








Introduction
Ultraviolet radiation (UVR) is electromagnetic radiation emitted by the sun, consisting of three wavelength ranges: UVC (200-290 nm), UVB (290-320 nm), and UVA (320-400 nm). In Poland, UVB rays are mainly present from spring to autumn, with the highest intensity around midday. On the other hand, UVA radiation occurs throughout the year, maintaining a consistent level during the day and having the ability to penetrate through window glass, unlike UVB.
UV radiation has proven effects on human health, both positive and negative. It is responsible for the synthesis of vitamin D in the skin, which has a significant impact on health, supporting the maintenance of healthy bones and positively affecting immunity. Excessive exposure to ultraviolet radiation can result in skin burns, accelerated skin aging, and the development of pre-cancerous and cancerous changes. The use of proper sun protection is crucial to prevent the negative effects of UV radiation on the human body, especially for individuals using photosensitizing medications and those with subacute cutaneous lupus erythematosus, photodermatoses, and skin cancer risk factors. Regular use of UV protective preparations with sunscreen inhibits the development of actinic keratosis, a precancerous condition, reduces the risk of melanoma and squamous cell carcinoma, and also delays skin photoaging [1-5].
The use of sun-protective substances in cosmetics is regulated by the European Parliament and Council Regulation (EC) No 1223/2009 of November 30, 2009, regarding cosmetic products. UV filter regulations stipulate that for a product to be classified as effective in sun protection, it must protect against both UVB and UVA [6]. The effectiveness of cosmetic products protecting against UVB radiation is indicated by the standardized international Sun Protection Factor (SPF) index. This index represents the ratio of the minimal erythema dose (MED) causing redness on skin protected by a given product to the MED causing redness on unprotected skin [7].
According to the guidelines of the Polish Dermatological Society, it is recommended to use sunscreen products with an SPF of 30 or higher in spring and summer and an SPF of 15 or higher in autumn and winter [8]. To ensure proper protection and achieve the specified SPF, sunscreen should be applied at a rate of 2 mg/cm2 of skin and reapplied no less than every 2 hours [9].
Clinical studies refute the idea that the use of sunscreen negatively affects vitamin D synthesis in the skin [10,11]. The Polish Dermatological Society does not recommend prolonging sun exposure to enhance vitamin D synthesis due to the negative impact of UV radiation on health. In cases of vitamin D deficiency, oral supplementation is recommended, especially for the pediatric population, to avoid excessive sun exposure and sunburn, which increases the risk of melanoma in the future [12,13].
Eye protection is also crucial, and the regular use of suitable sunglasses that absorb ultraviolet waves up to 400 nm and have European certification can reduce the incidence of cataracts [14,15].
Sun protection applies to individuals of all ages, especially children up to the age of 14, immunocompetent individuals, and those with fair skin. From a public health perspective, educating the population on photoprotection is essential to reduce the risk associated with excessive exposure to sunlight.
Aim of the work
The aim of the study was to assess the use of sunscreen and other sun protection practices among the residents of the Silesian Voivodeship, Poland, as well as to determine the reasons behind the protective actions taken by the residents.
Material and methods
The study was conducted among residents of the Silesian Voivodeship. A total of 417 questionnaires were distributed, out of which 400 (96%) were correctly filled out and included in further analysis. Among them were surveys completed by 243 females and 157 males, ranging in age from 16 to 84 years (mean age = 34.38±18.39). The inclusion criteria for the study included individuals aged 16 and above residing within the territory of the Silesian Voivodeship, who, with their own consent (or parental consent for minors), expressed willingness to participate.
An original questionnaire was used in the study, and its completion was anonymous and voluntary. Participants were asked about general information (age, gender, place of residence, employment and/or education) and factors related to the risk of developing melanoma and its prevention. The survey also included questions about the involvement of primary health care physicians in the diagnosis and preventive actions against melanoma. The questionnaire included both single-choice and multiple-choice questions and also allowed for respondents to provide their own answers. In the analysis of results, the data related to multiple-choice questions were detailed. To avoid favoring answers appearing at the beginning, the order of responses in each survey was randomized.
Paper questionnaires were distributed, with the consent of students, their parents, teachers, and directors, in primary schools, higher education institutions, workplaces, and nursing homes (with the consent of the participants and facility managers) within the Silesian Voivodeship. In the event a question is misunderstood, the researchers provided additional explanations to help participants better understand their content. Completed questionnaires were stored in a special folder in a locked drawer and were only taken out during data entry into a spreadsheet. Consequently, the identification of respondents was not possible, ensuring their complete anonymity.
All methods employed in the research were carried out in accordance with the relevant guidelines and regulations. The data was collected and organized in Microsoft Excel, and then analyzed using basic statistics in Statistica 13.3. The analyzed results were presented in numerical and percentage values. In Table 2 and 5, the percentage values also refer to the created subgroups. In Table 2, participants were divided into 3 age groups (16-25, 26-65, >65 years) for analysis purposes. The results were categorized according to gender, age, place of residence, and education. A Chi-squared test was used to examine the relationship between the mentioned factors and the use of UV filter products. Additionally, using the Chi-squared test, it was investigated which groups of participants, depending on gender and age (16-25, >25 years), exhibited exceptional conscientiousness in using sunscreen creams. The criterion was daily use of SPF > 50 on the face. The obtained results were presented in Table 5. The null hypothesis negated the existence of a relationship between variables. The critical level of significance was set at p<0.05.
Results
General characteristics of the studied group
The overall characteristics of the studied group, including gender, age, place of residence, and education, are presented in Table 1.
Table 1.
General characteristic of the studied group
The majority of the study group consisted of women and individuals below the age of 50, predominantly residing in rural areas. People with higher and secondary education accounted for over 70% of all respondents.
Use of sunscreen in the study group
Figure 1 presents percentage figures for study group subjects who do use sunscreen and those who do not use sunscreen. In Table 2, the above-mentioned data are presented based on gender, education, place of residence and age.
Table 2.
Characteristics of the study group according to the use of sunscreen based on gender, education, place of residence and age
Unfortunately, 58 (14.5%) of the participants did not use sunscreen. Among men, as many as 41 (26.11%) did not use it, while only 17 women (7%) neglected to use it. In the group of individuals with vocational education, 10 (66.67%) did not use sunscreen, and for those with higher education, only 7 (5.15%) did not use it. In the population of people living in rural areas, 37 (17.79%) respondents did not use sunscreen, while in cities 21 (10.94%) neglected to use it. For the presented results, the p-value based on gender, education and age was less than 5%, indicating statistical significance, while for place of residence, it was slightly above the established threshold (p=052).
Values of the SPF in sunscreen used by the respondents
The characteristics of the study group, taking into account the SPF values of the sunscreen used, are presented in Figure 2.
Figure 2
The characteristics of the study group with respect to the SPF values of the sunscreen used (multiple choices possible)
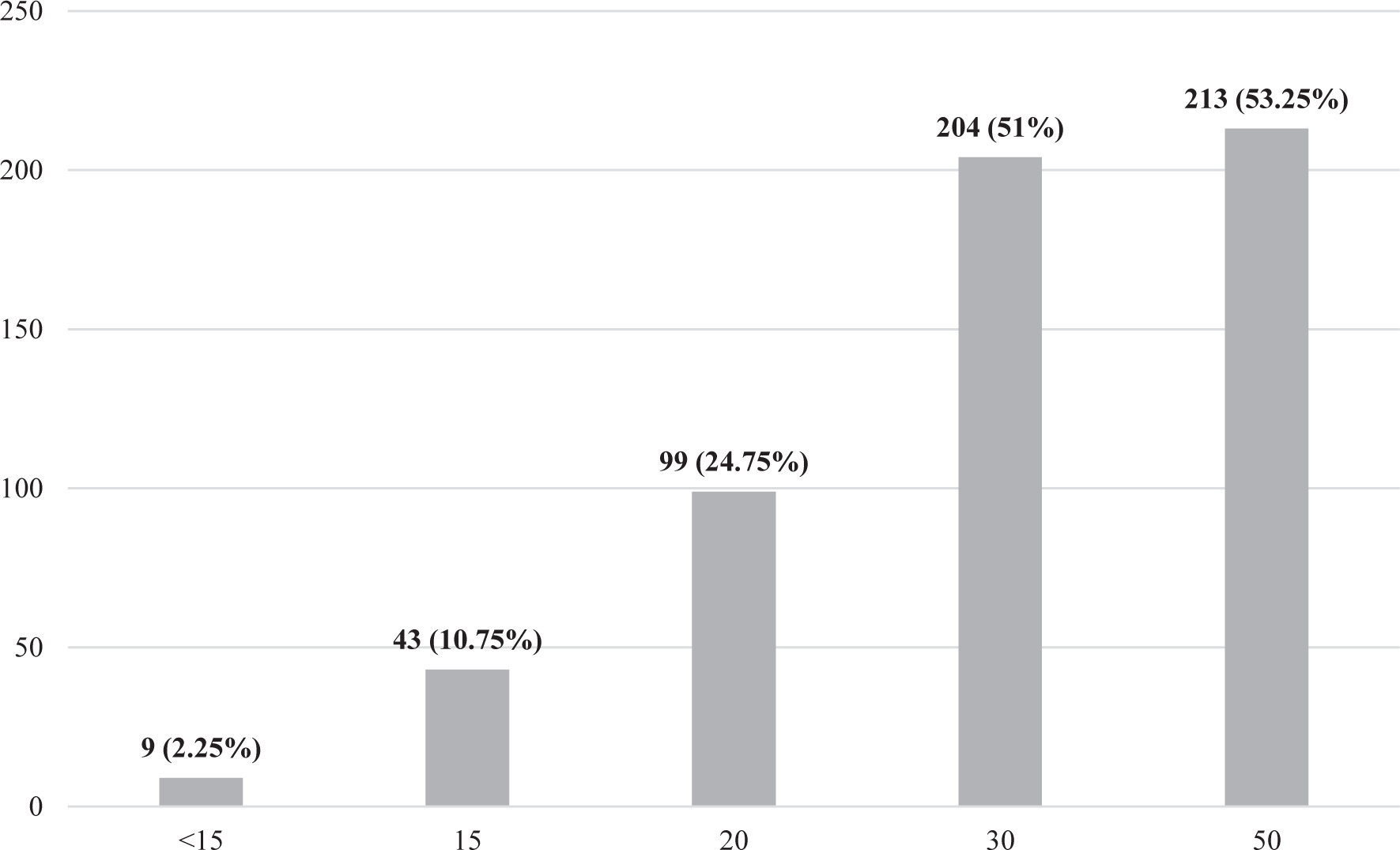
The respondents most commonly used sunscreen with an SPF of 50 (213; 53.25%) and SPF 30 (204; 51%).
Practices of the respondents related to the application of sunscreen
In Table 3, the behaviors of the respondents associated with the use of sunscreen are presented, while Table 4 shows the body parts to which respondents applied sunscreen cream depending on the situation. Table 5 contains information about the characteristics of individuals using SPF 50 sunscreen daily, applying it to their faces, and Table 6 presents the SPF values of sunscreen used by respondents based on weather conditions.
Table 3.
The characteristics of the study group with respect to behaviors associated with the use of sunscreen (multiple choices possible)
Table 4.
The characteristics of the study group, considering the body parts to which sunscreen are applied based on the situation
Table 5.
The characteristics of the study group, considering the daily use of SPF 50 UV filters on the face
Table 6.
The characteristics of the study group, considering the Sun Protection Factor (SPF) of the applied UV filter based on weather conditions
141 (35.25%) respondents did not reapply sunscreen after applying it once. A whopping 358 people (89.5%) did not apply the recommended amount of sunscreen, and over 225 (56.25%) did not reapply sunscreen after coming out of the water. In various situations, participants most frequently applied sunscreen to their face, with only 94 (23.5%) doing so daily. As many as 122 (28%) respondents did not apply UV filter-containing products to their ears and the tops of their feet. Respondents rarely applied sunscreen to their hands; only 33 (8.25%) did so on sunny days. Similarly, sunscreen was rarely applied to the lower limbs (26; 6.5%), back (22; 5.5%), abdomen, and chest (16; 4%) on sunny days. Daily use of SPF 50 sunscreen was most common in the group of women (71; 29.22%) and individuals aged 16 to 25 (53; 27.46%).
In the group of women aged 16 to 25, as many as 47 (36.72%) applied sunscreen with SPF 50 to their faces daily, making this group exceptionally diligent in terms of photoprotection. For the presented results, the p-value based on gender (p<0.0001) and age (p=0.00018) was less than 5%, indicating statistical significance. A significant 184 (46%) respondents would use sunscreen with an SPF lower than the recommended minimum of 30 or would not use it at all on a hot summer morning. The majority of respondents (216; 54%) would not use sunscreen on a cloudy August day.
Other sun protection methods used by the respondents
The characteristics of the study group considering sun protection measures other than sunscreen are presented in Table 7.
Table 7.
The characteristics of the study group, considering sun protection measures other than sunscreen (multiple choices possible)
The respondents most commonly (329; 82.25%) used sunglasses as a sun protection method other than sunscreen. However, only half of them (204; 51%) used recommended glasses featuring UV filter. Unfortunately, 57 (14.25%) respondents still regarded oiling the skin as a sun protection measure.
Reasons for using or not using sun protection
The reasons for which the respondents used or did not use sun protection measures are presented in Table 8.
Table 8.
The characteristics of the study group according to the reasons indicated by the respondents for using or not using sun protection measures (multiple choices possible)
The most common reasons indicated by the respondents for using sun protection measures were: the desire to avoid sunburn (289; 72.25%), prevention against aging (191; 47.75%), and preventing the development of melanoma (145; 36.25%). For 61 (15.25%) respondents, the reason for not always using sun protection was the fear of vitamin D deficiency, and 118 (29.5%) occasionally did not use photoprotection because they wanted to get a tan. Sun protection was skipped by 36 (9%) respondents due to its inconvenience and by 17 (4.25%) respondents due to a lack of knowledge about its importance for health. Fortunately, only one person had the misconception that UV filter is harmful.
Discussion
Most of the surveyed group (342; 85.5%) declared the use of sunscreen. Women, individuals with higher education, and people living in cities used them most frequently. Similar results were obtained by Parker et al.; their research indicated that individuals with higher education more frequently declared the use of sunscreen [16]. Studies conducted in Italy also demonstrated a correlation between female gender and more frequent use of sunscreen creams [17]. Other data also highlight the issue of less frequent use of sun protection among men and individuals with lower education levels [18,19]. It is important to ensure equal access to health-related information in society, including information about risk factors and prevention of diseases, such as the discussed impact of sun protection in reducing the risk of malignant skin tumors. Introducing education on disease prevention at earlier stages of education is crucial to ensuring equal access to health knowledge among individuals with different levels of education.
The surveyed individuals most frequently used sunscreen with SPF 50 (213; 53.25%) and SPF 30 (204; 51%). In comparison with other studies, residents of the Silesian Voivodeship more often chose sunscreen with higher SPF values. In a study conducted by Sultan et al., 40% of respondents declared using sunscreen with SPF greater than 30, while Othman Bahakim et al. showed that only 8% of respondents used a cream with SPF >30 [20,21]. In studies conducted in Saudi Arabia, SPF 50 was the most commonly used value among sunscreen product users (35.1%) [22]. These differences may arise from variations in skin types. Poles most commonly exhibit Skin Phototypes I and II, whereas Arabs exhibit Skin Phototypes IV and V, which are less sensitive to sunburn. According to scientific data and the consensus of the Polish Dermatological Society, for a sunscreen to have a specified SPF value, it must be applied in the recommended amount of 2 mg/cm2 of skin and should be reapplied after 2 hours [9]. There is another, simpler method. Based on the so-called teaspoon rule, one teaspoon of sunscreen (approximately 5 ml) should be applied to the face, head, and neck, one teaspoon to each upper arm and forearm, two teaspoons to the trunk (front and back), and two teaspoons to each leg. Although the surveyed residents of the Silesian Voivodeship primarily used products with a high SPF value, they did not always apply them correctly.
In studies conducted among healthcare workers, understood to be individuals with greater knowledge of the impact of sunlight on health, it was shown that 27% of respondents applied sunscreen every 2 hours as recommended [23]. However, in our study, this percentage was nearly half of that figure. In contrast, less than 5% of Australian farmers reapplied sunscreen every 2 hours despite working in intense sunlight exposure [24]. Over 63% of students in Saudi Arabia applied sunscreen only once, and only 6.7% reapplied it after 2 hours [22]. Australians, more often than residents of Silesia, applied the recommended amount of sunscreen, although only 15% of respondents did so [25]. Although the geographical location and associated intensity of UV radiation may influence the aforementioned differences, the knowledge of Poles regarding the proper use of sunscreen is still insufficient. This results in a lower quality of protection against sunburns and skin cancers.
Participants in our study most frequently used sunscreen on their faces, similar to findings from studies conducted by Boyas et al. [26], as well as surveys conducted among students [21,22]. However, areas cited as being commonly neglected by participants in our study were the back and lower limbs. The most common location for melanoma in men is the skin on the back, and in women, it is the lower limbs [27]. Considering these facts and the results of our study and other analyses, one can infer that frequently-occurring cases of melanoma may result from inadequate use of sunscreen on these less-protected parts of the body. This raises the question of whether the frequency of melanoma occurrence results from neglecting the use of sun protection on these body parts.
In a study conducted by Heckman et al., sunscreen was more frequently used by female students [28]. Our research likewise showed that daily use of sunscreen with SPF 50 was most common among women and individuals aged 16 to 25. Women aged 16 to 25 stood out for their exceptional conscientiousness in using UV filter. This may be related to the popularization of skincare and UV filter content on social media [29]. Similar conclusions can be drawn from a study conducted among Thai youth. Adolescent girls and high school students demonstrated more knowledge and practice in photoprotection compared to adolescent boys. Among teenage girls, 58% used sunscreen compared to 42% of teenage boys. The main sources of skincare information for teenagers were social media (77.5%), with YouTube accounting for 52% and Instagram nearly 37% [30]. In a study by Basch et al., Instagram posts about skin cancer were analyzed. Overall, the content focused on prevention (33.3%), skin cancer treatment (29.3%), and preventive measures such as the use of sunscreen (29.3%) [31]. Considering the popularity and reach of Instagram among youth and young adults, it can be inferred that it is a common source of information and could be used for health promotion by appropriately qualified individuals.
More than half of the respondents (216; 54%) would not use sunscreen on a cloudy summer day and only 154 (38.5%) would use SPF 15 or higher in winter. In studies conducted among Brazilian students, the use of sunscreen on cloudy days and in winter was considered irrelevant by 2.7% and 4.9%, respectively [32]. On the other hand, 67.7% of students surveyed in Saudi Arabia believed that using sunscreen on cloudy days is not necessary [22]. Participants in a study from China claimed to use sunscreen in winter (36%) and when indoors [18].
Although compared to the studied groups from countries with higher solar radiation intensity, Silesians did not perform the worst, the sun protection practices reported by the respondents still deviated from national recommendations. According to the guidelines of the Polish Dermatological Society, it is recommended to use products with SPF ≥30 in spring and summer, and ≥15 in autumn-winter [8]. A small percentage of respondents adhere to these recommendations. It is crucial to include this information in campaigns promoting sun protection to ensure widespread awareness.
In both our study and other studies, it has been shown that sunglasses were the most frequently chosen method of sun protection (alongside sunscreen) [21, 22, 33]. Additionally, staying in the shade and wearing protective clothing were commonly reported methods of sun protection [21,22]. These data are satisfactory, because the fundamental and inseparable recommendations for photoprotection according to the Polish Dermatological Society include avoiding excessive exposure to UVR, using protective clothing, including appropriate headgear and sunglasses, as well as the correct application of products containing UVA/UVB filters [8].
The most common reasons for using sun protection, as indicated by the respondents, were the desire to avoid sunburn, prevention of aging, and preventing the development of melanoma. Similar reasons were reported by participants in other studies. In an analysis conducted by Agarwal et al., 65% of respondents used sun protection to avoid sunburn, 34% to delay the aging process, and 29% to protect against skin cancer [34]. Healthcare workers listed protection against skin cancer ahead of skin aging as a reason for using sun protection [23]. For non-medical communities, prevention against photoaging was more important than prevention against UV radiation-induced carcinogenesis. As evident from the discussed study, residents of Silesia had knowledge that sun exposure increases the risk of skin cancer, and for this reason, more than one-third of the respondents declared using sun protection. However, nearly half valued the aesthetic aspect of taking this action, specifically the slowing down of the skin aging process. This raises the question of whether content from the field of aesthetic medicine, cosmetology, and those closely related to beauty and human physicality reaches a broader audience than content related to public health and the extension of life length and quality. Therefore, healthcare representatives should consider how to expand their reach in disseminating knowledge about health and disease prevention, including skin cancers.
The reason why 61 (15.25%) respondents occasionally did not use sun protection was the fear of vitamin D deficiency. The issue of the myth concerning vitamin D deficiency as a result of sun protection was less pronounced in studies conducted abroad compared to the study of the residents of Silesia. In Australia, only 3% of respondents reported lack of sun protection due to the belief that sunscreens could cause vitamin D deficiency [25]. In Saudi Arabia, 70.9% of respondents agreed that sunscreens do not adversely affect vitamin D levels in the body [22]. Clinical studies refute the idea that using sunscreens has a negative impact on vitamin D synthesis in the skin [10,11]. Therefore, there is no scientific justification to use this reason to neglect the use of protection against the sun. Moreover, in cases of vitamin D deficiency, supplementation is recommended rather than prolonging exposure to sunlight. In our geographical region, oral vitamin D supplementation is recommended during the autumn and winter due to the deficiency of UVB rays responsible for its synthesis in the skin during these two seasons.
36 (9%) respondents discontinued sun protection due to inconvenience, and 17 (4.25%) did so because of a lack of knowledge about its significance for health. Among Brazilian students, the primary reason for not using UV protection was laziness, indicated by 48.7% of participants [32]. In contrast, among Australian farmers, the most common barriers to sun protection were forgetfulness (43.4%), inconvenience (16.8%), and lack of time (7%). Only three participants in the study considered sunscreen unhealthy [24]. Fortunately, in our study only one person held the false belief that UV filter is harmful. Some of these issues could be addressed through educational campaigns highlighting the benefits of sun protection or by use of periodic alerts sent to residents.
Conclusions
A large part of the surveyed group did not use sunscreen, with the majority being men, individuals with vocational education, and those living in rural areas. The most conscientious application was demonstrated by women aged 16-25.
In addition to skin-protective products with UV filter for sun protection, the surveyed individuals most commonly used protective eyewear and headgear.
The most common reasons for the actions related to sun protection undertaken by the surveyed individuals were avoiding sunburns, preventing premature skin aging, and preventing the development of melanoma.