (growth) phase and prevent follicular miniaturization [58]. Low-level laser therapy (LLLT) has gained traction as a non-invasive adjunct to stimulate hair regrowth [8]. Emerging therapies under investigation include prostaglandin analogs and agents modulating the Wnt/β-catenin signaling pathway, both of which target early molecular drivers of follicular cycling, offering hope for more targeted and sustained regrowth interventions [58].
Hirsutism, defined by excessive terminal hair growth in a male distribution pattern in females, often reflects underlying hyperandrogenism. Pharmacologic management is aimed at reducing androgen production or blocking androgen receptor activity. Combined oral contraceptives are first-line therapies, often supplemented by anti-androgens such as spironolactone and cyproterone acetate [58]. Insulin-sensitizing agents like metformin may also be employed, particularly in cases associated with polycystic ovary syndrome (PCOS). In cases refractory to medical therapy, physical modalities such as laser hair removal and electrolysis provide effective long-term solutions by selectively targeting and destroying hair follicles [8]. Innovations in laser technologies, such as the development of longer wavelength diode lasers and combination laser systems, have further improved efficacy and safety profiles, even in patients with darker skin types [8].
Pediatric dermatology: specialized approaches for childhood skin diseases
Pediatric dermatology addresses a broad spectrum of dermatologic disorders unique to the pediatric population, ranging from common inflammatory conditions like eczema to rare congenital and genetic skin diseases. Management strategies must be specifically tailored to the unique physiological and developmental considerations of children [5, 9]. Understanding the distinct presentations and therapeutic needs of pediatric patients is essential for achieving optimal outcomes and ensuring healthy development.
Atopic dermatitis (eczema) remains one of the most prevalent pediatric skin conditions, characterized by chronic, pruritic, and inflammatory lesions often localized to flexural surfaces [4, 48]. Its multifactorial pathogenesis involves genetic predispositions, immune dysregulation (especially Th2-dominated inflammation), and environmental insults. Management centers around restoring the skin barrier with emollients, controlling inflammation with topical corticosteroids and calcineurin inhibitors, and reducing pruritus with antihistamines. Recent advances emphasize the importance of early intervention with proactive barrier repair strategies to prevent atopic march – the progression to allergic rhinitis and asthma – highlighting the broader implications of eczema management in systemic health [52].
Diaper dermatitis is another frequent concern in infancy and early childhood, primarily resulting from prolonged exposure to moisture, friction, and irritants like ammonia from urine breakdown [58]. Preventative strategies include frequent diaper changes, gentle cleansing, and the liberal application of barrier creams containing zinc oxide or petrolatum. Emerging products incorporating skin microbiome-friendly formulations and anti-inflammatory botanical extracts aim to further reduce irritation and restore microbial balance, promoting faster healing.
Genetic skin disorders present unique challenges due to their chronicity and multisystem involvement. Conditions such as epidermolysis bullosa, ichthyosis, and congenital melanocytic nevi often manifest early in life and require multidisciplinary management involving dermatology, genetics, pediatrics, and sometimes surgical teams [58]. Treatment focuses on symptom control, prevention of secondary complications, and psychosocial support. Recent advances in gene therapy, such as ex vivo gene-corrected epidermal grafts for epidermolysis bullosa, represent groundbreaking developments with the potential to offer curative interventions in the future [58]. Early diagnosis through genetic testing and patient-tailored management plans are critical for improving both dermatologic and systemic outcomes in these patients.
Telemedicine in dermatology: expanding access and enhancing patient care
Telemedicine has become an increasingly integral component of dermatological care, particularly in the wake of technological advances and changing healthcare delivery paradigms. Its applications extend across diagnosis, management, education, and triage, providing critical services to both urban and rural populations [77]. The COVID-19 pandemic further accelerated teledermatology adoption, cementing its role as a cornerstone of contemporary dermatologic practice [78].
Teledermatology effectively bridges the geographical divide, offering patients in rural or underserved areas timely access to dermatological expertise [79]. By utilizing store-and-forward (asynchronous) technologies and live-interactive (synchronous) video consultations, specialists can review clinical images, provide diagnostic opinions, and recommend treatments without the need for in-person visits [80]. Recent studies have demonstrated diagnostic concordance rates between teledermatology and face-to-face consultations approaching 90%, supporting its validity as a reliable alternative in many clinical scenarios [81, 82].
Beyond improving accessibility, telemedicine offers notable enhancements in patient convenience and satisfaction. Remote consultations eliminate the need for travel, reduce wait times, and facilitate follow-up care, leading to greater patient engagement and adherence to therapeutic regimens [83]. Teledermatology platforms are increasingly integrating electronic prescribing and automated follow-up reminders, further streamlining the care continuum [84].
In acute and emergency settings, telemedicine enables rapid triage of dermatological conditions, allowing clinicians to prioritize care based on the severity of presentations. This approach has been shown to decrease unnecessary emergency department visits and hospital admissions for dermatological complaints [77]. Specialized teledermatology programs for inpatient consults, post-operative wound monitoring, and chronic disease management (e.g., psoriasis, hidradenitis suppurativa) are expanding, offering additional clinical benefits across care settings [85].
Despite its many advantages, teledermatology faces challenges that warrant careful consideration. Limitations in image quality, variability in lighting conditions, and the inability to perform physical palpation may occasionally hinder diagnostic accuracy. Additionally, issues surrounding data security, patient confidentiality, and regulatory compliance must be addressed to maintain trust and ensure ethical practice [86]. Ongoing innovations, including AI-assisted diagnostic support tools and standardized imaging protocols, are being developed to mitigate these limitations and enhance teledermatology’s diagnostic precision.
Emerging research priorities and persistent knowledge gaps in dermatology
Looking ahead, future research efforts in dermatology must strategically address several critical domains to build upon the substantial therapeutic advancements achieved thus far while overcoming existing limitations (fig. 2). One major priority is the long-term evaluation of novel therapies, including recently approved biologic agents and topical treatments such as roflumilast and ruxolitinib. Although these agents have demonstrated promising short-term efficacy and safety profiles, the chronic nature of most dermatological diseases necessitates prolonged treatment, raising concerns about potential immunologic consequences, adverse effects, and the development of therapeutic resistance over time [49]. Robust longitudinal studies and real-world evidence are essential to fully characterize the risk-benefit profile of these newer interventions and guide their optimal use.

Another burgeoning area of importance is the integration of personalized medicine into dermatological practice. Although precision medicine has revolutionized oncology and other medical disciplines, its full potential remains largely untapped in dermatology. Future investigations should emphasize the utilization of genetic, epigenetic, proteomic, and metabolomic data to better stratify patients and predict therapeutic responses [50]. The development of individualized treatment algorithms based on molecular profiling could maximize therapeutic efficacy, minimize adverse events, and enhance cost-effectiveness, representing a paradigm shift toward truly personalized dermatological care.
Significant gaps also persist in the understanding of the immunopathogenesis of common skin diseases, including psoriasis, atopic dermatitis, and melanoma. While it is well recognized that immune dysregulation plays a central role, the precise molecular triggers initiating and sustaining chronic inflammation remain incompletely understood. In melanoma, in particular, the mechanisms underpinning resistance to immune checkpoint inhibitors and targeted therapies such as BRAF/MEK inhibitors warrant urgent investigation [15, 20]. Addressing these fundamental knowledge gaps could enable the development of next-generation therapies that overcome current limitations and improve long-term survival rates.
The role of the skin microbiome in dermatological health and disease is another fertile area for exploration. Although growing evidence suggests that dysbiosis contributes to conditions like acne, psoriasis, and atopic dermatitis, the mechanistic pathways linking microbial alterations to immune dysfunction require further elucidation. Future research should aim to identify specific microbial signatures associated with disease phenotypes and investigate microbiome-modulating therapies, such as probiotics, prebiotics, and postbiotics [33–35, 87]. Importantly, understanding how conventional treatments alter the skin microbiome could guide the design of combination strategies that simultaneously treat disease while preserving microbial homeostasis.
Emerging technologies, notably artificial intelligence (AI) and machine learning, promise to redefine diagnostic accuracy and therapeutic decision-making in dermatology. Although AI-powered tools for skin cancer detection and triage have shown high sensitivity and specificity in controlled studies, real-world validation and standardization are imperative before widespread clinical adoption [2, 13]. Furthermore, AI applications in disease monitoring, treatment outcome prediction, and personalized patient education represent exciting frontiers that warrant robust research investment. Advancements in non-invasive imaging techniques and biomarker discovery also offer potential for earlier diagnosis and more precise disease monitoring, enhancing clinical outcomes across diverse dermatological conditions [88].
Finally, the psychosocial burden of chronic skin diseases deserves greater scholarly attention. Despite the well-documented associations between conditions like psoriasis, atopic dermatitis, and acne with depression, anxiety, and impaired quality of life, mental health considerations often remain underemphasized in clinical practice and research design [89]. Future studies should prioritize holistic care models that integrate dermatological treatment with psychological support, aiming not only to improve dermatologic outcomes but also to restore mental well-being and social functioning. Such integrative approaches could significantly enhance overall patient satisfaction and quality of life.
CONCLUSIONS
This comprehensive systematic review underscores the dynamic and multifaceted nature of contemporary dermatology, spanning a wide array of subfields ranging from skin cancer detection and therapeutic innovations to pediatric dermatology, cosmetic advancements, and the expanding role of telemedicine. Through critical appraisal of recent breakthroughs, novel treatment modalities, and technological integrations, this review highlights the evolving strategies that are reshaping clinical practice and enhancing patient care. Notably, advances in biologic therapies, small molecule inhibitors, targeted diagnostics, and regenerative medicine have dramatically improved outcomes across numerous dermatological diseases. Simultaneously, the growing adoption of teledermatology has democratized access to specialized services, particularly benefitting patients in remote and underserved regions. The integration of artificial intelligence, microbiome science, and precision medicine is poised to further refine diagnostic capabilities and personalize therapeutic approaches, marking the dawn of a new era in dermatological practice.
However, this rapidly advancing field also brings forth new challenges, including the need for longterm safety surveillance, the validation of emerging technologies, and the imperative to address psychosocial dimensions of chronic skin diseases. As such, continuous professional education, interdisciplinary collaboration, and patient-centered research initiatives are essential to harness these advancements effectively. Ultimately, by remaining attuned to scientific innovations, embracing holistic and personalized care models, and fostering equitable access to dermatological services, healthcare providers can significantly elevate patient outcomes, optimize quality of life, and contribute to the ongoing evolution of dermatological excellence.










