
Introduction
Liver cirrhosis is the end result of the fibrogenesis that occurs with chronic liver injury, and its natural history is marked by decompensation of the disease, and the development of ascites is the most frequent first decompensating event [1]. Clinical decompensation is mostly related to a progressive rise in portal pressure, circulatory dysfunction, and more recently systemic inflammation [2]. In this stage of the disease, endotoxins and proinflammatory cytokines increase splanchnic arterial vasodilation, leading to a marked reduction in systemic vascular resistance with stimulation of the renin-angiotensin-aldosterone system (RAAS), sympathetic nervous system (SNS), and the release of arginine-vasopressin (AVP). The stimulation of these vasoconstrictor systems induces sodium and water retention, which is associated with the occurrence of ascites, dilutional hyponatraemia, and finally hepatorenal syndrome (HRS) [3, 4].
Spontaneous bacterial peritonitis (SBP) is one of the major complications of ascites and it is defined as an infection of the ascitic fluid without an obvious abdominal source. It is the most prevalent infection in hospitalized cirrhotic patients, responsible for about 10-30% of all bacterial infections, with a 20-30% mortality rate [5]. In recent studies, gastrointestinal stasis secondary to portal hypertension and overactive SNS, intestinal dyskinesia, and relative insufficiency in gastric acid and bile secretion resulted in small intestinal bacterial overgrowth (SIBO) and endotoxaemia. Moreover, cirrhotic patients with ascites have increased intestinal permeability, immune dysfunction, and low ascitic fluid opsonic activity. These factors together with SIBO promote bacterial translocation and finally SBP [6]. The development of SBP worsens liver failure, impairs left ventricular contractibility, and adds to the haemodynamic abnormalities previously mentioned with more reduction in the vascular resistance of the splanchnic and systemic circulation. SBP is the most common precipitant of HRS [2].
Arginine-vasopressin is a potent antidiuretic hormone. Because of its systemic vasoconstrictor effects, and crucial role in maintaining circulatory homeostasis, it could presumably serve as a marker of circulatory dysfunction and clinical decompensation in cirrhosis. Moreover, AVP levels increased in stressful situations including sepsis and systemic inflammation [7]. However, measurement of AVP is challenging due to its short half-life, small size, ability to bind platelets, and secretion in a pulsatile pattern. Copeptin is a stable and highly sensitive surrogate marker for AVP secretion. It is the cleavage product of the C-terminal portion of the AVP precursor and is released from the posterior pituitary in equimolar amounts in response to AVP release stimulating conditions [7, 8].
Recent studies have shown that copeptin, independent of liver-specific scoring systems, predicts disease progression and prognosis in cirrhotic patients [7]. To the best of our knowledge, few studies have addressed the relationship between copeptin and sepsis in cirrhosis; moreover, they were performed on variable types of infections [3, 9]. Therefore, we conducted this study with a focus on its possible role in patients with SBP. We aimed to explore the possible association between copeptin and complications of liver cirrhosis with stress on its potential role as an inflammatory biomarker in SBP.
Material and methods
Patients
Between June 2021 and February 2022, an observational cross-sectional study was carried out in the Tropical Medicine and Gastroenterology Department at Sohag University Hospitals in Sohag, Egypt. The Sohag Faculty of Medicine’s Medical Research Ethics Committee (MREC) gave its approval to the study protocol (IRB number: Soh-Med-21-04-24), ClinicalTrials.gov (ID: NCT05401721). Before enrolment, informed written consent was sought from every participant or their relatives (for patients who were comatose).
A total of 89 cirrhotic ascitic patients (64 males, 25 females) were included, 37 (41.57%) with SBP and 52 (58.43%) without SBP. The diagnosis of liver cirrhosis was based on clinical data and findings from abdominal ultrasound. The diagnosis of SBP was based on the presence of at least 250 cells/ml of polymorphonuclear leucocytes (PMNLs) in the ascitic fluid, with or without positive ascitic fluid culture, and the lack of secondary peritonitis and haemorrhagic ascites [10].
We excluded patients with prior antibiotic treatment before hospital admission, severe infections other than SBP, malignancies other than hepatocellular carcinoma (HCC), previous liver or kidney transplantation, chronic kidney disease on haemodialysis, coronary insufficiency, heart failure, shock, and polyuria-polydipsia syndrome.
Methods (see Supplementary Methods and Supplementary Table 1 for more details)
Table 1
Baseline demographic, clinical, and laboratory characteristics of the studied cohort
[i] SBP – spontaneous bacterial peritonitis, HBV – hepatitis B virus, HCV – hepatitis C virus, AIH – autoimmune hepatitis, UGIB – upper gastrointestinal bleeding, HRS – hepatorenal syndrome, HCC – hepatocellular carcinoma, SIRS – systemic inflammatory response syndrome, MAP – mean arterial pressure, WBCs – white blood cells, PMNLs – polymorphonuclear leucocytes, ALT – alanine aminotransferase, AST – aspartate aminotransferase, INR – international normalized ratio, CRP – C-reactive protein, MELD-Na – Model for end-stage liver disease sodium corrected, eGFR – estimated glomerular filtration rate.
All patients were subjected to a thorough medical history and clinical examination. Abdominal ultrasonography was performed and a triphasic computed tomography (CT) scan was done if a heterogenous liver or hepatic focal lesion was detected on ultrasonography to establish the diagnosis of HCC. Liver function tests, serum creatinine, copeptin, C-reactive protein (CRP), sodium, complete blood count (CBC), and serology for viral hepatitis (hepatitis B surface antigen [HBsAg], and hepatitis C virus [HCV] antibodies) were performed for all patients at admission. To diagnose SBP, a paracentesis was carried out under aseptic conditions, with the patient lying flat, and guided by abdominal ultrasonography, total ascitic fluid proteins, white blood cell count (WBCs), and PMNLs were determined. The Child-Turcotte-Pugh (CTP) [11], and model for end-stage liver disease sodium corrected (MELD-Na+) [12] scores were calculated to assess liver disease severity. The estimated glomerular filtration rate (eGFR) [13] was calculated to assess renal function.
Measurement of serum copeptin
Following the manufacturer’s instructions, an enzyme-linked immunosorbent assay (ELISA) Kit (Bioassay Technology Laboratory Cat. No. E1129Hu) was used to measure the serum concentration of copeptin, by serially diluting the kit-supplied standard solution, and a standard curve was prepared. 50 µl of calibrators and patient samples were added to the wells and 50 µl of streptavidin-horseradish peroxidase (HRP) was immediately added to each well and the plate was incubated at 37°C for 60 minutes. Following complete washing, 50 µl of substrate solution A and 50 µl of substrate solution B were added to each well and incubated at 37°C for 10 minutes in the dark. The enzyme reaction was stopped by the addition of 50 µl of sulphuric acid (stop solution). Thermo Fisher Scientific Multi-skan EX Microplate Reader (Thermo Fisher Scientific Oy, FI-01621 Vantaa, Finland) was used to measure the change of colour from blue to yellow at 450 nm. Copeptin levels (pmol/l) were detected by comparing the OD of the samples to the standard curve.
Statistical analysis
Data were analysed using IBM-SPSS 25 (IBM Corp., Armonk, NY, USA). Data were expressed as mean, standard deviation (SD), median, interquartile range (IQR), frequency, and/or percentage as appropriate. The normality of continuous variables was tested using the Shapiro-Wilk test. Chi-square/Fisher’s exact test was used to compare the difference in the distribution of frequencies among different groups. Student’s t-test was performed to compare the means of dichotomous parametric data. Mann-Whitney U/independent sample Kruskal-Wallis test analysis was performed to compare the medians of non-parametric data. Univariate and multivariate logistic regression analyses were used to test the independent predictors of SBP in patients with ascites. The receiver operating characteristics (ROC) curve depicted the diagnostic performance of copeptin for the prediction of SBP in ascitic patients. The Spearman rank correlation coefficient was calculated for univariate correlations of copeptin level with other parameters. The p-value was considered significant when it was < 0.05.
Results
Baseline characteristics of the studied population
The baseline characteristics of study patients are depicted in Table 1 and Supplementary Table 2. The mean age was 61.27 ±11.13 years (range, 35-80), 71.91% were male, and HCV was the main aetiology of cirrhosis in our patients (84.27%). Patients with SBP were younger than those without SBP and they had a significantly higher prevalence of fever, abdominal pain, abdominal tenderness, upper gastrointestinal bleeding (UGIB), systemic inflammatory response syndrome (SIRS), and significantly lower mean arterial pressure (MAP). Patients with SBP also had significantly higher levels of copeptin, CRP, and WBCs. Other clinical and laboratory features were comparable between patient subgroups.
Table 2
Correlation between serum copeptin level and other parameters in the studied cohort
MAP – mean arterial pressure, WBCs – white blood cells, PMNLs – polymorphonuclear leucocytes, ALT – alanine aminotransferase, AST – aspartate aminotransferase, INR – international normalized ratio, Na – sodium, RBCs – red blood cells, CRP – C-reactive protein, MELD-Na – model for end-stage liver disease sodium corrected, eGFR – estimated glomerular filtration rate
Copeptin was significantly higher in patients with SBP and SIRS
As previously mentioned, copeptin was significantly elevated in patients with SBP compared to those without SBP (p = 0.032) (Table 1). Moreover, it was significantly correlated with ascitic fluid study parameters with a positive correlation with ascitic fluid WBCs and PMNLs (p = 0.025 and 0.008, respectively), and a negative correlation with ascitic fluid protein (p = 0.028) (Table 2). Finally, we noted that copeptin was significantly higher in patients with SIRS (p = 0.036), with a significant positive correlation with systemic inflammatory markers, namely WBCs and CRP (p = 0.002 and 0.01, respectively) (Tables 2 and 3).
Table 3
Association between copeptin and cirrhosis-related complications, eGFR, and SIRS in the studied cohort
Indicators of SBP development among ascitic patients
On univariate logistic regression analysis (Supplementary Table 3), the presence of fever, abdominal pain, abdominal tenderness, SIRS, elevated WBCs, copeptin, and CRP levels were substantially associated with SBP development. Multivariate logistic regression analysis (Table 4) was applied to the significant factors in the univariate model and revealed that elevated copeptin (OR = 1.39, 95% CI: 1.013-1.908, p = 0.042), and CRP (OR = 1.849, 95% CI: 1.17-2.923, p = 0.008), were independent risk factors for the presence of SBP in cirrhotic patients with ascites.
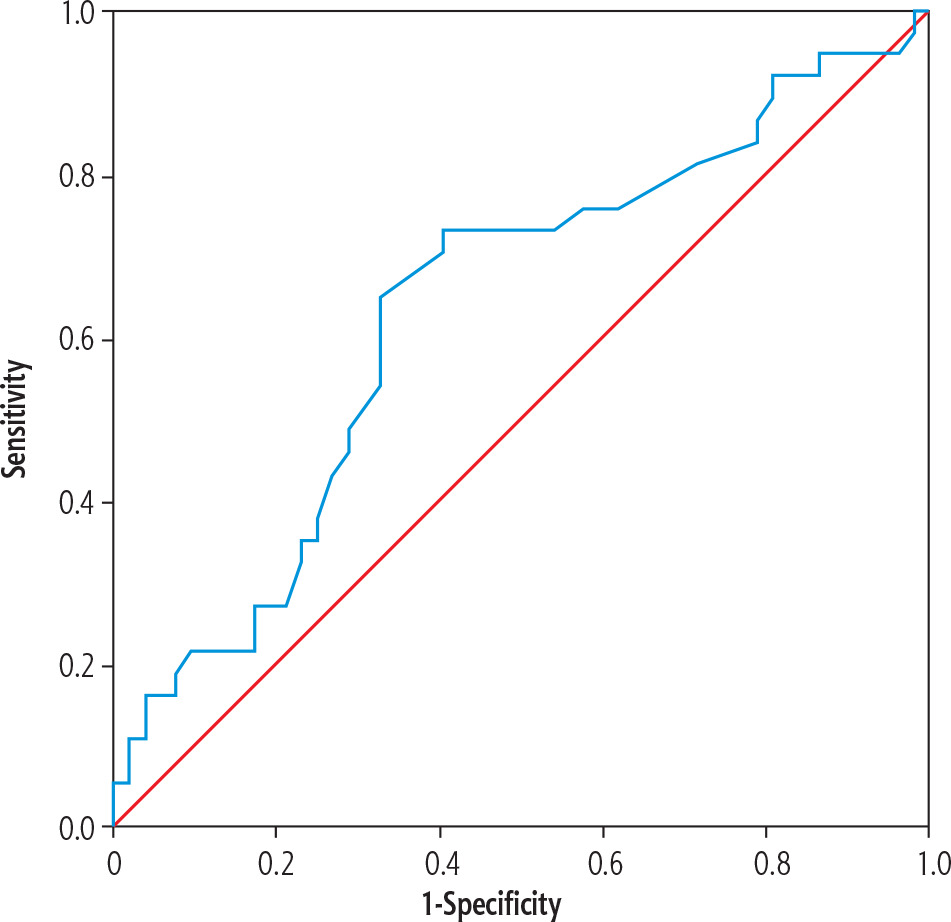
ROC curve analysis of the diagnostic efficacy of copeptin for the detection of SBP
We noted that at a cut-off value of 9 pmol/l, copeptin had 73% sensitivity and 64% specificity for detecting SBP [AUC (95% CI): 0.634 (0.515-0.753)] with a positive predictive value (PPV) of 67%, negative predictive value (NPV) of 71%, and an overall accuracy of 68.5% (Table 5, Fig. 1).
Copeptin correlates with liver, renal, and circulatory functions, and is associated with complications of liver cirrhosis
Copeptin showed a significant positive correlation with alanine aminotransferase (ALT), aspartate aminotransferase (AST), international normalized ratio (INR), total bilirubin, Child, and MELD-Na scores, and a significant negative correlation with albumin. Moreover, Child class C patients had significantly higher copeptin levels than those with Child B (p < 0.001), suggesting a strong relationship between copeptin and liver damage, functional reserve, and stage of the disease (Tables 2 and 3). Patients with UGIB, hepatic encephalopathy (HE), and HRS had significantly higher copeptin levels than those who did not experience these complications (p = 0.029, 0.007, and 0.016, respectively). Moreover, patients with moderate to marked ascites had significantly higher copeptin levels than those with mild ascites (p = 0.049 and 0.014, respectively) (Table 3). No significant difference in copeptin levels was found between patients with and without HCC (p = 0.126).
We noted a significant correlation between copeptin and kidney function parameters, as evidenced by a significant positive correlation with creatinine and a significant negative correlation with eGFR (all p < 0.001). Moreover, patients with eGFR < 60 ml/min/1.73 m2 had significantly higher copeptin levels (Tables 2 and 3). Finally, copeptin demonstrated a strong correlation with circulatory function, as evidenced by a significant positive correlation with the pulse, and a significant inverse correlation with MAP and sodium (Table 2).
Discussion
The study’s main finding is that cirrhotic patients with SBP have significantly higher copeptin levels than those without SBP. In addition, copeptin was found to be an independent risk factor for SBP development. To the best of our knowledge, this study is the first to report a relationship between copeptin and SBP in cirrhotic patients with ascites, as previous studies in cirrhosis were conducted on different types of infections.
Copeptin is the C-terminal portion of the AVP precursor and is released from the posterior pituitary together with AVP in equimolar amounts in response to AVP release stimulating conditions [4]. However, the stability and long half-life of copeptin make it a better marker than AVP in clinical practice. AVP and hence copeptin is released in response to haemodynamic or osmotic stimuli; moreover, it is elevated in the setting of systemic inflammation and sepsis [3].
We found that serum copeptin was significantly elevated in patients with SBP (p = 0.032), with a significant correlation with the parameters of the ascitic fluid study. This finding could be attributed to several factors. First, bacterial translocation and the associating endotoxaemia which are implicated in the development of SBP and systemic inflammation in cirrhosis directly increase the production of vasopressin and copeptin independently of osmotic stimuli or baroreceptor activity, as evidenced by the significant correlation of copeptin with markers of systemic inflammation, namely CRP and WBCs, as been demonstrated in previous studies [7, 9, 14, 15]. Moreover, copeptin was significantly elevated in patients presenting with SIRS criteria (p = 0.036). In agreement with our results, the value of copeptin as a marker of systemic inflammation and sepsis had been confirmed in several studies both in cirrhotic and non-cirrhotic populations [3, 16-18]. Second, MAP is significantly lower in our studied patients with SBP compared to those without SBP (p = 0.041); this drop in blood pressure results in a strong copeptin response secondary to stimulation of baroreceptors [16]. This pathophysiological mechanism is supported by the significant negative correlation between serum copeptin and MAP. The lower value of MAP in patients with SBP could be attributed to extensive bacterial translocation which triggers an inflammatory response, with increased release of vasoactive factors such as nitric oxide (NO) and proinflammatory cytokines such as interleukin 6 (IL-6) and tumour necrosis factor α (TNF-α), thereby resulting in more splanchnic vasodilation, with worsening of preexisting systemic circulatory dysfunction, leading to a further reduction in effective arterial blood volume and arterial pressure, and overactivation of endogenous vasoconstrictor systems including AVP [2].
When we performed a multivariate logistic regression analysis, copeptin and CRP were independently associated with the existence of SBP. Several risk factors for the presence of SBP have been investigated with variable results; however, the role of inflammation had been recognized in previous research [19]. Several studies have highlighted the potential role of copeptin in identifying the development, severity, and mortality from infections in different clinical settings [20-24]. However, our study is the first to be performed exclusively on SBP, which needs further validation in future studies. CRP is an acute phase reactant which is secreted from hepatocytes and elevated in conditions associated with systemic inflammation; it activates complement and reflects endogenous IL-6 activity [25]. In agreement with our results, Preto-Zamperlini et al. [26] and Falleti et al. [19] found that CRP was independently associated with the presence of SBP.
In this study, we found that copeptin detects SBP at a cutoff value of 9 pmol/l with sensitivity, specificity, PPV, NPV, and overall accuracy of 73%, 64%, 67%, 71%, and 68.5%, respectively. Furthermore, copeptin was significantly correlated with ascitic fluid WBCs, PMNLs, and total protein, so copeptin could serve as a diagnostic marker for SBP. Previous research revealed the potential association between copeptin and complications of liver cirrhosis [7, 8], as well as its increase in infections and sepsis in non-cirrhotic patients [16, 18]. This is the first time that the diagnostic value of copeptin in patients with SBP has been demonstrated, indicating that it is a sensitive marker of systemic inflammation and sepsis; however, this observation needs further validation on a larger cohort of patients.
In the current study, copeptin was significantly elevated in patients who presented with UGIB, a moderate to marked amount of ascites, and in those with advanced liver disease as assessed by Child-Pugh, and MELD-Na scores, which is consistent with previous studies [3, 4, 7, 8, 14]. This could be attributed to the ability of copeptin to reflect circulatory dysfunction as evidenced by its strong correlation with pulse, MAP, and sodium. In these patients, the stimulation of baroreceptors occurs due to the presence of significant arterial hypovolaemia secondary to splanchnic vasodilation and portal hypertension [4]. Moreover, blood loss in the case of UGIB adds to arterial hypovolaemia.
We found that copeptin was significantly increased in patients with HRS and those with renal impairment as estimated by creatinine levels and eGFR, as demonstrated in previous studies [4, 8, 27, 28]. There are two suggested mechanisms. First, copeptin levels would likely rise as kidney function decreased, since copeptin is eliminated by kidney excretion. Second, more copeptin is secreted in individuals with poorer renal function, because the AVP system is triggered due to decreased urine concentrating ability to maintain water homeostasis [27, 28]. In addition to the aforementioned mechanisms, elevated copeptin in patients with HRS could reflect the extensive circulatory dysfunction due to extreme splanchnic vasodilation, which activates vasoconstrictor systems including AVP. Moreover, a strong systemic inflammatory process which is characteristic of advanced cirrhosis may play a role [29].
The elevated copeptin level in patients with HE was demonstrated in previous studies [4, 7], which is consistent with our findings. Hyponatraemia and systemic inflammation (as indicated by elevated serum CRP) were involved in the pathogenesis of HE. The association of copeptin levels with sodium and CRP may explain the high copeptin levels in these patients [7].
Finally, the major features of acute decompensation of cirrhosis (SBP, HE, UGIB, HRS, and ascites) in our study could be explained in the light of the newly proposed systemic inflammation hypothesis, which posits that in patients with decompensated cirrhosis systemic inflammation is a chronic condition linked to persistent translocation of bacterial products from the intestinal lumen to the systemic circulation. The processes through which organ system dysfunctions or failures occur are bouts of systemic inflammation linked to episodic exacerbations of bacterial translocation or proinflammatory precipitants. So, the elevated copeptin levels in these conditions were related to its ability to reflect systemic inflammation. However, it should be noted that the development of major cirrhosis complications is likely to involve a synergistic interaction between systemic inflammation and organ-specific mechanisms such as portal hypertension, sodium retention, and hyperammonaemia [2]. The main limitations of this study were that it was a single-centre study on a relatively small number of patients. Moreover, the lack of follow-up measures of copeptin during and after completing antibiotic treatment hinders monitoring the impact of SBP treatment on copeptin levels.
Conclusions
In conclusion, copeptin is an independent risk factor for the presence of SBP in patients with cirrhosis, and it might be a tool for the diagnosis of SBP. Moreover, copeptin was significantly elevated in patients who presented with major complications of liver cirrhosis, demonstrating its ability to reflect circulatory dysfunction and systemic inflammation.





