
Introduction
Chronic inflammation of the lower respiratory tract is involved in the pathogenesis of both asthma and chronic obstructive pulmonary disease (COPD) [1, 2].
The long-term goals of asthma therapy are to obtain a good control of symptoms, maintain a healthy level of activity as well as to minimize the risk of exacerbations, airflow reduction and side effects [1]. The choice of drugs in the treatment of asthma depends on the degree of disease control. Currently there are 5 degrees of treatment, reflecting its intensity. Drugs used in the treatment of asthma are prescribed for permanent use for controlling symptoms and immediate use temporarily in case of the exacerbation. Drugs controlling the course of the disease include: inhaled corticosteroids (ICS) – currently most effective anti-inflammatory drugs preferred in chronic asthma, antileukotrienes, long-acting β2-adrenergic agonists (LABA), theophylline in a sustained release form, cromones, oral LABA – used exceptionally, anti-IgE antibodies (omalizumab), corticosteroids applied systemically – primarily orally. Drugs used temporarily include: fast-acting inhaled β2-mimetics, corticosteroids applied systemically – primarily orally, optionally intravenously, anticholinergics drugs, theophylline in a short-acting form, fast-acting oral β2-mimetics used rarely, if the patient cannot take medications by inhalation. In asthma treatment, administration of drugs by inhalation is preferred because the drug reaches the airways directly and reaches the therapeutic concentration with a limited risk of systemic adverse effects. ICS and LABA are recommended in the second and higher degrees of treatment [1].
The goal of treatment in stable COPD is to decrease severity of disease symptoms, improve tolerance of exercise and health condition as well as to prevent disease progression, prevent and treat exacerbations and reduce mortality. A number of factors, including perceived severity of dyspnoea, frequency of exacerbations, the severity of the airflow restriction through the bronchi should be taken into account in taking the therapeutic decision. Currently available drugs can improve bronchial patency, reduce dyspnoea and other symptoms and reduce the frequency of exacerbations. The therapeutic options include: bronchodilators (short-acting β2-mimetics, LABA, short-acting anticholinergics), ICS and phosphodiesterase 4 inhibitors [2, 3]. It should be noted that polytherapy with ICS and LABA is more effective than monotherapy with each of these drugs [4, 5].
There are no data on making the therapeutic decision by Polish doctors concerning the prescription of polytherapy with ICS and LABA in asthma and COPD and factors influencing these decisions.
Aim
The aim of the multicentre, open-label, post-marketing observational survey was to assess the therapeutic preferences in the use of polytherapy with ICS and LABA in patients with asthma or COPD in daily clinical practice. In addition, the efficacy and tolerance of the prescribed inhaled therapy was assessed.
Material and methods
A nation-wide, multicentre, open-label, post-marketing observational survey involved 245 doctors (11 general practitioners, 23 allergists and 211 pulmonologists) and 13,800 patients treated with ICS and LABA (7,416 diagnosed with asthma and 6,384 diagnosed with COPD) interviewed during two subsequent visits. The survey did not meet the criteria of a medical experiment and thus did not require the Bioethics Committee’s approval. It was performed from January 2016 to December 2018.
The survey was performed among doctors recruited by medical representatives, specialists in family or internal medicine, pulmonology or allergology, currently licensed to practice, who completed and signed the Application Form for the Study and mailed it to Europharma.
The inclusion criteria for outpatients were: age of 18 years and over, diagnosis of asthma or COPD, and use of polytherapy with ICS and LABA. The exclusion criterion was inability to obtain answers to questions contained in the survey and refusal of the patient to participate in the survey.
The participating physician had a dual role in the survey. They answered the questions regarding their medical practice and filled out questionnaires for at least 20 patients who fulfilled the inclusion criteria during one visit resulting from a clinical need of the patient.
The first part of the questionnaire included demographic data of the doctors (speciality, work experience, place of work) and data on their clinical practice (the frequency of use of different polytherapy with ICS and LABA in patients with asthma or COPD and factors affecting these decisions).
The second part of the questionnaire on the first visit included patients’ demographic data (gender, age, education level, place of residence and professional activity), clinical data (basic diagnosis due to the patient’s request, duration of asthma or COPD, number of asthma and COPD exacerbations and related hospitalizations during the least 3 months, the degree of asthma and COPD control, recommended treatment regimen and occurrence of concomitant diseases). On visit 2 (about 3 months after visit 1) control of disease symptoms was assessed.
In addition, the patients’ opinion on effectiveness and tolerance of used pharmacotherapy consisted with ICS and LABA were assessed on the basis of a 4-point scale (1 – no, 2 – moderate, 3 – good, 4 – very good and 1 – difficult-to-accept discomfort, 2 – acceptable discomfort, 3 – good tolerance, 4 – very good-tolerance, respectively).
Statistical analysis
Statistical analysis was performed with Statistica 12.0 software (TIBCO Software Inc., Palo Alto, CA, USA). Values of variables were presented as percentages and mean values with standard deviations (SD). Separate groups were compared using the χ2 test and χ2 test for trend. The value of p < 0.05 was considered to be statistically significant.
Results
Doctors’ therapeutic preferences
The study group of doctors (characteristics presented in Table 1) most frequently declared the use of formoterol with fluticasone in polytherapy of asthma and COPD (81.1% and 82.0%, respectively). The most important factors declared by physicians as determining the choice of this polytherapy in the treatment of asthma and COPD were efficacy (88.2% and 82.4%, respectively) and safety (83.3% in both cases) – Table 2.
Table 1
Characteristics of the study group of doctors (n = 245)
Table 2
Therapeutic preferences and factors determining the choice of polytherapy with ICS and LABA in patients with asthma and COPD declared by doctors
Factors determining the use of polytherapy with ICS and LABA in enrolled patients
The analysis included 7,416 patients with asthma, and 6,384 with COPD (Table 3). Concomitant diseases occurred in 44.0% of patients with asthma, and 84.6% with COPD, most often hypertension.
Table 3
Characteristics of patients’ study groups treated with ICS and LABA
The severity of asthma was assessed as controlled in 53.5%, partially controlled in 41.2% and uncontrolled in 5.3% of the study group. Exacerbation of the disease during the last 3 months was reported by 28.8% of patients (in 75.8% once, 21.6% twice and 2.6% more than twice). 5.2% of patients with asthma were hospitalized due to the exacerbation in the last 3 months.
The severity of COPD was scored as category A in 3.8%, B in 35.8%, C in 40.6% and D in 19.8% of patients. Exacerbation of the disease in the last 3 months was reported by 44.9% of patients (in 71.1% once, 25.7% twice and 3.2% more than twice). 13.6% of patients with COPD were hospitalized due to the exacerbation in the last 3 months (Table 4).
Table 4
Clinical characteristics of the study groups
The most frequent ICS with LABA polytherapy in patients with asthma and COPD included: formoterol with fluticasone (71.1% and 81.4%, respectively), formoterol with budesonide (11.2% and 8.7%, respectively), formoterol with beclomethasone (8.0% and 4.6%, respectively), and salmeterol with fluticasone (7.5% and 9.2%, respectively) – Table 4. The most important factors determining the use of ICS and LABA polytherapy in the treatment of asthma as well as COPD were: safety, efficacy, the doctor’s own experience with use of this drug, convenience of use, and impact of pharmacotherapy on the quality of life (Table 5).
Table 5
Factors influencing the use of polytherapy with ICS and LABA
The efficacy and tolerance of pharmacotherapy used
During the observation, 96.5% of the study group continued the treatment. The most frequent reasons for discontinuation were resolution of symptoms (25.4%). In 5.8% of the study group an exacerbation of the disease occurred (in 95.6% once), and 0.9% of patients were hospitalized due to the exacerbation of the disease (all once).
During the observation, in patients with asthma, the efficacy of pharmacotherapy used and assessed as very good increased significantly (from 64.6% to 79.7%, p < 0.001). On the first visit, the percentage of patients with asthma who assessed efficacy of pharmacotherapy used as very good was the highest among patients treated with formoterol and fluticasone (71.2%) and the lowest among patients treated with salmeterol and fluticasone (57.8%). During the observation, the efficacy of polytherapy with most frequent combinations of ICS and LABA in asthma control increased significantly (Figures 1 A–D). The highest scores at the end of observation were showed for formoterol with budesonide (82.3%).
Figure 1
A – The assessment of efficacy of all pharmacotherapy used in patients with asthma. B – The assessment of efficacy of formoterol with budesonide in patients with asthma. C – The assessment of efficacy of formoterol with fluticasone in patients with asthma. D – The assessment of efficacy of salmeterol with fluticasone in patients with asthma. E – The assessment of efficacy all pharmacotherapy used in patients with COPD. F – The assessment of efficacy of formoterol with budesonide in patients with COPD. G –The assessment of efficacy of formoterol with fluticasone in patients with COPD. H – The assessment of efficacy of salmeterol with fluticasone in patients with COPD
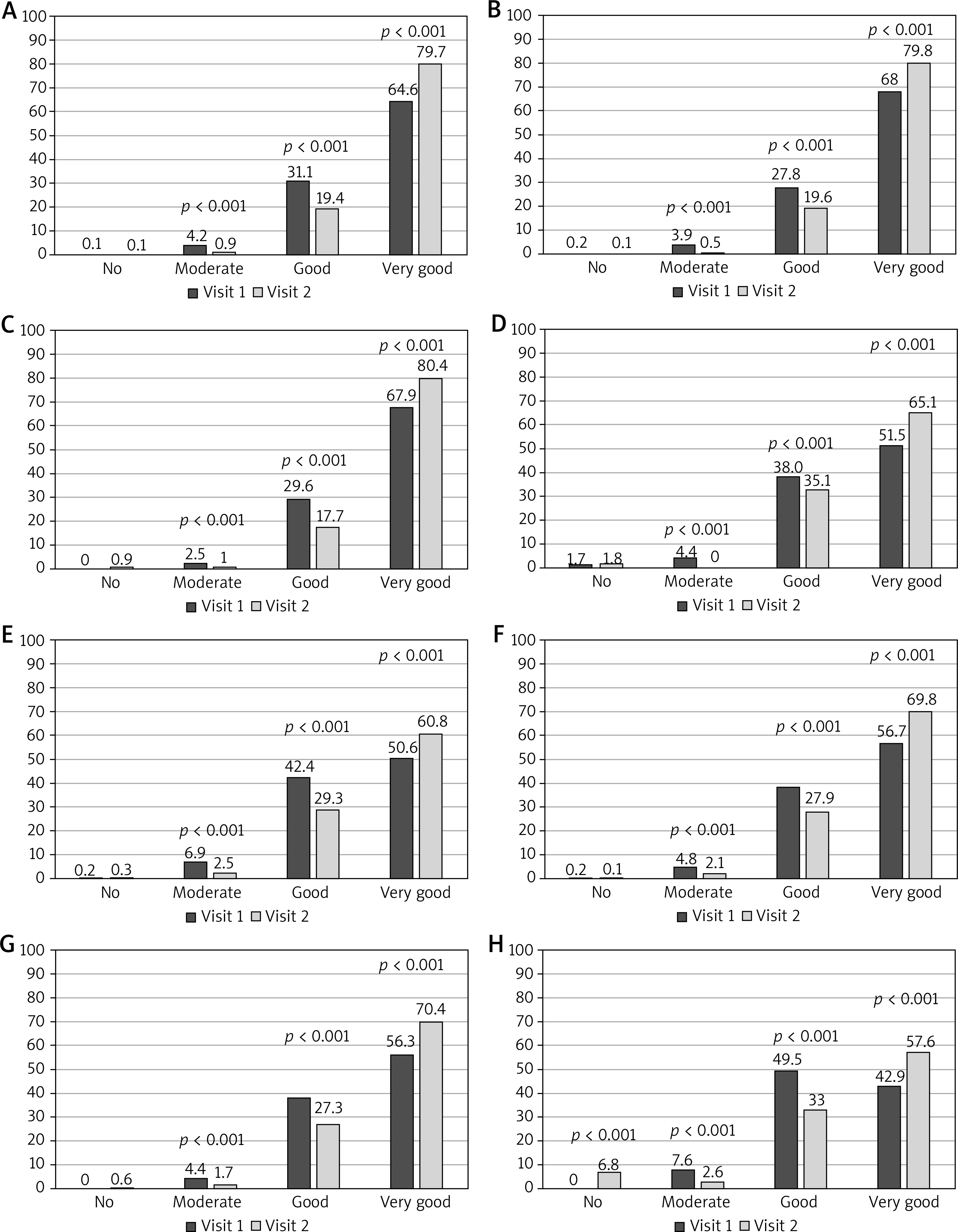
Similarly, during the observation in all patients with COPD, the efficacy of pharmacotherapy used and assessed as very good increased significantly (from 50.6% to 68.0%, p < 0.001). On the first visit, the percentage of patients with COPD who assessed efficacy of pharmacotherapy used as very good was the highest among patients treated with formoterol and fluticasone (56.3%) and the lowest among patients treated with formoterol and budesonide (34.9%). In the subgroup with COPD receiving polytherapy with formoterol and fluticasone, the efficacy assessed as very good increased significantly (from 56.3% to 70.4%, p < 0.001), with formoterol and budesonide (from 34.9% to 61.2%, p < 0.001) and with salmeterol and fluticasone (from 42.9% to 57.6%, p < 0.001) – Figures 1 E–H.
During the observation in all patients with asthma, the tolerance of pharmacotherapy used and assessed as very good increased significantly (from 69.0% to 79.8%, p < 0.001). On the first visit, the percentage of patients with asthma who assessed tolerance of pharmacotherapy used as very good was the highest among patients treated with formoterol and fluticasone (62.3%) and the lowest among patients treated with formoterol and budesonide (39.2%). In a subgroup with asthma on polytherapy with formoterol and fluticasone, the tolerance assessed as very good increased significantly (from 62.3% to 72.6%, p < 0.001), with formoterol and budesonide (from 39.2% to 59.0%, p < 0.001) and with salmeterol and fluticasone (from 49.1% to 59.3%, p < 0.001) – Figures 2 A–D.
Figure 2
A – The assessment of tolerance all pharmacotherapy used in patients with asthma. B – The assessment of tolerance of formoterol with budesonide in patients with asthma. C – The assessment of tolerance of formoterol with fluticasone in patients with asthma. D – The assessment of tolerance of salmeterol with fluticasone in patients with asthma. E – The assessment of tolerance all pharmacotherapy used in patients with COPD. F – The assessment of tolerance of formoterol with budesonide in patients with COPD. G – The assessment of tolerance of formoterol with fluticasone in patients with COPD. H – The assessment of tolerance of salmeterol with fluticasone in patients with COPD
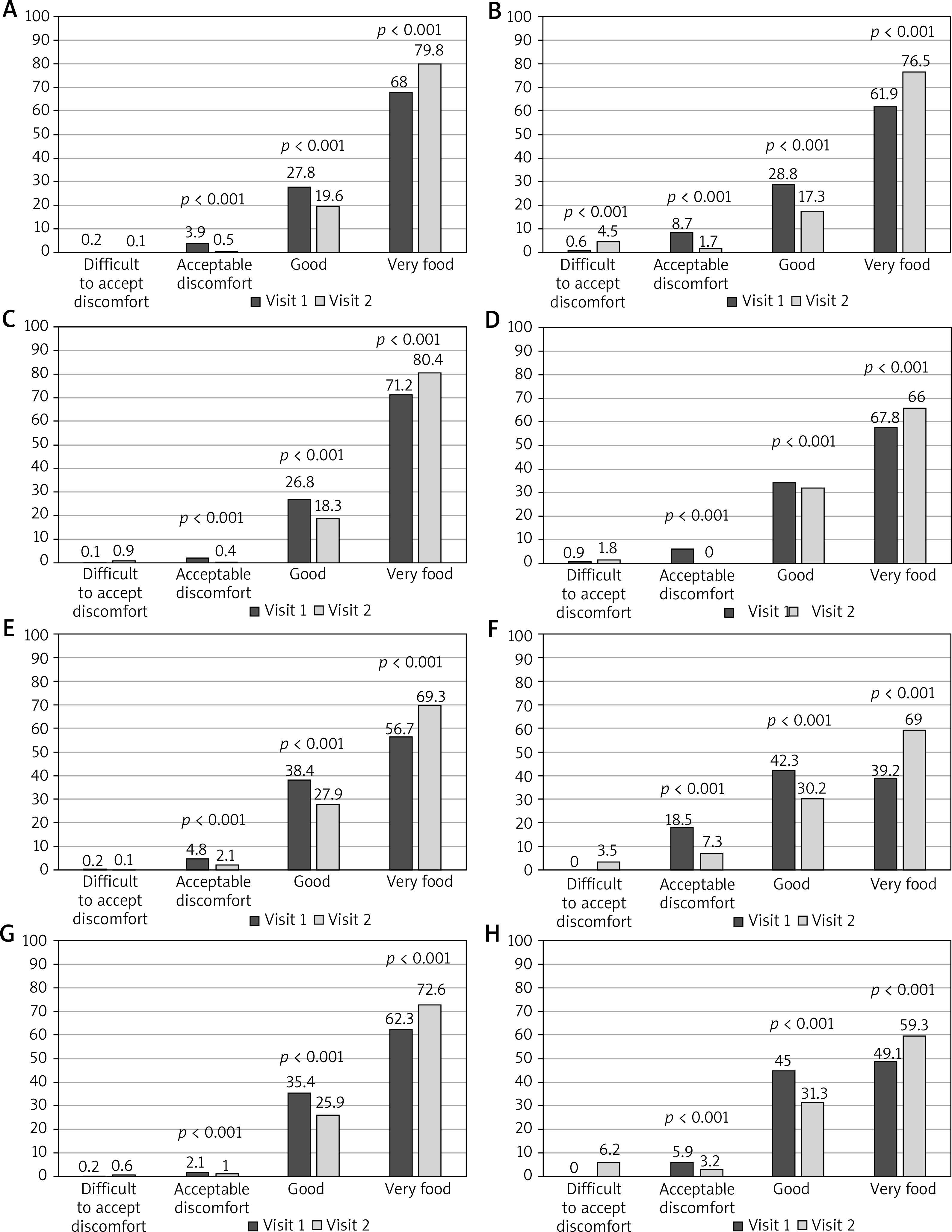
Similarly, during the observation in all patients with COPD, the tolerance of pharmacotherapy used and assessed as very good increased significantly (from 56.7% to 69.8%, p < 0.001). On the first visit, the percentage of patients with COPD who assessed the tolerance of pharmacotherapy used as very good was the highest among patients treated with formoterol and fluticasone (71.2%) and the lowest among patients treated with salmeterol and fluticasone (57.8%). In a subgroup with COPD on polytherapy with formoterol and fluticasone, the tolerance assessed as very good increased significantly (from 71.2% to 80.4%, p < 0.001), with formoterol and budesonide (from 61.9% to 76.5%, p < 0.001) and with salmeterol and fluticasone (from 57.8% to 66.0%, p < 0.001) – Figures 2 E–H.
Discussion
The presented study was the first large survey that assessed therapeutic preferences in the use of ICS and LABA polytherapy and its efficacy and tolerance in patients with asthma or COPD in daily clinical practice, performed in the Polish population. It should also be noted that so far such a study has not been conducted in other populations.
Over 80% of doctors who participated in this study declared that the most common ICS and LABA regimen in the treatment of asthma and COPD is a combination of formoterol with fluticasone. As the very important factors influencing the choice of this therapy for both asthma and COPD, the doctors most often reported its efficacy and safety.
The preferences and factors influencing the choice of medications declared by the doctors were reflected in the individual decisions made for the patients enrolled in the study. More than 70% of patients with asthma included in the study were using formoterol with fluticasone. Very important factors determining the choice of this therapy were efficacy and safety. Efficacy of polytherapy with formoterol and fluticasone was confirmed by results obtained in our study and showing a significant increase in the percentage of patients assessing it as very good. This percentage was increasing despite the therapeutic regimen used. However, it should be noted that on both visits the percentage of patients who assessed efficacy of treatment as very good was the highest among patients receiving polytherapy containing formoterol and fluticasone. During the observation, the percentage of patients who assessed the tolerance of pharmacotherapy used as very good increased significantly. However, the increase in the percentage of patients scoring the tolerance of treatment as very good was independent of the regimen used. Moreover, it should be noted that on both visits, the percentage of patients who assessed tolerance of the treatment as very good was the highest among patients treated with a combination of formoterol and fluticasone. Greater efficacy and safety of polytherapy with a combination of formoterol with fluticasone than formoterol with budesonide in patients with asthma as shown in our study, was also confirmed by the results of a randomized trial [6]. In addition, the efficacy and safety of combined therapy with formoterol and fluticasone was comparable to those found in clinical trials and also a non-interventional post-authorization observational study conducted in a group of over 2,500 patients with asthma [7]. In another non-interventional, post-marketing observational study, similarly to the presented survey, greater efficacy of polytherapy with formoterol and fluticasone was found compared to the therapy with formoterol and budesonide despite the lack of differences in the patients’ compliance with the recommendations [8]. It should also be emphasized that in the cost-effect assessment study, the change or initiation of a combination therapy with formoterol and fluticasone was associated with a better cost-effect ratio than treatment with a combination of formoterol and salbutamol [9].
Similarly to a group with asthma, the declarations of the doctor were also reflected in the therapeutic decision taken for patients with COPD. Over 80% of patients with COPD were treated with a combination of formoterol and fluticasone. Factors influencing the selection of a therapeutic regimen, indicated as the most important, were efficacy and safety. In accordance with these factors, during the observation a significantly increased percentage of patients with COPD assessed efficacy of the treatment used as very good regardless of the therapeutic regimen used. However, it should be noted that on both visits, the percentage of patients assessing the effectiveness of the treatment as very good was the highest among those treated with a combination of formoterol and fluticasone. Higher efficacy of polytherapy with fluticasone and formoterol than monotherapy with formoterol in the treatment of COPD was confirmed in a 12-month randomized trial involving nearly 2,000 patients [10]. The efficacy and safety of this therapy has also been confirmed by the results of a 52-week, randomized, double-blind phase III trial (EFFECT – Efficacy of Fluticasone propionate/FormotErol in COPD Treatment) [11].
In summary, our multicentre, open label, post-marketing observational study has shown that polytherapy containing formoterol and fluticasone is preferably used in the treatment of asthma and COPD by Polish general practitioners and specialists due to its efficacy and safety. Preferences of doctors were reflected in the prescription pattern shown in the study group.
The main limitations of our survey were a small number of participating general practitioners, subjective assessment of treatment efficacy and different duration of the use of current pharmacotherapy.
Conclusions
Formoterol and fluticasone polytherapy is frequently chosen in the treatment of asthma and COPD by Polish physicians due to its high efficacy and safety. In accordance with doctors’ declaration, in the study group this therapy was characterized by the highest effectiveness and the best tolerance.







