
Introduction
First defined in 2005 at the Montreal World Congress of Gastroenterology, cirrhotic cardiomyopathy (CCM) is a condition of subclinical cardiac dysfunction characterized by impaired myocardial contractility, left ventricular (LV) hypertrophy, diastolic dysfunction (DD), impaired chronotropic function and electrophysiological abnormalities in the absence of other known causes of heart disease [1]. The preliminary criteria which were considered for the diagnosis of CCM are reported in Table 1. This condition has been reported to predict the development of hepatorenal syndrome (HRS) [2] and poor outcome in patients with advanced cirrhosis and in patients undergoing orthotopic liver transplantation (OLT) [3]. CCM is actually considered a condition of latent heart failure which manifests only under stress, resulting in a blunted increase in cardiac index (CI) and cardiac output (CO) during exercise or pharmacologic stimuli [1, 4], but which is barely identified at rest mainly because it is confused with other symptoms of advanced liver cirrhosis, such as exercise intolerance, fatigue and dyspnoea, and therefore its prevalence is still unclear. In the last decade 2-dimensional speckle tracking echocardiography (2DSTE) emerged as robust ultrasonic technique also validated by magnetic resonance imaging [5] allowing evaluation of the longitudinal function (deformation) of the myocardium through strain and strain rate analysis and providing information on subclinical impairment of longitudinal ventricular function [6]. The latter always precedes the depression of LV ejection fraction (LVEF) and may be a guide to the presence of fibrosis. Global longitudinal strain (GLS), a parameter derived from 2DSTE, has been reported to add incremental prognostic value, in addition to established prediction models, in the general population [6].
Table 1
Criteria for cirrhotic cardiomyopathy (CCM) as proposed at the World Congress of Gastroenterology in 2005
Hence, these advances in cardiovascular imaging, including the assessment of LV strain (longitudinal, radial and transverse), have provided new criteria to identify a subclinical cardiac dysfunction, rendering the 2005 CCM criteria obsolete. Therefore, in 2019 a position paper of a multi-disciplinary international group (Cirrhotic Cardiomyopathy Consortium) proposed new criteria to define CCM (Table 2), including advanced DD and systolic dysfunction defined as LVEF ≤ 50% or absolute GLS < 18% or > 22% [7].
Table 2
Criteria for cirrhotic cardiomyopathy (CCM) as proposed by the Cirrhotic Cardiomyopathy Consortium (2019)
At present, no information exists as regards the prevalence of CCM according to these new criteria and, more importantly, its prognostic value in cirrhotic patients. Therefore, the aim of our study is to assess the real prevalence of CCM, as defined according to the above criteria, and its prognostic relevance after long follow-up.
Material and methods
Patient selection
We retrospectively interrogated a large data set of 162 consecutive cirrhotic patients collected from 2009 to 2012, who underwent a detailed haemodynamic evaluation and standard trans-thoracic Doppler echocardiography in our clinic. Exclusion criteria were arterial hypertension, history of cardiovascular disease, diabetes, obesity, and heart valve disease. Coronary heart disease was excluded in all participants on the basis of symptoms, negative family history, a normal standard 12-lead electrocardiogram, and normal wall motion on the two-dimensional echocardiographic examination.
If taken, β-blockers were stopped 48 hours before echocardiography. The diagnosis of liver cirrhosis was based on clinical, biochemical, imaging and endoscopic findings in all patients. The presence of ascites was detected clinically and confirmed by an abdomen ultrasound examination. The diagnosis of refractory ascites was based on the criteria of the International Club of Ascites [8]. In patients with refractory ascites the haemodynamic evaluation was performed soon after the therapeutic paracentesis.
As controls, we selected 46 healthy subjects, matched for age, who voluntarily participated in this study. All patients furnished written consent to the study, which was approved by the Ethics Committee of the University of Padua, and followed the Helsinki Declaration principles.
Analysis of echocardiographic parameters
All echocardiographic examinations were performed by an expert sonographer (M.C.) using a General Electrics Vivid 7 ultrasound machine with a 2.5 MHz transducer. Measurements were performed according to the American Society of Echocardiography/European Association of Echocardiography guidelines [9]. Left ventricular EF and fractional shortening (FS) were measured in biplane two-dimensional mode using Simpson’s method [9]. Midwall fractional shortening (MWFS) was also calculated to assess underlying systolic dysfunction in the setting of concentric hypertrophy [10]. The LV mass (LVM) was estimated using the formula of Devereux et al. [9] and normalized both by body surface area (BSA) and by height in metres to the power of 2.7. Criteria for LV hypertrophy (LVH) were LVM/height ≥ 50 g/m2.7 for men and ≥ 47 g/m2.7 for women according to the current European Society of Cardiology/European Society of Hypertension (ESC/ESH) guidelines.
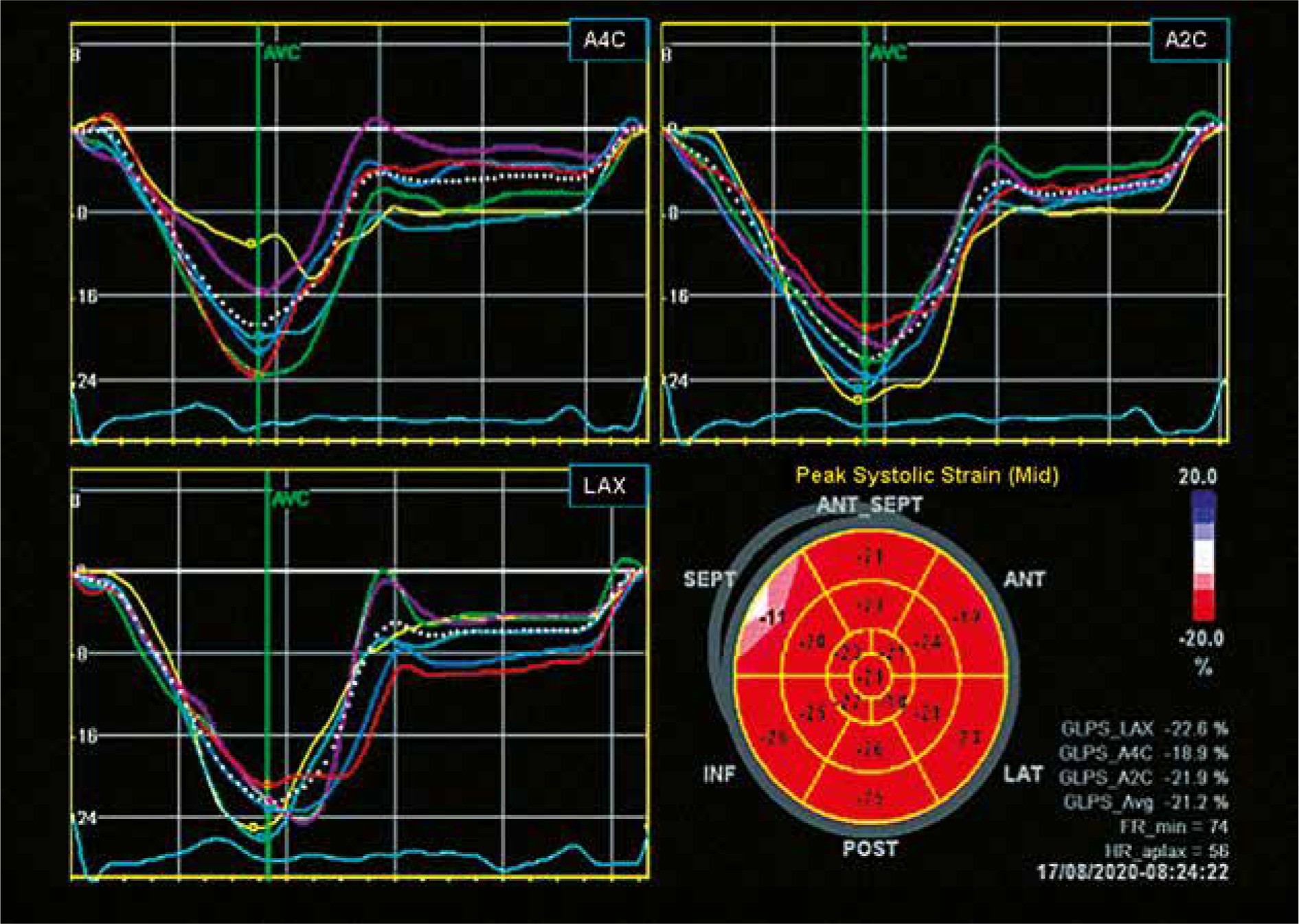
The GLS was assessed according to the European Association of Cardiovascular Imaging (EACVI) and the American Society of Echocardiography (ASE) guidelines [11]. Figure 1 shows the global longitudinal strain polar map image of a cirrhotic patient with preserved systolic function and normal GLS.
Fig. 1
Global longitudinal strain (GLS) polar map image of a cirrhotic patient with preserved systolic function and normal GLS (GLS average 21.2%)
Pulsed Doppler recordings at the level of the mitral valve tips were obtained from apical 4-chamber scans to measure early (E) and late (A) diastolic filling velocities, their ratio (E/A ratio), and the early wave deceleration time (DT) [12].
The tissue Doppler imaging (TDI) program was set to pulse-wave Doppler mode. Filters were set to exclude high frequency signals. Gains were minimized to allow a clear tissue signal with minimal background noise. The TDI of the diastolic velocities was obtained from the apical 4-chamber view positioning the recorded wall in the centre of the sector and placing a 1.5-mm sample volume at the septal corner of the mitral valve annulus. The angle between the Doppler beam and the longitudinal motion of the septal mitral valve annulus was minimized, as well. All Doppler parameters were recorded at a horizontal speed of 100 mm/s. The average values obtained for at least three consecutive cardiac cycles were taken into consideration. Early diastolic peak velocity of septal mitral annulus (septal E') was obtained and the E/e' ratio was derived [12]. Analysis of strain rate (SR) parameters was performed offline by the same operator (M.C.). Placing the region of interest on the medial corner of the mitral annulus we assessed its peak systolic tissue velocity (septal S'). Placing the region of interest (6 mm × 4 mm) on the basal portion of the inferior interventricular septum we assessed septal peak systolic strain (septal strain) and the systolic strain rate (septal SRs).
The measurement of these echocardiographic parameters was shown to be highly reproducible in our laboratory, as already reported [13, 14].
Definitions and calculation of parameters
The following parameters were calculated: mean arterial pressure (MAP) (systolic pressure + 2 × diastolic pressure/3); stroke volume (SV) was computed as the difference between end-diastolic and end-systolic LV volume and used as a direct indicator of LV volume load. Cardiac output (CO) was calculated as the product of SV and heart rate; cardiac index (CI) was calculated as CO adjusted by the BSA; systemic vascular resistance index (SVRI) was calculated as the product of MAP and 80/CI [4]; stroke work (SW), a measure of total cardiac workload, was calculated as the product of systolic blood pressure (pressure load) and SV (volume load) and converted into gram-metres per beat by multiplying by the conversion factor 0.0014 [14].
Myocardial mechano-energetic efficiency (MEE) was estimated as follows: SV (z-derived)/(heart rate × 0.6) and divided by LVM to obtain an estimate of MEE per gram of LVM (MEEi) (ml/s × g) [15].
Advanced diastolic dysfunction was diagnosed if ≥ 3 of the following criteria were met: left atrial volume index > 34 ml/m2, tricuspid regurgitation velocity > 2.8 m/s, septal e' velocity (early diastolic myocardial velocity on TDI) < 7 cm/s, E/e' (early diastolic transmitral and myocardial velocity on TDI ratio ) > 15 [7].
Statistical analysis
The data are expressed as mean ±SD (or SEM, or median and range), as appropriate. All echocardiographic and haemodynamic parameters showed a normal distribution, which was formally verified by Kolmogorov-Smirnov test. Student’s t-test or Wilcoxon rank sum test was applied to compare quantitative variables, and χ2 analysis for categorical variables. Significance was set at p < 0.05. The statistical analysis was performed using SPSS 18 for Windows (SPSS Italy Inc., Bologna, Italy).
Results
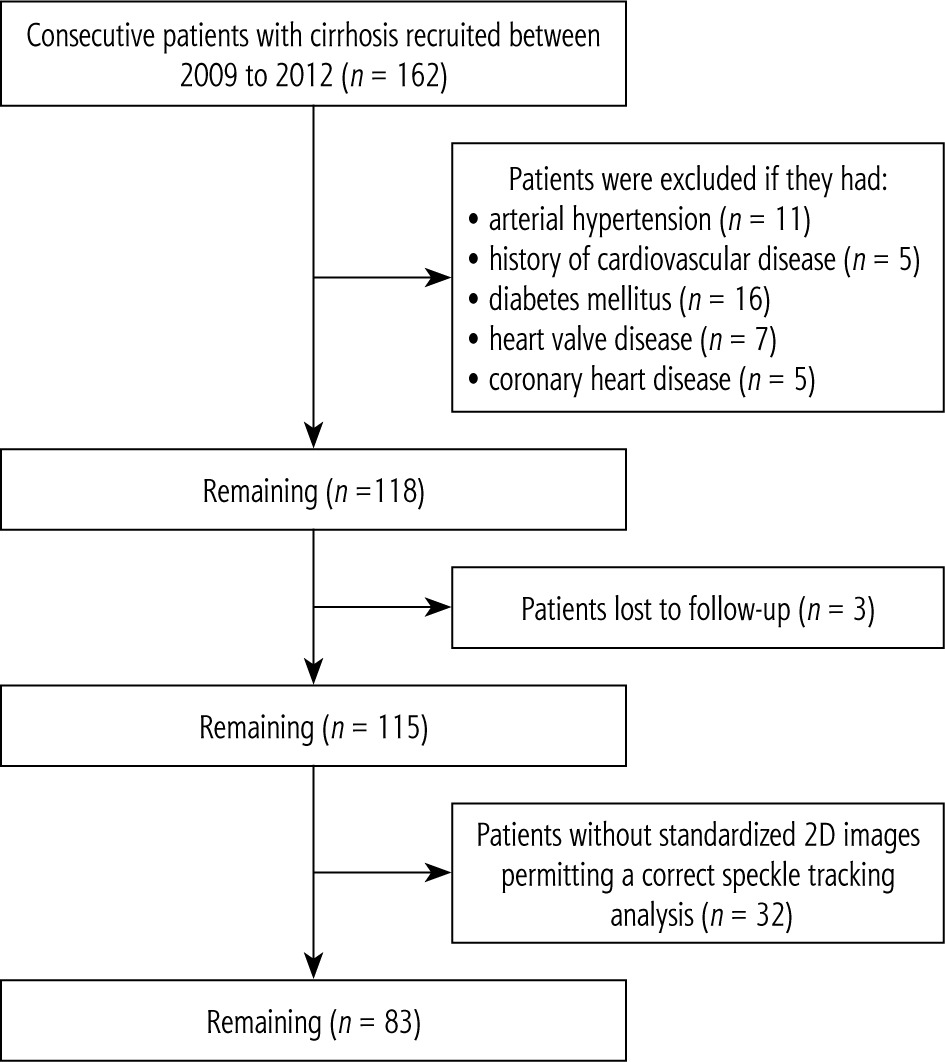
Between 2009 to 2012 we recruited 162 consecutive outpatients with cirrhosis. As shown in Figure 2, patients were excluded if they had arterial hypertension (n = 11), history of cardiovascular disease (n = 5), diabetes mellitus (n = 16), heart valve disease (n = 7), or coronary heart disease (n = 5). Three patients were lost to follow-up. Of the remaining 115 patients only in 83 were good and standardized 2D echocardiographic images available to permit correct speckle tracking analysis according to the EACVI/ASE guidelines [11].
These 83 patients were mostly males, in different stages of liver disease of different aetiology. As expected, cirrhotic patients showed a reduction of MAP and peripheral vascular resistance, and an increase of heart rate and QTc, LA dimension, LV dimension and mass, SV, SW, and CO as compared with healthy subjects (Tables 3 and 4).
Table 3
Clinical, demographic and biochemical features of cirrhotic patients with and without cirrhotic cardiomyopathy (CCM)
Table 4
Haemodynamic and echocardiographic features of cirrhotic patients with and without cirrhotic cardiomyopathy (CCM)
[i] The data are reported as mean ±SD. CO – cardiac output, DT/HR – deceleration time of the E wave/heart rate, GLS – global longitudinal strain, E/A – early and late diastolic velocity ratio, LA – left atrium, LVEDVol – left ventricular end-diastolic volume, LVM – left ventricular mass, MEEi – myocardial mechano-energetic efficiency indexed for LVM, MWFS – midwall fractional shortening, SV – stroke volume, SW – stroke work.
Diagnosis and prevalence of cirrhotic cardiomyopathy
As regards the systolic dysfunction, no patient presented LVEF ≤ 50%. A GLS < 18% or > 22% was evident in 21 patients (25%) independently of aetiology of cirrhosis or the presence/absence of ascites. As regards the parameters used to define diastolic function, an increased LA volume (> 34 ml/m2) was evident in 26 patients (31%); tricuspid regurgitation velocity > 2.8 m/s was evident in 10 patients (12%), septal e' velocity < 7 cm/s was evident in 15 patients (18%), E/e' > 15 was evident in 9 patients (11%). Considering together the above parameters, advanced diastolic dysfunction was evident in 8 patients (10%).
Overall, the prevalence of CCM defined according to all the above parameters was 29%.
Comparison of patients with and without cirrhotic cardiomyopathy
Tables 3 and 4 present the main clinical, biochemical, haemodynamic and echocardiographic parameters of cirrhotic patients divided according to the presence or absence of CCM. No significant differences emerged between the two groups. In particular, no differences were found as regards cardiac dimensions, subclinical systolic dysfunction (MWFS and GLS), cardiac work (SV, SW and CO), and myocardial mechano-energetic efficiency (MEEi). Moreover, other accepted indexes of diastolic function (E/e', E/A, DT/HR) were found to be similar in patients with and without CCM.
Survival according to the diagnosis of cirrhotic cardiomyopathy
Among the 83 patients considered in this study, during a median follow-up of 6 years (range: 20 days- 7 years) 30 patients died (36%) and 5 patients developed type 1 HRS. Main causes of death were complications of cirrhosis (gastrointestinal haemorrhages, hepatorenal syndrome, liver failure, sepsis, hepatocellular carcinoma). Patients with and without CCM presented similar incidence of death after 6 years of follow-up. Of the 5 patients who developed HRS only 1 presented CCM (Table 3). In a sub-analysis we considered only the 47 patients with cirrhosis and ascites who were on the list for liver transplantation. Of them, 17 presented CCM and 30 did not. The mortality rates in the two groups were 41% in patients with CCM and 43% in patients without CCM (NS). Paradoxically, the 17 patients on the transplant list with CCM presented a lower incidence of HRS as compared with patients without CCM (6% vs. 13%, respectively) during the follow-up.
Discussion
Cardiac complications are common after orthotopic liver transplantation (OLT), ranging from 7% to 70%, and lead to considerable mortality and morbidity [3].
Perioperative and postoperative heart failure with reduced left ventricular ejection fraction (HFrEF) has been observed in 3% to 14% patients [16, 17] despite the majority of them presenting normal LV function before OLT, since patients with overt systolic dysfunction are often declined for OLT.
In a single-centre cohort of 176 consecutive patients who underwent OLT, post-OLT HFrEF (defined as EF ≤ 40% with acute heart failure symptoms) was present in 14% with a median of 5 days and was associated with a 7-fold increase in 1-year mortality [17].
Cirrhotic cardiomyopathy is considered an important risk factor for early post-transplant HFrEF [17, 18] since it may manifest with unexpected and often severe LV systolic and diastolic dysfunction, sometimes rapidly arising after transplant when the redistribution of significant blood volumes leads to marked right and LV volume overload, and a contemporary increase in afterload due to the rapid postoperative reversion of systemic vasodilation. Hence, the pre-LT diagnosis of CCM is fundamental to identify patients at higher risk of developing perioperative and postoperative HFrEF.
The newly proposed criteria to define CCM consider both subclinical systolic dysfunction and advanced diastolic dysfunction.
As regards the systolic dysfunction, since in our cohort of cirrhotic patients in different stages of liver disease none presented a LVEF < 50% it is clear that a low LVEF is not a useful criterion to define CCM and should not be considered in the guidelines. At variance, altered GLS (as defined if < 18% or > 22%) was evident in 25% independently of aetiology of cirrhosis or the presence/absence of ascites. However, after a 6-year follow-up the percentage of patients who died was similar in patients with and without altered GLS or advanced diastolic dysfunction at baseline (i.e. with and without CCM so defined), thus suggesting a poor relevance of this classification in terms of prognosis, at least in cirrhotic patients. It should be noted that the evidence of an altered GLS at rest in cirrhotic patients is limited and conflicting. Some studies showed normal longitudinal strain when compared with controls [19, 20], while others reporting a reduced longitudinal strain compared with controls but without a difference between compensated vs decompensated patients (i.e. between Child-Pugh A, B, and C grade cirrhosis) [21-23] or an increased GLS at rest (i.e. higher LV contractility) in more advanced liver disease (Child-Pugh C) correlating with a worse prognosis [24, 25]. In the newly proposed classification a GLS < 18% and > 22% has been considered diagnostic of CCM [7].
As regards the diastolic dysfunction, we previously reported that DD, as defined according to both previous (ASE 2009) [12] and current guidelines (ASE/EACVI 2016) [26], does not correlate with poor prognosis in a large cohort of cirrhotic patients followed for 6 years [14, 27]. This is in line with the results of other groups [23, 28, 29] which observed an independent predictive value of left atrial dimension [29] or E/e' [28] but not of the above definitions of DD proposed by current guidelines [26]. Moreover, the prevalence of DD according to the algorithms below demonstrated a wide variability independently of the severity of liver disease [30], probably because none of these algorithms was developed in patients with cirrhosis, but they have been validated in patients with symptomatic cardiovascular diseases, aiming at identifying increased cardiac filling pressures, a condition which is probably uncommon in asymptomatic cirrhotic patients with normal LVEF and with central hypovolemia.
Conclusions
In conclusion, we believe that the recently proposed new criteria to define CCM, predominantly based on altered GLS at rest, are mainly descriptive, with poor relevance in terms of prognosis and useless for the clinical management of cirrhotic patients, particularly in pre-transplant evaluation.
Moreover, this classification does not permit to clarify whether CCM represents a disease per se or a symptom of cirrhosis. If the aim is to identify a pathophysiological condition, i.e. subclinical cardiac dysfunction, which could affect the outcome during/after OLT, we believe that a stress test (such as a stress-echocardiography with low-dose dobutamine) assessing not the presence/absence of inducible ischaemia (i.e. coronary artery disease detection) but the cardiac contractile reserve could allow one to distinguish patients with a blunted cardiac response (i.e. with CCM) who could be at higher risk of new-onset HF. Hence, we suggest modifying the proposed new criteria by removing the assessment of LVEF and adding stress echocardiography assessing the cardiac contractile reserve. Further research in this field is required to better clarify which is the best stress test to assess the cardiac contractile reserve and the predictive value of a blunted cardiac response to stress for the development of perioperative and postoperative HFrEF.
Limitations and strengths
We recognize that a single-centre, retrospective design could limit the robustness of the findings. Strengths of this study to be underscored include the long follow-up and the large sample size of phenotypically well-characterized cirrhotic patients; the use of state-of-the art echo-Doppler techniques entailing TDI and speckle tracking analysis; and the fact that all of the echocardiograms were performed by a single experienced cardiologist.





