
INTRODUCTION
Morphea, also referred to as localized scleroderma, is a chronic inflammatory disorder of the skin characterized by excessive collagen deposition, resulting in progressive dermal thickening and sclerosis. It primarily affects the skin and subcutaneous tissues, but in more extensive cases may involve deeper structures such as fascia, muscle, or even bone. Current classifications describe five major subtypes: localized, generalized, linear, deep, and mixed forms [1, 2].
The clinical manifestations vary according to the depth and extent of tissue involvement and disease activity [3]. Unlike systemic sclerosis, morphea typically does not involve Raynaud’s phenomenon, disease-specific autoantibodies, or internal organs [4]. The diagnosis is predominantly clinical, relying on the identification of localized well-demarkated foci of skin sclerosis [5, 6]. Exclusion of other conditions that may mimic this clinical presentation is essential [2].
In this report, we describe a 54-year-old woman with a long-standing history of en coup de sabre morphea (ECDS) and progressive facial hemiatrophy (PFH). In addition to frontotemporal atrophy, the patient demonstrated ocular involvement, raising the possibility of a potential link to the underlying disease. This case highlights the importance of multidisciplinary assessment in atypical clinical presentations.
CASE REPORT
A 54-year-old woman was admitted to our dermatology ward with ECDS, with coexisting features of PFH. She had a long-standing history of linear morphea diagnosed 20 years earlier, previously stable without systemic therapy. Over the past year, she reported increasing atrophy of the right cheek and eyebrow, along with intermittent headaches and visual disturbances.
Her medical history included iron-deficiency anemia, hypertriglyceridemia, and chronic right knee pain under rheumatologic evaluation. Family history included rheumatoid arthritis in her father.
On physical examination, the patient exhibited maxillomandibular asymmetry and enophthalmia with overlying brownish skin discoloration, and alopecia on the right scalp, consistent with ECDS. Additionally, she presented with a pterygium in the right eye, hemiatrophy of the right side of the tongue, and a sclerotic plaque on the left side of the neck (Figure 1). Moreover, eyelid atrophy was present.
Figure 1
Clinical presentation of a 54-yo woman with en coup de sabre morphea and progressive facial hemiatrophy of her right site

Brain magnetic resonance imaging (MRI) demonstrated thinning of the right frontal bone and multiple chronic ischemic lesions in the right cerebral hemisphere, with glial scarring near the temporal horn.
Given the newly observed disease progression, she began treatment with intravenous corticosteroid pulses and was qualified for systemic immunosuppressive treatment with methotrexate. Due to the ocular findings and suspected morphea-related involvement, an ophthalmologic consultation was arranged.
The optometric examination revealed full best-corrected visual acuity. Intraocular pressure in both eyes was within normal limits. We did not observe lagophthalmos.
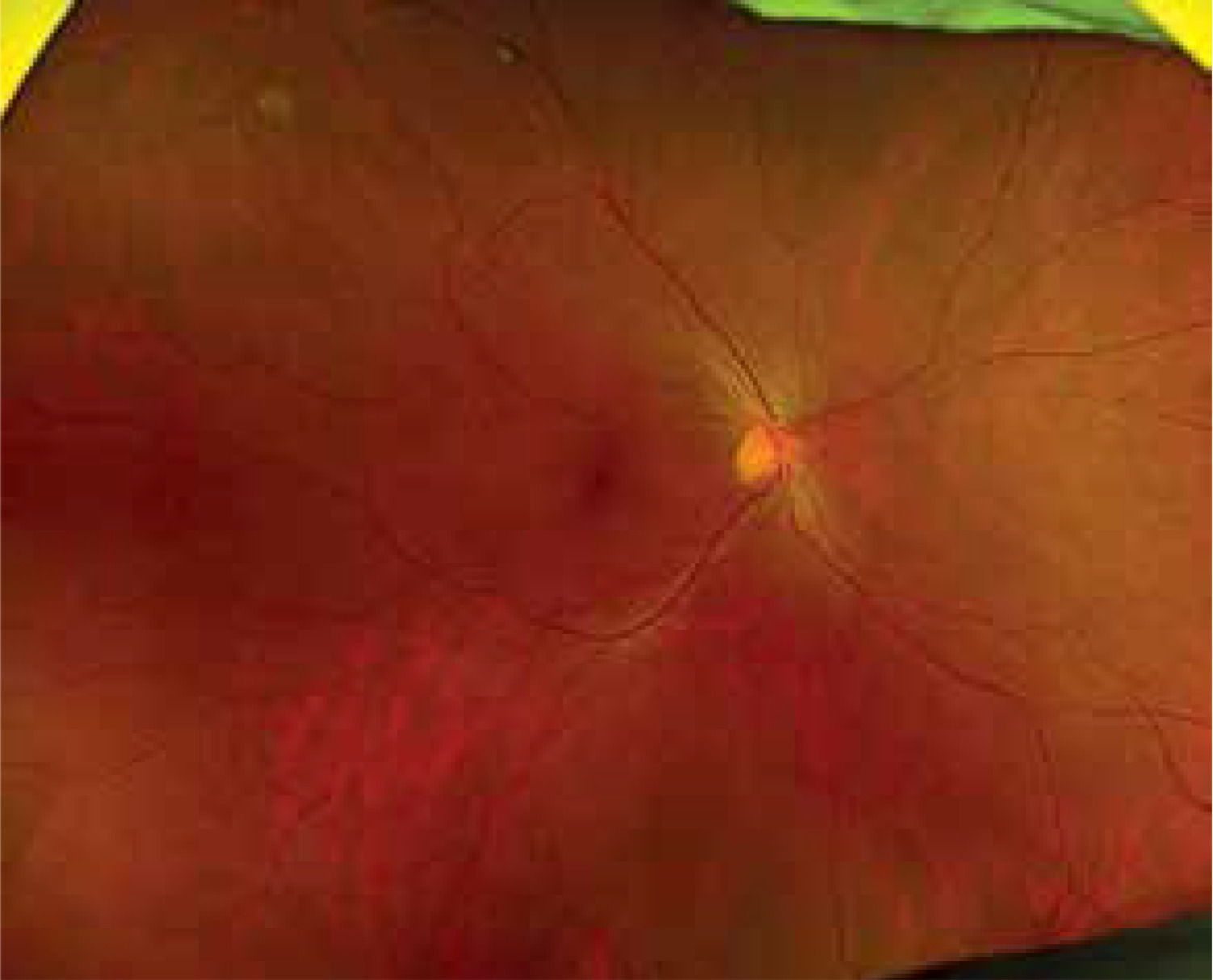
Anterior segment assessment of the right eye demonstrated a nasal pterygium not extending into the visual axis (Figure 2). No other anterior segment abnormalities were observed. No synechiae were present in either eye. Posterior segment evaluation of the right eye revealed a small, well demarcated, retinal pigment epithelium atrophy located near the superior temporal vascular arcade in the middle periphery (Figure 3). No additional abnormalities of the posterior segment were noted. Optical coherence tomography (OCT) showed no pathological findings. Macular morphology was preserved in both eyes, and the retinal nerve fiber layer (RNFL) and ganglion cell complex (GCC) thickness values were within normal limits bilaterally.

DISCUSSION
ECDS is a term used to describe linear morphea involving the forehead and scalp. It typically manifests as a linear, indurated depression on the forehead and scalp, aligned with the lines of Blaschko and reflecting underlying localized sclerosis [7]. While ECDS is usually confined to the frontoparietal region, some case reports describe broader tissue involvement, with atrophy extending into adjacent facial structures such as the eyelids and periorbital area [8]. In some cases, ECDS may coexist with PFH, with an estimated overlap in 20–40% of patients, including our case [9].
PFH, also known as Parry-Romberg syndrome, is often considered a severe variant within the spectrum of linear morphea, although it may represent a distinct clinical entity. It typically involves progressive atrophy of subcutaneous fat with minimal or absent skin sclerosis. The disease may involve areas innervated by the trigeminal nerve, including ocular and oral structures [1, 2]. Ocular involvement is observed in approximately 15% of patients with PFH [2].
Linear morphea may affect a wide range of ophthalmic structures, with manifestations described in both ECDS and PFH. Enophthalmos is the most commonly reported periorbital manifestation. Among the most frequently described ocular findings are keratopathy, uveitis and episcleritis. Optic neuropathy, including optic neuritis, has also been documented in the literature [10, 11].
However, the pathogenesis of morphea is still not fully understood. The literature highlights a multifactorial etiology involving genetic, epigenetic, and environmental triggers, such as trauma, infections, or drugs [12]. A recent study revealed that the epidermis in morphea showed a highly proliferative and inflammatory transcriptomic profile, with overexpression of the p53 signaling pathway [13]. This may contribute to aberrant keratinocyte proliferation, apoptosis regulation and fibrotic responses.
Similarly, pterygium is a fibrovascular degenerative lesion of the conjunctiva with an incompletely understood pathogenesis. Studies show increased expression of p53 and Mouse Double Minute 2 (MDM2) proteins in pterygium [14, 15]. Over time, it may invade the cornea and affect visual acuity. Risk factors include ultraviolet light exposure, aging, and male gender, with common symptoms such as redness, irritation, dryness, and tearing [16]. Pterygium fleshiness is correlated with stromal fibrosis [17]. In our patient, stromal fibrosis was classified as stage T2, which may indicate a shared underlying fibrotic mechanism.
This case emphasizes the necessity of considering atypical ocular involvement when evaluating patients with morphea. The literature offers limited evidence linking the occurrence of pterygium as an ophthalmic manifestation to morphea. However, since pterygium is associated with fibrosis – a hallmark feature of morphea – a causal relationship between these conditions cannot be excluded.
To confirm this potential association, further investigation is required.










