
Introduction
Asthma is a chronic and heterogenous inflammatory pulmonary disease with several distinct phenotypes. Its symptoms include wheezing, shortness of breath, chest tightness, and cough of varying intensity. Asthma affects between 1% and 29% of the population in different countries. Treatment is primarily based on inhaled corticosteroids and beta-2 agonists, while biologic therapies are usually reserved for patients with severe asthma [1].
Asthma patients often suffer from comorbidities that influence the course of the disease. The most frequent mental disorders among individuals with asthma include anxiety, depression, personality disorders, and alcohol-related problems [2]. Patients with a late asthma diagnosis, additional comorbidities, and female gender are at higher risk of developing depression and anxiety, with a reported prevalence ranging from 11% to 13% [3–5].
Psychiatric comorbidities impact asthma management by contributing to poorer asthma control, reduced medication adherence, and lower asthma-related quality of life [1]. Mental health disorders and asthma are in a bidirectional relationship, wherein asthma exacerbates psychiatric symptoms, and mental health conditions can worsen asthma outcomes. Asthma increases the risk of developing mental health disorders, and patients with depression are more likely to have asthma [6, 7]. Global Initiative for Asthma (GINA) emphasises the lack of a structured treatment plan for asthma patients with comorbid depression and anxiety. Although antidepressants and cognitive behavioural therapy show potential benefits in this context, the current evidence remains limited [1].
The aim of this review is to analyse current studies on the correlation between asthma and common mental health disorders. It highlights shared elements in the pathophysiology of asthma and depression or anxiety, discusses the negative impact of these comorbidities on disease management, and presents proposed psychiatric interventions for this patient group.
Depression in asthma patients
Depression is a mental disorder characterised by persistent sadness, loss of interest or pleasure, reduced energy, impaired cognition, and disturbances in sleep and appetite. As reported by the World Health Organisation (WHO), in 2021, depression affected approximately 3.8% of the global population [8].
A systematic review and meta-analysis by Jiménez-Peinado et al. (2025), including 15 studies with a total of nearly 500,000 patients, found that the prevalence of asthma in individuals with depression is twice as high as that reported in the general global population [9]. Individuals with asthma have a 30% higher risk of developing depression compared to those without asthma [10]. On the other hand, patients with depression are 3.14 times more likely to have asthma compared to those without that condition [6].
Currently, studies have suggested that a special communication – the brain-lung axis – plays a potential role in the course and pathogenesis of pulmonary diseases, including asthma. This term relates to the bidirectional relationship between brain and lung, the ways of communication of which comprise the central and peripheral nervous, endocrine, and immunological system, and microbiota. These elements cooperate with each other, creating a complex system of bilateral interactions of lung and central nervous system, which can explain the correlation between the occurrence of mental disorders and pulmonary diseases [11].
Asthma involves chronic airway inflammation, with elevated proinflammatory cytokines in blood such as IL-1, IL-4, IL-6, and TNF-α during exacerbations. On the other hand, patients with asthma and psychological symptoms like depression and anxiety show significantly higher levels of IFN-γ, TNF-α, and IL-17A [10]. According to meta-analyses and systematic reviews, depression is also associated with significant alterations in the levels of IL-1β, IL-2, IL-4, IL-5, IL-8, the soluble IL-6 receptor, CCL3, IL-17A, and TGF-β1 [12]. Zhu et al. (2019) also demonstrated shared genetic factors between asthma and depressive disorders. However, the underlying mechanisms driving the co-occurrence of asthma and depression remain poorly understood [13]. According to a U-BIOPRED study involving patients with varying asthma severity, individuals with severe asthma showed significantly higher levels of anxiety and depression, which were associated with elevated inflammatory markers such as IL-6, MCP-1, CCL17, and CCL18, suggesting that inflammation may underlie this comorbid condition [14].
Based on a study conducted by Chen et al. (2025) among 19,195 current asthma and 11,972 ever asthma patients, individuals with comorbid depression reported a higher frequency of asthma attacks (57.25% vs. 42.73%), emergency visits (15.31% vs. 9.90%), rescue medication use (73.11% vs. 63.17%), and work disruption due to asthma, compared to those without depression [15]. Moreover, a study by Patel et al. (2017) among adults aged ≥ 55 years demonstrated that those with both asthma and depression experienced increased sleep disturbances, and activity limitations compared to their non-depressed counterparts. They also reported significantly poorer health-related quality of life across physical, mental, and general health domains. However, no significant differences were found in spirometric values [16].
Asthmatic patients with comorbid depression had a 31% higher risk of experiencing asthma attacks. Asthmatic patients with depression demonstrated a significantly higher prevalence of sinusitis, respiratory allergy, and food allergy. Moreover, they presented with a greater mean number of allergic comorbidities, suggesting a potential link between depressive symptoms and the burden of allergic disease in asthma [15].
A hospital-based cross-sectional study among 102 adolescents with asthma found that poor and intermediate inhaler adherence were significantly associated with higher odds of depression, while lower family income also emerged as an independent predictor [17]. These findings suggest that, similarly to adults, certain psychosocial and behavioural patterns such as treatment nonadherence and socioeconomic disadvantage may contribute to the co-occurrence of asthma and depression in adolescents.
According to a study conducted by Gajewski et al. (2023) among 592 adult patients with asthma and no diagnosed mood disorder, treatment with selective serotonin reuptake inhibitors (SSRIs) or serotonin and norepinephrine reuptake inhibitors (SNRIs) was associated with a significant improvement in asthma control. The study reported a decrease in oral corticosteroid prescriptions, emergency department visits, and hospitalisations within 12 months after starting SSRI/SNRI therapy. These findings suggest that SSRIs and SNRIs may improve asthma outcomes even in patients without comorbid depression, potentially through modulation of neuroimmune and inflammatory pathways [18].
In a 2023 study by Theodoro et al. involving 309 asthmatic subjects, those with untreated depression were more than three times as likely to have uncontrolled asthma symptoms and more than twice as likely to have airway obstruction, whereas subjects using antidepressants had similarly increased odds of uncontrolled symptoms but did not show a significant increase in airway obstruction [19].
Antidepressants, including SSRIs, SNRIs, and bupropion, are generally safe and well-tolerated across age groups, in both asthmatic and non-asthmatic individuals. SSRIs are preferred because they minimise respiratory side effects, although caution is advised when prescribing citalopram or escitalopram with albuterol due to the potential risk of QTc prolongation [20]. Additionally, psychological and lifestyle interventions show promise for improving both mental health and asthma outcomes, but more well-designed randomised trials are needed to confirm their effectiveness [21].
Anxiety disorders in asthma patients
Anxiety disorders are a group of mental health conditions characterised by excessive fear or worry that is disproportionate to the actual threat. These symptoms persist for several months and can be situation-specific, such as in panic or social anxiety disorder, or more generalised, as seen in generalised anxiety disorder. Anxiety disorders are the most prevalent mental health conditions globally, affecting an estimated 4% of the population [22].
According to a study by Ye et al. (2021), which included 106,813 participants, approximately 32% of individuals with asthma experience anxiety symptoms, and 24% have anxiety disorders, with significantly higher odds compared to non-asthmatic controls [23]. In a Ugandan case-control study among 162 adolescents, 46.6% of adolescents with asthma had anxiety disorders compared to 21.4% without asthma, with the strongest associations found for generalised anxiety disorder and panic disorder, suggesting shared early-life risk factors [24]. However, due to the small sample size, further research is warranted to confirm these findings among adolescents.
Asthma and anxiety disorders may share common aetiopathogenetic mechanisms involving dysregulation of psycho-neuro-immunological pathways, particularly an imbalance in proinflammatory cytokines and Th2-mediated immune responses. This shared inflammatory profile could partly explain the high comorbidity observed between these conditions [25]. However, these mechanisms are not yet fully understood and require further investigation.
According to Chen et al. (2025), asthmatic patients with anxiety were more likely than those without anxiety to experience asthma attacks (54.3% vs. 41.5%), emergency visits (12.9% vs. 9.9%), rescue medication use (69.2% vs. 62.9%), and hospitalisations, work disturbances due to asthma, and reported worsening of asthma since initial diagnosis. Additionally, a significantly higher proportion of patients with anxiety had never used controller medications, suggesting poorer treatment adherence [15]. A study conducted by Licari et al. (2022), involving 87 adolescents with a median age of 14.2 years, found that 44.4% of participants with uncontrolled asthma had scores above 35 points on the Childhood Anxiety Sensitivity Index (CASI) – a self-report tool assessing anxiety sensitivity – compared with 14.6% of adolescents with well-controlled asthma and 10% of those with partly controlled asthma. This suggests a significant association between elevated anxiety sensitivity and poor asthma control [26]. There is a significant negative correlation between anxiety levels and quality of life in asthma patients, indicating that higher anxiety is associated with a substantial decrease in quality of life, even when asthma symptoms are clinically controlled [27]. According to a systematic review by Pateraki et al. (2016), anxiety-focused cognitive behavioural therapy shows preliminary effectiveness in reducing anxiety in adults with asthma, with promising but limited evidence in children, particularly when tailored to clinical anxiety and combined with asthma education [28].
Discussion
The research was conducted in the Google Scholar, PubMed, and ResearchGate databases on articles mainly published between 2019 and 2025. Older studies were also cited when more recent publications were not available. The article also cites information from the WHO online database and GINA document. The search included the following terms: “depression”, “asthma”, “anxiety”. The chosen abstracts were read, and only relevant ones were analysed and summarised. Original studies and review articles in English language were concerned.
GINA identifies major psychological problems as modifiable risk factors for asthma exacerbations, emphasising that arranging a mental health assessment for patients with symptoms of anxiety or depression, helping them distinguish between anxiety and asthma symptoms, and providing guidance on managing panic attacks can reduce exacerbations and minimise the need for oral corticosteroids [1]. Psychological distress has been strongly linked to increased asthma severity, more frequent exacerbations, and reduced quality of life, as well as to poor treatment response and adherence in patients with anxiety and depression. These findings have led researchers to identify these conditions as extrapulmonary barriers to achieving remission and as important treatable traits in asthma management [15]. The impact of depression and anxiety on asthma control and related outcomes is presented in Table 1.
Table 1
Moreover, severe asthma often interferes with family, social, and work life, limits career choices and vacation options, and affects emotional well-being. This ongoing burden and sense of isolation can also have a significant impact on mental health [1].
Recognising depression and anxiety as treatable traits allows clinicians to implement targeted interventions – such as pharmacological treatment with antidepressants, cognitive behavioural therapy, and lifestyle modifications – which can improve both mental health and asthma-related outcomes [19, 21, 28].
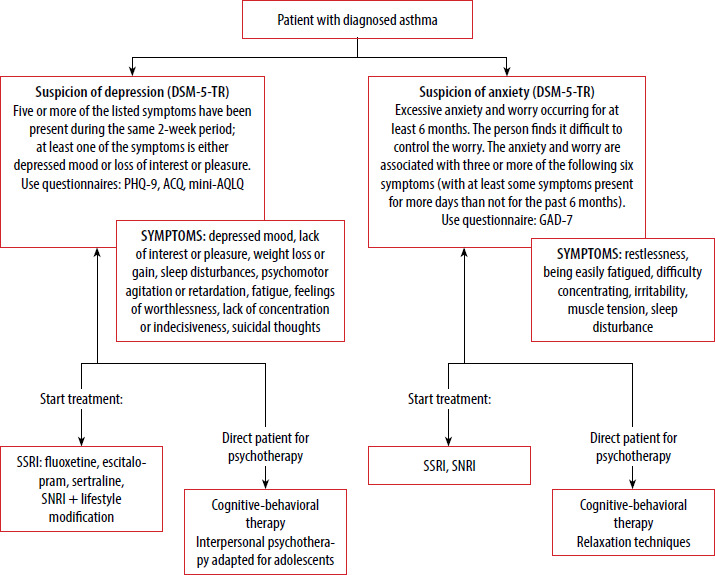
Best practice recommendations emphasise early detection of depression and anxiety, followed by prompt initiation of pharmacological or psychotherapeutic interventions in clinical settings. The Patient Health Questionnaire-9 (PHQ-9) questionnaire is a simple and reliable self-assessment tool for diagnosing depression and monitoring treatment response, with scores ≥ 10 indicating probable clinical depression that requires confirmation and management [20]. In 2020, a study conducted by Robinson et al. among 300 patients with poorly controlled asthma demonstrated that Asthma Control Questionnaire (ACQ) and mini-AQLQ scores were significantly correlated with Generalized Anxiety Disorder 7-item scale (GAD-7) and PHQ-9 scores, indicating that asthma-specific questionnaires can reflect levels of anxiety and depression. A mini-AQLQ score greater than 3 suggested a low likelihood of co-morbid anxiety or depression, supporting the feasibility of targeted psychological screening in this population [29].
Routine screening of asthma patients for depression, combined with prescribing antidepressants when clinically indicated, can improve both psychiatric symptoms and asthma control [30]. The abbreviated diagnostic pathway for asthma patients with psychiatric disorders is presented in Figure 1.
Conclusions
It is important that further assessment and management be conducted by a specialist, preferably within a multidisciplinary severe asthma clinic, which should ideally include a mental health professional to address the psychological aspects of the disease [1].
Emerging evidence supports the effectiveness of psychological interventions in improving asthma outcomes. These include cognitive behavioural therapy, relaxation techniques, breathing exercises, and pharmacological treatments such as antidepressants.
Systematic reviews have demonstrated beneficial effects of these approaches on both mental health and asthma control [15]. However, further research is needed to improve treatment for asthma patients with anxiety disorders or depression.










