
Introduction
Atopic dermatitis (AD) is a chronic inflammatory skin disease that most commonly occurs in childhood, with as many as 45% of all cases reported to be manifested in the first 6 months of life [1]. The worldwide prevalence of AD has increased during the past three decades, and currently 10–20% of children are affected. AD prevalence in Indonesia reached 23.67%, which occurred in 65% of children before 18 months of age [2]. AD was reported to cause a significant negative impact on children’s quality of life, in addition to dealing with the medical aspects of the disease. Furthermore, because this is primarily a disease of childhood, family members, especially parents, are also affected by the condition [3].
Vitamin D is known to play a crucial role in the regulation of immune responses. Therefore, there was evidence connecting vitamin D to several allergic diseases, including asthma, allergic rhinitis, and food allergies [4]. It has also been reported that vitamin D contributes to the pathophysiology of atopic dermatitis (AD). Studies in recent years have reported an inverse relationship between vitamin D and AD [5, 6]. Vitamin D insufficiency and deficiency have an inverse correlation with AD. It has been suggested that a low level of vitamin D at birth is a risk factor for developing AD in the future [7]. Moreover, vitamin D supplementation given to children was reported to reduce the symptoms of AD [8–10]. However, several other studies showed contradictory findings [11]. There was no association between the vitamin D status and the prevalence or severity AD [12–14]. Although several studies reported the correlation between low vitamin D levels and disease activities in patients with AD, limited studies have evaluated cytokines or other immune parameters that contributed to the immune-regulation mechanism of vitamin D in AD.
Vitamin D regulates the action of several immune cells, such as monocytes, dendritic cells, and lymphocytes. It also regulates the integrity and function of epithelial cells, which are important in AD [15]. It has been reported that vitamin D could modulate T-helper type 2 (Th2) imbalance, Immunoglobulin E (IgE) production, and eosinophilia, which are the major features of AD [16]. A previous study showed that there was a significant reduction of the Scoring of Atopic Dermatitis (SCORAD) index and Th2 cytokines after vitamin D supplementation in children with AD [10]. With the increasing complexity in the immune mechanism of AD, other cytokines have also been identified as those that play a role in pathogenesis of AD. A new proposed mechanism was the role of T-helper type 17 (Th17) and T-helper type 22 (Th22) in AD, especially in infants. Infants showed different immune profiles compared to those in adolescents and adults [17]. Interleukin (IL)-17, which is produced mainly by Th17, was considered to serve as an initial cytokine source for the development of inflammatory responses in AD [18]. A study reported that vitamin D supplementation in patients with AD leads to a decrease in the number of CD4 T-cells producing IL-17 and improves the disease severity [19]. Th22 has also been identified as those that play a role in pathogenesis of AD, however limited data were available [20, 21]. There is an ongoing need to investigate the role of vitamin D on cytokine profiles in AD to understand its mechanism and for treatment purposes.
Aim
The aim of the study was to evaluate the correlation between 25(OH)D and immune profiles (IL-4, IL-17, and IL-22 cytokines, eosinophil count, tIgE serum levels) and also SCORAD index in infants with AD.
Material and methods
Research subjects
We enrolled 36 infants with AD aged ≤ 1 year, who visited the outpatient clinic of the Paediatric Department of Saiful Anwar Hospital, Malang, Indonesia. Exclusion criteria were active skin infection and the use of topical glucocorticosteroids/immunomodulators in the past 1 week and systemic immunosuppressants in the past 4 weeks. Before inclusion in the study, parents signed a written consent form approved by the institutional review board. This study was approved by the Ethical Committee of the Faculty of Medicine, Brawijaya University, Indonesia (237/EC/KEPK/10/2018).
Evaluation of disease severity
The disease severity of AD was evaluated by the SCORAD index. The SCORAD index consists of the extent of the disease (the affected area as a percentage of the whole body); the intensity, composed of six items (erythema, edema, papules, effect of scratching, oozing, crust formation, lichenification, and dryness); and two subjective symptoms (itch and sleeplessness). Using the SCORAD index, AD was classified as mild (< 15), moderate (15–40), or severe (> 40), as defined in previous studies [22].
Laboratory tests
Venous blood samples were drawn and sera were stored at –20°C after centrifugation, until testing. The levels of 25(OH)D were assayed using immunoassays (Cobas e400, Roche, Germany). Values were used as continuous variables and vitamin D amounts were also categorized, in a descriptive analysis, as follows: normal or sufficient, at least 30–40 ng/ml; insufficient, 20–30 ng/ml; and deficient, < 20 ng/ml [23]. Complete blood count was performed by a haematology analyser (Cobas m511, Roche) to evaluate the number of eosinophils. The total IgE (tIgE) serum level was measured using an immunoassay (Cobas e400, Roche). tIgE concentrations > 15 IU/ml were considered to be increased. The IL-4, IL-17A, and IL-22 serum cytokine levels were measured using enzyme-linked immunosorbent assays (LEGEND MAXTM Human ELISA Kit BioLegend, Inc).
Statistical analysis
Quantitative variables are expressed as the means ± standard deviation, or median values with interquartile ranges. Differences between groups were analyzed using the t-test or Mann-Whitney test. The correlation analyses were performed using Pearson’s or Spearman’s correlation tests. Path analysis was conducted by linear regression tests. All statistical analyses were performed using IBM SPSS Statistics, ver. 25.0 (IBM Corporation, New York City, USA); p-value of < 0.05 was considered statistically significant.
Results
Characteristics of subjects
Characteristics of the study subjects are shown in Table 1. Thirty-six infants with AD were enrolled in this study. The median of age was 6 months (range: 1–12 months). Subjects with mild AD (n = 19) presented a SCORAD value of 10.32 ±4.29 and subjects with moderate AD (n = 17) had a SCORAD value of 24.12 ±5.16. Among the subjects, vitamin D deficiency and insufficiency were found in 18 (50%) and 9 (25%) children, respectively. Only 9 (25%) children were found to have normal vitamin D levels. The mean serum 25(OH)D level was 21.32 ±11.83 ng/ml in the study subjects. From the immune parameters, we found that the median TEC was 0.32/mm3, tIgE was 8.40 IU/ml, IL-4 was 1.28 pg/ml, IL-22 was 152.43 pg/ml, and the mean ± SD of IL-17A was 6.30 ±1.56 pg/ml.
Table 1
Demographic, clinical, and laboratory characteristics of subjects
Comparison of vitamin D and immune parameters based on AD severity category
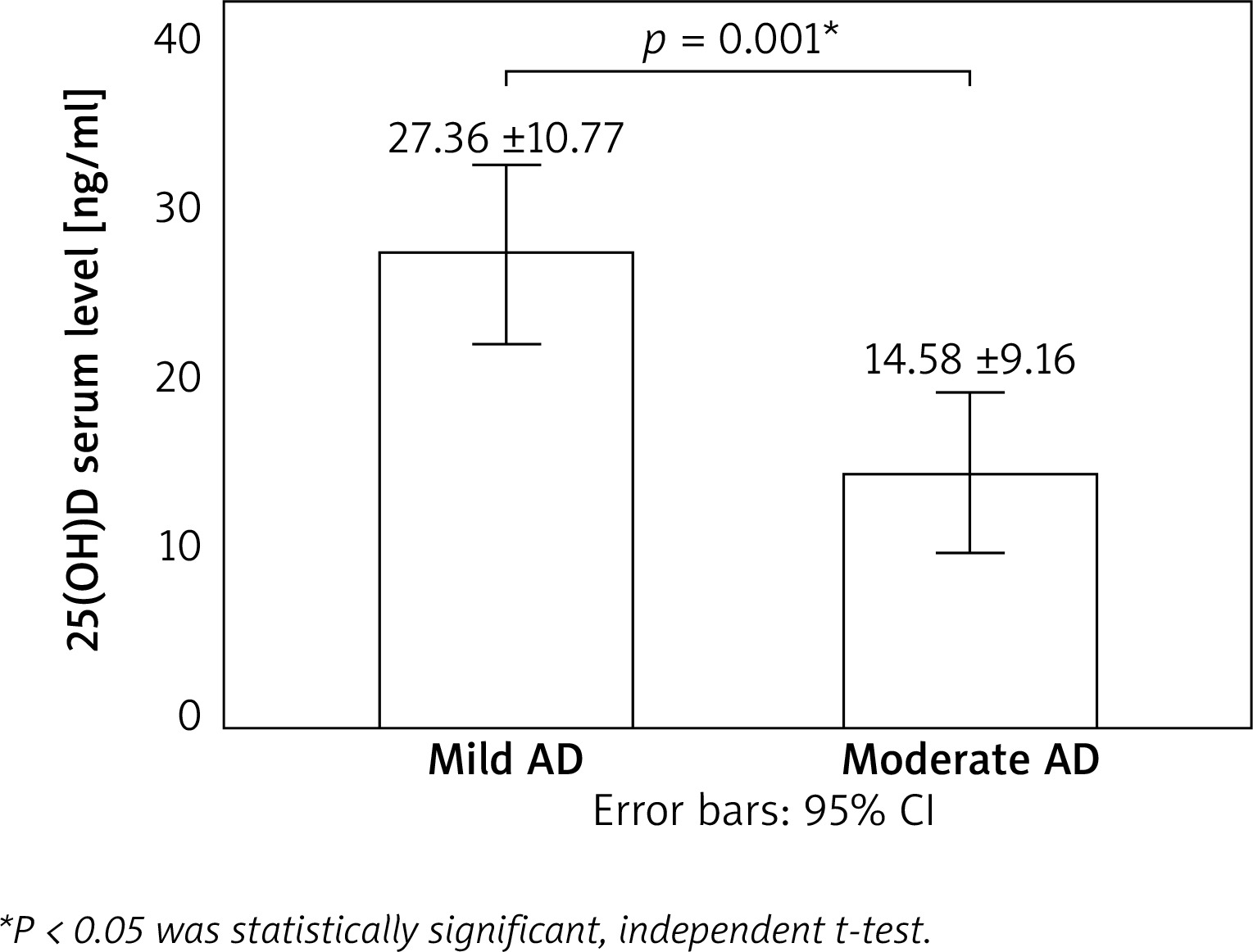
We classified the subjects into mild and moderate AD groups, based on the SCORAD index, and compared 25(OH) D serum levels between the groups (Figure 1). We found that the mean 25(OH)D level was significantly lower in the moderate AD group than in the mild AD group (p = 0.001). Mean 25(OH) D serum levels were 27.36 ±10.77 ng/ml in subjects with mild AD and 14.58 ±9.16 ng/ml in those with moderate AD. The serum level of IL-4 was found to be lower in the mild AD group than in the moderate AD group (p = 0.006). The IL-17A serum level was also decreased in the mild AD group compared to the moderate AD group (p = 0.003). Moreover, we reported that the IL-22 serum level was significantly lower in the mild AD group than in the moderate AD group (p = 0.006). In this study, we also evaluated the levels of TEC and tIgE in each subject. The mean TEC showed no significant difference in the mild and moderate AD groups (p = 0.601). The mean tIgE was also not significantly different among the groups (p = 0.862). The mean values of each cytokine and immune parameter are shown in Table 2.
Correlation between 25(OH)D, immune parameters, and disease activity
Table 3 shows the correlation between the 25(OH)D serum level, immune parameters, and disease activity. As can be seen, a significant inverse correlation (r = −0.315, p = 0.041) was found between the 25(OH)D serum level and IL-17A. The value of the 25(OH)D serum level was also correlated negatively with the SCORAD index (r = −0.714, p < 0.001). We found a positive significant correlation between IL-4 and IL-17A serum levels (r = 0.645, p < 0.001). Moreover, IL-17A was found correlated with the TEC and SCORAD (r = 0.351, p = 0.036; and r = 0.522, p = 0.001; respectively). There were no significant associations between the 25(OH)D serum level and IL-4 and IL-22 (r = −0.239, p = 0.160; and r = −0.221, p = 0.196; respectively). IL-4 was not correlated with the SCORAD index (r = 0.325, p = 0.053), but IL-22 had a significant positive correlation with the SCORAD index (r = 0.612, p < 0.001). No significant correlations were found between the TEC and IgE and the SCORAD index (r = 0.271, p = 0.110; and r = 0.058, p = 0.738; respectively).
Table 3
Correlation coefficients of variables representing 25(OH), immune parameters, and disease activity
| 25(OH) | IL-4 | IL-17A | IL-22 | TEC | tIgE | SCORAD | |
|---|---|---|---|---|---|---|---|
| 25(OH) | 1.000 | ||||||
| IL-4 | –0.239 | 1.000 | |||||
| IL-17A | –0.315* | 0.645** | 1.000 | ||||
| IL-22 | –0.221 | 0.319 | 0.259 | 1.000 | |||
| TEC | –0.303 | 0.091 | 0.351* | 0.031 | 1.000 | ||
| tIgE | –0.102 | 0.108 | 0.021 | 0.206 | 0.136 | 1.000 | |
| SCORAD | –0.714** | 0.325 | 0.522* | 0.612** | 0.271 | 0.058 | 1.000 |
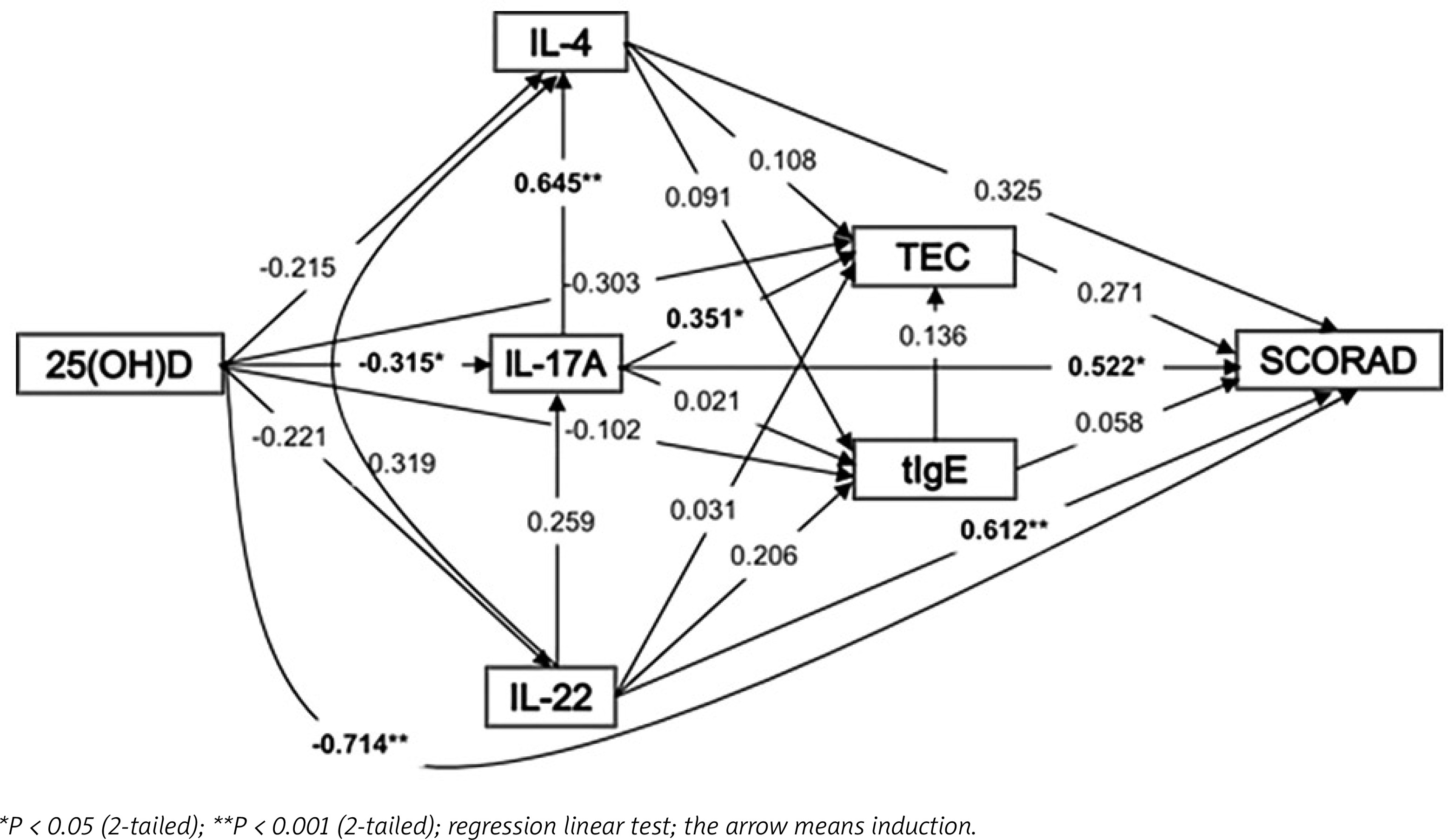
In this study, we also constructed a path analysis model that included all variables that contributed to the SCORAD index. From Figure 2, we can see that a lower level of 25(OH)D was correlated with a higher level of IL-17A and the SCORAD index. An increase in the IL-17A serum level was associated with increases in IL-4, TEC, and the SCORAD index. The SCORAD index was also increased with a higher IL-22 serum level.
Discussion
This study aimed to evaluate whether 25(OH)D levels were decreased in infants with AD, and whether 25(OH)D was related to the severity of AD. In addition, we investigated the correlation between IL-4, IL-17A, and IL-22, and the severity of AD. We found that the mean 25(OH)D serum level was decreased in our study subjects. There was a high prevalence of vitamin D deficiency (50%) and insufficiency (25%) in the study subjects. This study also showed that the mean 25(OH)D serum level was significantly lower in the moderate AD group than in the mild AD group. This is in agreement with previous studies on the vitamin D profile in AD. An insufficient level of vitamin D was found in 82% of children (32/39) with AD [7]. A study reported that serum levels of vitamin D were higher in patients with mild AD compared to those with moderate or severe AD [24]. Overall these data showed that a low level of vitamin D was related to the severity of AD.
A low level of vitamin D has been linked to various allergy and autoimmune diseases [1]. Previous studies reported that there was a high prevalence of vitamin D insufficiency in children with allergic asthma [25] and Juvenile Idiopathic Arthritis (JIA) [26]. This study also found that a low level of 25(OH)D correlated with the severity of AD. A study conducted on sixty Turkish children with AD reported that a low serum vitamin D level is inversely associated with severity of AD in children [27]. A similar study performed in India also reported a significant negative correlation between the vitamin D serum level and SCORAD [28]. A previous study conducted on Indonesian children suggested a moderate correlation between the serum 25(OH)D level and the SCORAD index in children with AD [29]. In addition, randomized, double-blind, placebo-controlled trials demonstrated that vitamin D supplementation given to children with AD showed a significant improvement in the SCORAD index [30]. However, several studies reported opposing results. A study on Brazilian children aged younger than 14 years reported that levels of 25(OH)D were deficient or insufficient in 85% of the children, but serum vitamin D concentrations were not significantly related to AD severity [31]. Several other studies showed contradictory findings, and there was no association between the vitamin D status and the prevalence or severity of AD [12–14]. Moreover, studies have reported that an increased intake of vitamin D during childhood was correlated with an increased risk of AD at 6 years of age [32] and that increased maternal serum levels of vitamin D predisposed infants to AD at 9 months of age [33]. Although there were different results, most of papers pointed out to vitamin D as a protective factor in AD. These controversial results could be explained by the dual-effects of vitamin D on in the immune pathogenesis of allergic skin. It has been suggested that both high and low vitamin D levels increased the risk of developing atopic dermatitis [4].
Vitamin D plays a key role in the immune responses. These mechanisms begin with the binding of 1,25(OH)2D to the vitamin D receptors (VDRs) that could regulate activation of several immune cells including phagocytes, T cells and B cells [34]. However, the possible mechanism of action of vitamin D on immune regulation in AD was variable. It has been reported that vitamin D could modulate Th2 imbalance and eosinophilia, which are the major features of AD. Th2 cells may play a pathogenetic role by producing and releasing cytokines relevant to allergic inflammation, such as IL-4, IL-13, IL-5, IL-31, and IL-10 [35]. A previous study showed that vitamin D deficiency could induce Th2 skewing and eosinophilia, and reduce T regulatory cells in allergic airway disease [36]. Another study reported a significant reduction in the SCORAD index by decreasing Th1 and Th2 cytokines (IL-2, IL-4, IL-6, interferon (IFN)-γ) after vitamin D supplementation in children with AD [9]. However, we obtained different results; there was no correlation between 25(OH)D and IL-4 in this study. The IL-4 serum level was also not associated with TEC, tIgE, and the SCORAD index.
It can be explained by the evidence that AD in infancy shows immune profiles different from those in young children and adolescents. Serum cytokine profiles show that there was no Th2 polarization in atopic infants, but that Th17 was dominant [17]. Our data showed that a lower level of 25(OH)D was correlated with a higher level of IL-17A. The IL-17A serum level was higher in the moderate AD group than in the mild AD group. The higher IL-17A serum level was correlated with the higher SCORAD index. Similarly, another study reported that oral vitamin D supplementation decreased the number of CD4+ T-helper cells producing IFN-γ and/or IL-17 pro-inflammatory cytokines and improves the clinical severity of AD [19]. Another possible explanation was that there was a distinction between intrinsic and extrinsic AD. Intrinsic AD is characterized by strong activation of Th17 and Th22 responses, shows normal IgE levels, and usually lacks a personal or family history of atopy. In contrast, extrinsic AD shows dominant Th2 response, increases in total and allergen-specific IgE levels, higher rates of eosinophils, and a family history of atopic diseases [37]. We found no correlation between 25(OH)D and IL-22 in this study. IL-22 also has no relationship with the SCORAD index; even though, the IL-22 serum level was higher in the moderate AD group than in the mild AD group. There are limited studies evaluating the role of vitamin D in IL-22 cytokines in patients with AD. Further studies are needed to confirm this results. In this study, we also reported that 25(OH)D was not correlated with tIgE and TEC. Furthermore, tIgE and TEC were not associated with the SCORAD index. In contrast, a study reported that the serum 25(OH)D level was inversely correlated with the SCORAD index and positively correlated with TEC and tIgE levels [22]. Vitamin D was also reported to have a negative correlation with serum tIgE levels, but there was no significant correlation between tIgE levels and the SCORAD index [27].
This is the first study that performed a path analysis model representing the interaction of vitamin D, cytokine profiles and disease severity in infants with AD. We found that 25(OH)D was inversely correlated with the SCORAD index, dependently on IL-17A cytokine. A low level of 25(OH)D was correlated with a higher level of IL-17A cytokine. Moreover, a higher level of IL-17A cytokine was associated with increased disease severity assessed by the SCORAD index. There was also an inverse correlation between IL-17A cytokine serum level and total eosinophil count but no correlation was found with IgE. The role of the IL-22 cytokine serum level in the SCORAD index was also reported in this study. There has been growing interest in studying the immune mechanism involved in AD with regard to both cellular and humoral immunity. Further research is needed to confirm this finding and explore the effects of vitamin D on the immune mechanism in AD.
Conclusions
This study concluded that there was a high prevalence of vitamin D deficiency and insufficiency in infants with AD and that a low level of vitamin D was correlated with the severity of AD, which was dependent on IL-17A. The limitations of our study were its small sample size and that it was conducted in a single centre. Therefore, further multicentre-based studies with larger groups of subjects are needed. Examination of vitamin D and cytokine profiles was not routinely performed in AD cases in our population. It might be due to the high cost and limited resources. However, understanding the role of vitamin D and cytokine patterns may open up good opportunities for mechanism-based therapeutic intervention in patients with AD.







