
Introduction
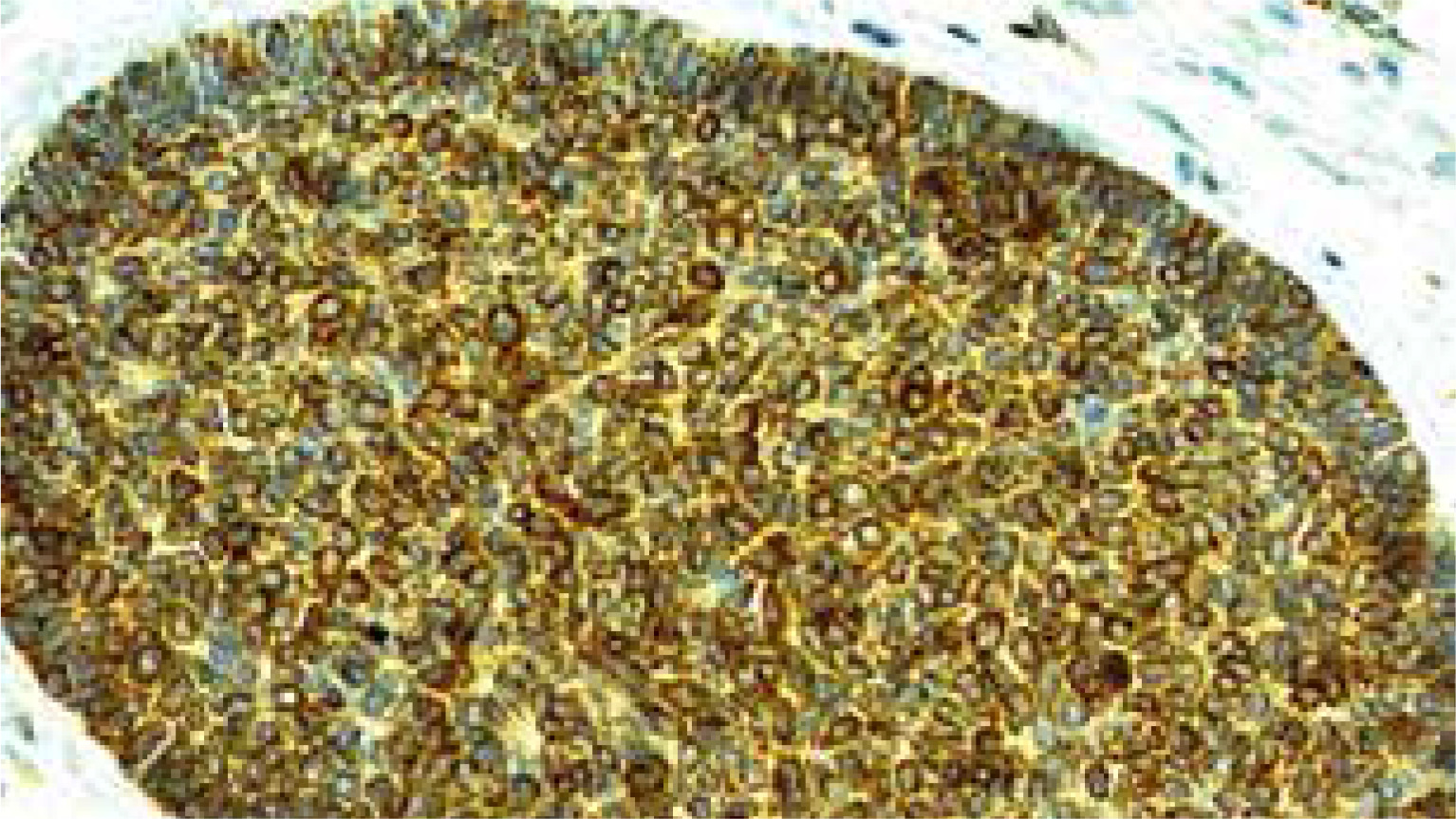
Basal cell carcinoma (BCC) occurs in 90% of all skin malignancies, in 70% of keratinocyte tumours with a rate of 2000 cases per 100 000 population [1, 2]. Together squamous cell carcinoma (SCC) and BCC constitute the vast majority of skin cancers with a ratio of 1 : 4 [3, 4]. In the majority of cases, photoexposed cheeks and also nose are affected, and although the progression of BCC is usually slow, the tumour can result in local destruction if surgery is delayed, but the metastasis rate does not exceed 0.5% [5–7]. BCC varies in aggressiveness within its forms. Nodular forms (Figure 1) are non-aggressive and the most common ones, and as a rule are excised completely, in contrast to the aggressive types – infiltrating, micronodular, morpheaform, sclerosing, metaplastic or rodent ulcer which show a high recurrence rate [8–10]. At the same type, basosquamous cell carcinoma (BSC) as a morphologically intermediate type between BCC and SCC is more invasive than BCC and more prone to local recurrence and metastasis [7, 11–13].
The hypotheses regarding the origin and differentiation of BCC are still a matter of controversy. According to Lever, BCC is not derived from the basal cell of epidermis but like a hamartoma or nevoid tumour originates from the primary epithelial germ cells [14]. In studies on the expression of cytokeratin in BCC and epidermal basal cell, the CK profile of BCC was almost identical to that of the outer root sheath [15]. Kruger stated that BCC could be derived from the outer root sheath and/or or the bulge region of the vellus hair follicle [16]. BCC as well as trichoblastoma go through the common differentiation pathway, and are neoplasms with follicular differentiation. The relationship between BCC and vellus hair follicle remains to be determined in further studies. Results of various studies related to evaluation of the selected immunohistochemical markers expression in skin cancers explore their predictive value on the course of these tumours [17–20]. CK15 is a specific stem cell marker and is expressed in the bulge region of the human hair follicle, the outermost layer of the outer root sheath of the hair follicle, basal layer of the epidermis, and eccrine glands [17, 18]. In cases of cutaneous malignancies, previous studies have shown that CK15 is mainly expressed by neoplasm suspected to be of follicular origin [18–20]. Bmi-1 is expressed in the nuclei of basal and suprabasal keratinocytes, basal cells of sebaceous glands, sweat glands, and in the bulge area and external root sheath of hair follicles. Bmi-1 was originally identified as an oncogene inducing leukaemia, but has also been overexpressed in a variety of human solid tumours. A recent study has suggested that Bmi-1 oncogene contributes to the pathogenesis of BCC [21]. Whereas, Bcl-2 is the first identified and best known anti-apoptotic gene. There are some studies indicating that Bcl-2 positive tumours have a slower course and better prognosis [22].
Aim
The aim of our study was to evaluate the immunoexpression of Bmi-1, CK15 and Bcl-2 in BCCs. Another purpose was to find a possible association between the immunoexpression of Bmi-1, CK15 and Bcl-2 and the histopathological type of BCC.
Material and methods
Patients
The histoclinical analysis included 56 specimens from patients (66.1% males, N = 37 and 33.9% females, N = 19), aged 67–92 (average: 75 years) with basal-cell carcinoma (BCC) of the skin (cheek – 51, nose – 5) who underwent standard surgical excision (Department of Plastic, Reconstructive and Aesthetic Surgery, Medical University of Lodz, Poland) between 2013 and 2019. The patients were Caucasians with a skin phototype between II and III.
All tissue sections taken from postoperative material were routinely fixed in formalin, processed, embedded in paraffin, and stained with haematoxylin and eosin. Histopathological diagnoses were established according to the current WHO standards. All cases of BCC were divided into four groups: non-aggressive – nodular (23 cases), and aggressive – infiltrative (13 cases), nodular/infiltrative (13 cases), and BSC – basosquamous (7 cases).
Immunohistochemistry
Immunohistochemical staining was carried out according to a standard method. 3-μm tissue sections were deparaffinised in xylene and rehydrated through a graded alcohol series. Heating in a microwave oven in a target retrieval solution pH 9.0 (TRS High pH; Dako) for 30 min was used for antigen retrieval. Endogenous peroxidase activity was quenched with 0.3% hydrogen peroxide in methanol for 30 min. The sections were washed with TBS and incubated with primary antibodies against: Bmi-1 (Invitrogen, USA, dilution 1 : 600, Catalog number PA5-23308), and CK15 (Invitrogen, USA, dilution 1 : 400, Catalog number MA1-90926), Bcl-2 Oncoprotein (Dako, RTU- Flex, clone 124, Catalog number IR 614). After washing, an adequate EnVision-HRP detection system (Dako, Carpinteria, CA, USA) was used. 3,3’-diaminobenzidine was used as the chromogen. After counterstaining with Mayer’s haematoxylin, the slides were washed, dehydrated, cleared in xylene and coverslipped. Negative controls for immunohistochemical staining were prepared with primary antibodies replaced by the antibody diluent.
Evaluation of Bmi-1, CK15 and Bcl-2 immunoexpression
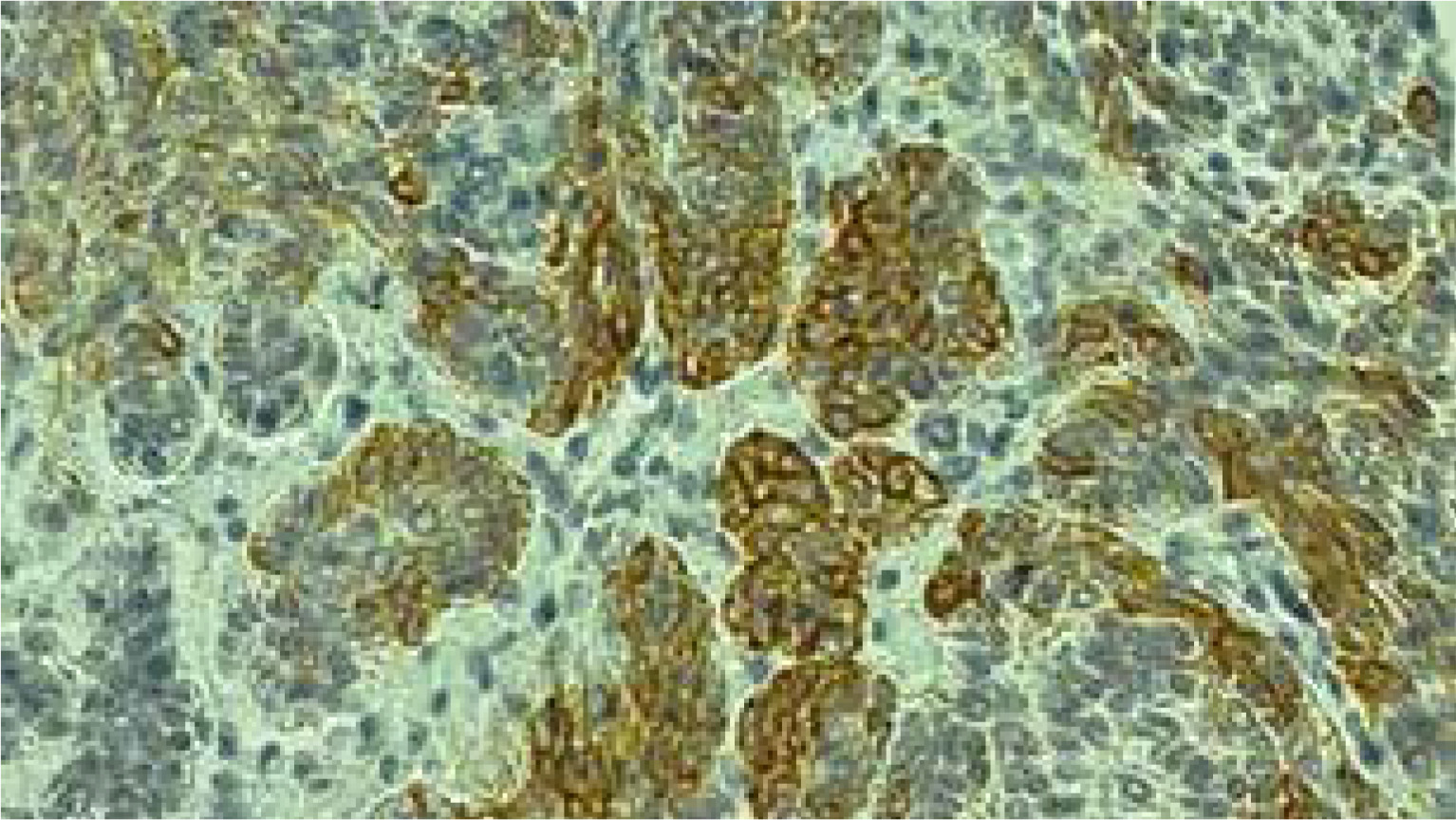
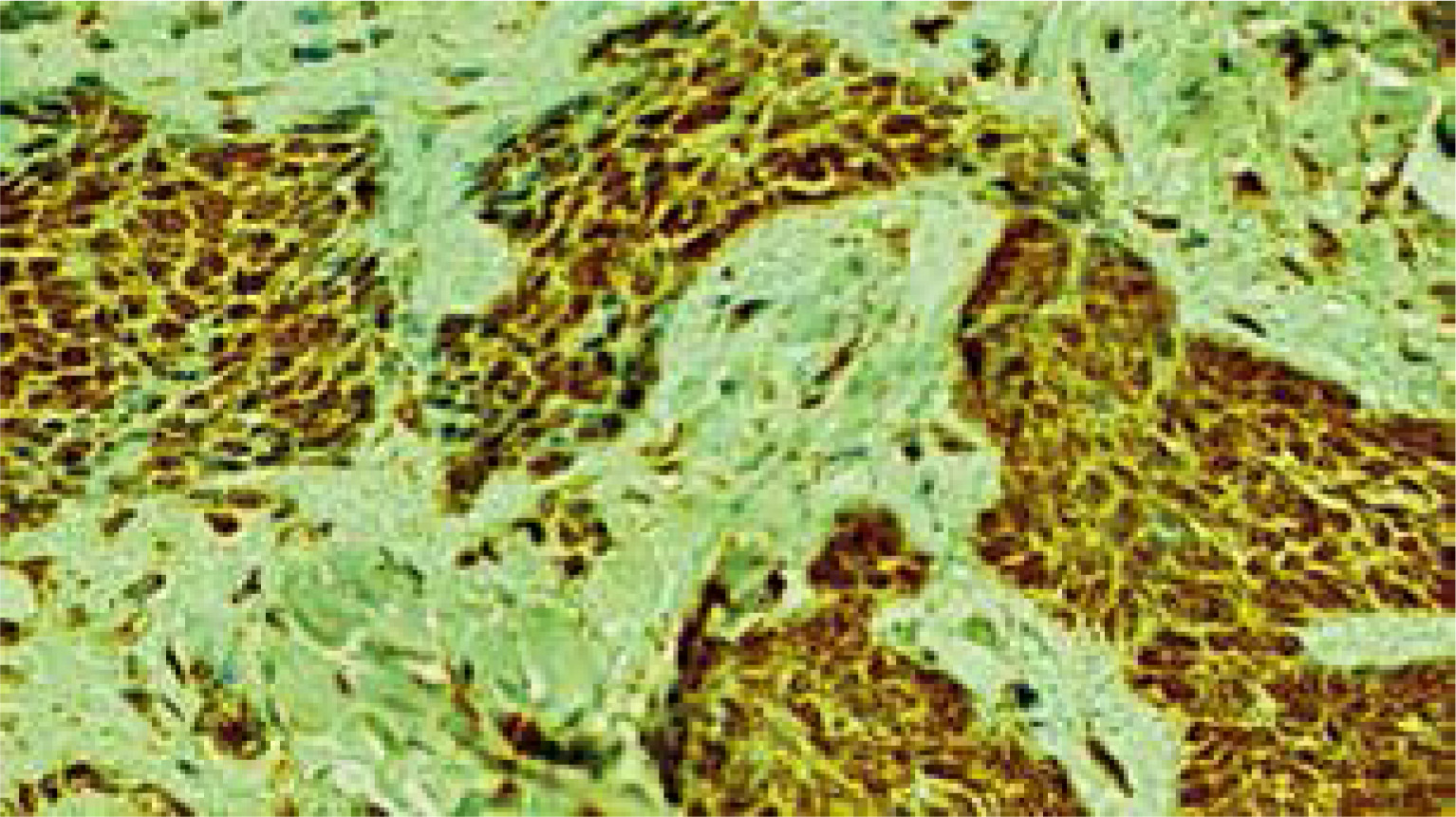
Immunohistochemical staining was carried out according to a standard method. The semiquantitative immunohistochemical analysis was done under the light microscope (Olympus BX41) to assess the expression of Bcl-2, CK15 and Bmi-1 proteins in the cancer cells. The sections were considered positive for Bcl-2 and CK15 in the presence of cytoplasmic staining (Figures 1 and 2, respectively) and for Bmi-1 in the presence of nuclear immunostaining (Figure 3).
The immunoreactivity was graded subjectively: as 0 (no or < 5% positive cells), 1+ (approximately 6–25%), 2+ (approximately 26–50%), 3+ (approximately 51–75%), and 4+ (> 75% positive cells). Grades 1+ and 2+ of positive staining were considered “low” and 3+ and 4+ – “high”.
Statistical analysis
Immunoexpression of Bmi-1, CK15 and Bcl-2 in different BCC types was compared using the Kruskal-Wallis test. In a situation where this test showed the existence of statistically significant differences, a post hoc test of multiple comparisons of mean ranks was performed. This allowed to determine which pairs of tumours differ from each other in terms of the expression of a given protein.
Results
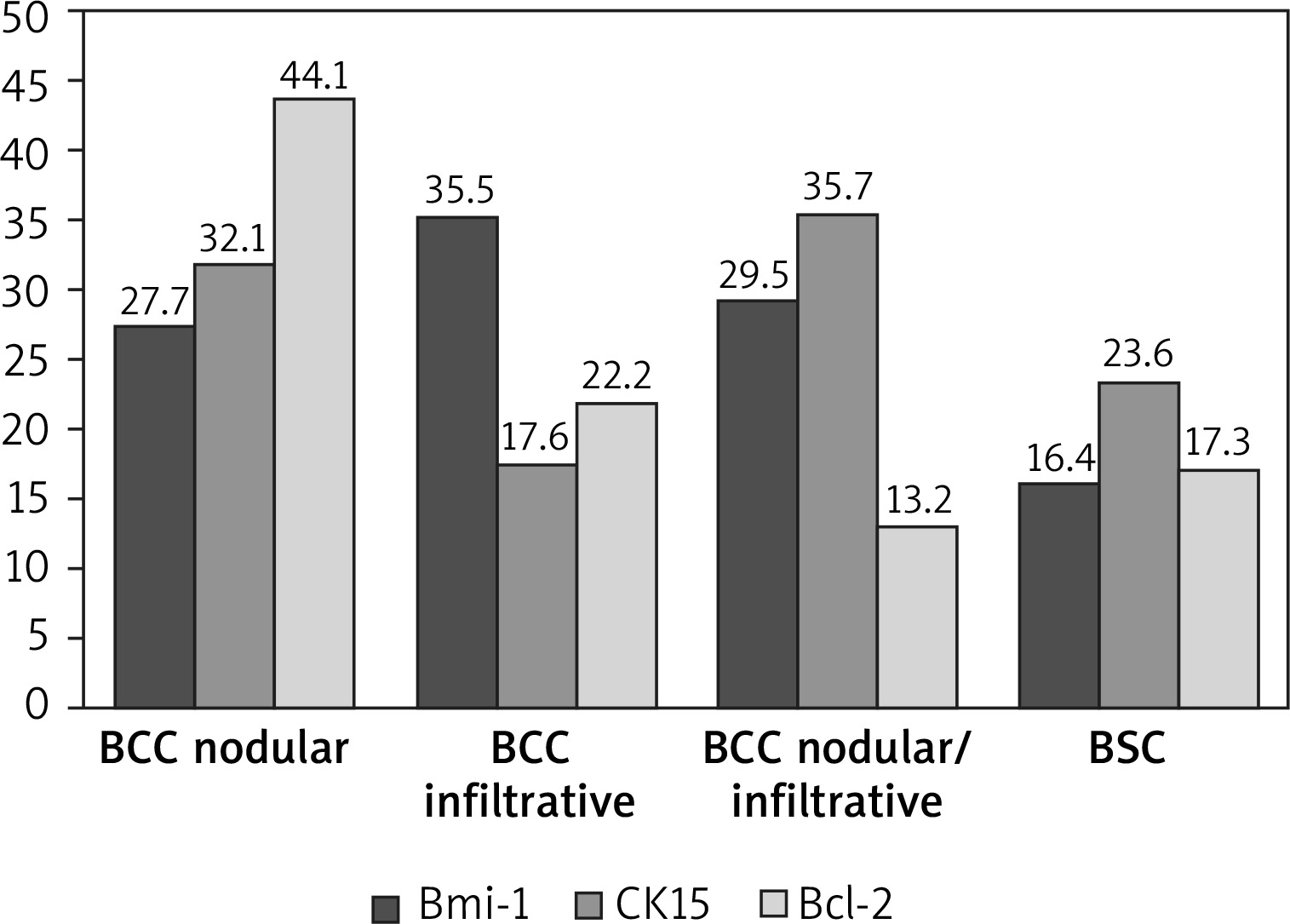
The nuclear immunoexpression of Bmi-1 was confirmed in all BCCs of our study group. The highest positivity levels 3–4+ in the nodular type constituted 91.3%, 4+ in infiltrative – 92.3%, 4+ in nodular/infiltrative – 69.2%, 3+ – 30.8%, in BSC 3+ – 42.8%, and 28.6% each for 2+ and 4+ (Table 1). The Kruskal-Wallis test showed differentiation in the level of Bmi-1 expression between different types of cancer (H = 9.50; p = 0.0233). Based on the post hoc test of multiple comparisons of mean ranks, it was found that the statistically significant difference was for infiltrative BCC tumours, where the expression was the highest, and BSC, where the expression was the lowest (p = 0.0437) (Table 2, Figure 4).
Table 1
The level of Bmi, CK15, Bcl-2 positivity in individual types of BCC
Table 2
Post hoc test results for multiple comparisons of mean ranks (the table presents the probability of differences)
Low grade positivity in CK15 staining was noted in non-aggressive as well as aggressive types of BCCs. The lowest grade – 0 was less frequent if there was a nodular component (nodular BCC – 39.1%, nodular/infiltrative BCC – 15.4%). Grade 0 was the most frequent in infiltrative BCCs (84.6%), whereas in BSCs it was seen in 42.9% (Table 1).
In total BCCs, low grade level 0–1+ constituted 52.1% of nodular, 46.2% – nodular/infiltrative, 92.3% – infiltrative, and 100% – BSC (Table 1).
Levels 2–3+ were seen in nodular BCC – 47.8%, nodular/infiltrative BCC – 53.8%, infiltrative – 7.7%, but no positivity at these ranges was found in BSC (Table 1).
The Kruskal-Wallis test showed the differentiation of CK15 expression between the types of tumours studied (H = 11.42; p = 0.0096). On the basis of post hoc test of multiple comparisons of mean ranks, a statistically significant difference was found between infiltrative and nodular BCC (p = 0.0407) and between infiltrative and nodular/infiltrative BCC (p = 0.0283). Infiltrative BCC was characterized by a lower level of CK15 expression than both types of cancer mentioned above (Table 2, Figure 4).
Bcl-2 positivity was seen in 56 specimens of BCC including nodular/infiltrative BCC – 0 (n = 4) (Table 1). Positivity on a higher level 3–4+ was revealed only in nonaggressive BCCs nodular group – in 95.6% (Table 1). Low-grade (1–2+) positivity was confirmed mainly in the group of aggressive BCC in 100% – of infiltrative BCC as well as BSC, and in infiltrative/nodular BCC (including cases of 0) (Table 1). The lowest (0–1+) positivity was noted in 76.9% of nodular/infiltrative BCC, 71.4% of BSC, and in 38.4% of infiltrative BCC (Table 1). The Kruskal-Wallis test confirmed the differentiation of Bcl-2 expression depending on the type of the tumour (H = 39.85; p < 0.0001). The highest level of Bcl-2 expression was found in nodular BCC, which differed in this respect from infiltrative BCC (p = 0.0007), nodular/infiltrative BCC (p < 0.0001) and BSC (p = 0.0008) (Table 2, Figure 4).
Discussion
Clinical course of various skin cancers differs depending on their histopathological structure and growth pattern [7, 10]. As many authors proved, to differentiate between aggressive and non-aggressive character of skin malignancies – tumours (mainly BCCs, BSC and SCCs), some immunohistochemically detected markers are predictive. Hence, they can be used in the clinical practice to forecast the behaviour of different types of cancer, and determine the patient’s treatment as well as follow-up [15, 17–22].
In this study, positivity in Bmi-1 staining was confirmed in all BCC samples. In the majority of cases it presented the highest levels, in nodular type 3–4+ it constituted 91.3%, in infiltrative 4+ – 92.3%, in nodular/infiltrative 4+ – 69.2% and 3+ – 30.8%, and in BSC 3+ – 42.8%, and 28.6% each for 2+ and 4+. Kim, who used a similar scale (from 0 to 4+), confirmed this positivity grade in Bmi-1 staining in 95% of BCCs, and level 4+ in 75%, but he did not differentiate between BCC subtypes. Whereas, he observed SCC positivity in 57.2%, of which 28.6% – 1+, 23.8% – 2+. Scores of 3+ or more were observed in 85% of BCC, 84.6% of trichoblastomas, 10.5% of actinic keratosis, and 4.8% of SCC. Thus, he also stated that similarities in BCCs and trichoblastoma resulted from follicular differentiation shared by both types [15]. Others, such as Reinisch, noticed that BCCs expressed Bmi-1 strongly and homogenously, in contrast to SCCs; Bmi-1 was expressed more heterogeneously and weakly to moderately [21]. In his study a semiquantitative assessment of expression was performed according to the following criteria: negative, weakly, moderately, and strongly positive.
Low grade positivity in CK15 staining was noted in non-aggressive as well as aggressive types of BCCs. The lowest grade – 0 was found less frequent if there was a nodular component (nodular BCC – 39.1%, nodular/infiltrative BCC – 15.4%), whereas the highest grade was seen in infiltrative BCC (84.6%), but in BSC – 42.9%. In total BCCs, low grade level 0–1+ constituted 52.1% of nodular, 46.2% – of nodular/infiltrative, 92.3% of infiltrative, and 100% of BSC. Levels 2–3+ were evidenced in nodular BCC in 47.8%, in nodular/infiltrative BCC – 53.8%, in infiltrative – 7.7%, but no positivity at these ranges was found in BSC.
Evangelista also noted in her study that the majority of BCCs stained positive for CK15. In her study staining for CK15 was scored as negative, 1 (< 25% staining), 2 (25–50% staining), 3 (50–75% staining) or 4 (> 75% staining). Among the BCC variants, infundibulocystic BCC had the highest rates of CK15 positivity – 87% (with 31% showing the intensity 3+) and negativity 0 in 13%, positivity of micronodular BCC in 83% (40% – 1+, 60% – 2+) and negativity 0 in 17%, positivity of morpheaform BCC in 78% (86% – 1+, 2–3+ – 14%) and negativity 0 in 22%. She concluded that greater intensity of CK15 expression generally favours a benign follicular lesion over a malignant one. Infundibulocystic BCC is characterized by a high percentage of CK15 positivity, which reflects the prominent follicular differentiation in this BCC subtype [23].
Kim in cases of BCCs confirmed positivity in CK15 staining in 100% (2+ – 15%, 3+ – 5%, 4+ – 80%), but in SCC positivity was observed in 61.9% (1+ – 42.9%, 2+ – 14.3% and 4+ – 4.8%). In cases of actinic keratosis positivity in CK15 was noted in 84.2% (1+ in 68.4%, 2+ in 15.8%). Trichoblastoma 3+ in 23.1%, 4+ in 76.9% [15]. However, Jih et al. reported focal CK15 positivity in 27% of BCCs, which was lower than in Kim’s study. Jih et al. also noted negative staining in SCCs, different than in Kim’s study [15, 24]. However, Abbas and Bhawan noted CK15 positivity in 30% of BCCs, and only in 5% of SCCs, which was lower than in Kim’s results [15, 25]. This heterogeneity of CK15 expression may result from different primary antibody for CK15 as well as criteria for positivity in these studies. Sabeti et al. stressed that CK15 expression strongly favours trichoepithelioma versus BCC, even those with follicular differentiation. They noted positivity for CK15 only in 4.5% in nodular BCCs, but in 66.7% in trichoepithelioma [26].
There are no literature reports dealing with immuno-expression of CK15 in various types of BCC as detailed as in our study.
We confirmed Bcl-2 positivity in all but 4 specimens included in this study (BCC nodular/infiltrative – 0). A significant relationship was found between low-grade (1–2+) positivity and aggressiveness of individual types of BCC (infiltrative, BSC, and nodular/ infiltrative). Hence, the highest positivity (3–4+) was revealed in 95% of nodular BCC of our study. Positivity in the range 0–1+ was noted in 76.9% of nodular/infiltrative BCC, 71.4% of BSC, and 38.4% of infiltrative BCC, but Bcl-2 positivity still did not exceed 2+ in those aggressive BCC types listed above. These observations are consistent with the results presented by some other authors. For example, Ramdial used a scale that is similar to ours and found high Bcl-2 positivity of 3–4+ in the nodular as well as in superficial types, 2–3+ staining in micronodular BCCs, and with pure or predominantly infiltrative component demonstrated 1–2+. He stated that regardless of derivation from primitive basaloid stem cell, as well as limited potential for metastasis, BCC are heterogeneous tumours that differ markedly in histologic and biologic behaviour. While the superficial and nodular tumours are indolent slow-growing with high Bcl-2 labelling, the aggressive ones are infiltrative, desmoplastic with low Bcl-2. In mixed tumours, heterogeneity of labelling is a distinctive feature and is contributed to in part by the labelling trends of the different histological subtypes. Micronodular type shows varied Bcl-2 labelling but in combined tumours occupies an intermediate niche between the non-aggressive nodular and superficial and the aggressive infiltrative subtypes. The initial and subsequent biopsies of recurrent, adequately excised BCCs share a pure or mixed, predominantly infiltrative, stroma-rich histopathology with low Bcl-2 labelling, reflecting the immunoprofile of a more aggressive growth pattern [27]. Whereas, Sivrikoz did not find any difference between two aggressive types of BCC – infiltrative BCC and BSC in terms of Bcl-2 expression; grading used was 1+: 0–25%, 2+: 26–50%, 3+: 51–75%, 4+: > 75% cell positivity, 1 or 2 positive staining was considered “low” and 3 or 4 positive staining “high” for both markers) [28].
We present a detailed analysis of the expression of selected markers in individual types of BCCs. So far, research has focused on the usefulness of selected immunohistochemical molecules in various types of skin lesions. Our study is complementary to the observations of other authors, differentiating and comparing the expression of markers in particular types of BCCs.
Conclusions
Positive Bmi-1 staining was the highest in the aggressive infiltrative subtype of BCCs, whereas the lowest in BSCs. Infiltrative BCC was characterized by a lower level of CK15 expression than nodular BCC and nodular/infiltrative BCC. Differentiation of Bcl-2 expression depended on the type of tumour; the highest level was found in nodular BCC, low grade in nodular/infiltrative and infiltrative BCCs, and BSC.







