
Cardiac tumors are exceedingly rare, particularly those of a malignant nature. Among them, synovial sarcoma represents an uncommon malignancy, typically affecting soft tissues in the extremities. However, when synovial sarcoma involves the heart, it poses significant diagnostic and therapeutic challenges due to its rarity, aggressive nature, and non-specific clinical presentation [1–4]. In this case report, we describe a rare and intriguing instance of primary cardiac synovial sarcoma obstructing the pulmonary trunk, further complicated by metastatic spread to the lungs.
A man in his 50s presented to the emergency department with rapidly worsening shortness of breath, chest pain, and facial swelling. These symptoms, while indicative of cardiopulmonary compromise, are not immediately specific to malignancy, highlighting the challenges in diagnosing such rare cases. Initial evaluation with a transthoracic echocardiogram revealed a large obstructive mass involving the right atrium, right ventricle, and the tricuspid valve. Given the severity of the findings, further imaging was performed. A computed tomography (CT) pulmonary angiogram demonstrated a large lobulated soft tissue mass extending through the right atrium and right ventricular cavity, involving the right ventricular outflow tract, pulmonary trunk, and right main pulmonary artery (Figure 1). In addition to this primary cardiac mass, the scan also identified multiple rounded soft tissue nodules and masses in the lungs, strongly suggestive of metastasis (Figure 2).
Figure 1
Series of axial computed tomography images show a hypodense mass (arrows) in the right atrium and right ventricle involving the left ventricular outflow tract and extending in the pulmonary trunk and right main pulmonary artery. The images also reveal a metastatic soft tissue round lesion (asterisk) in the basal medial segment of the right lower lobe
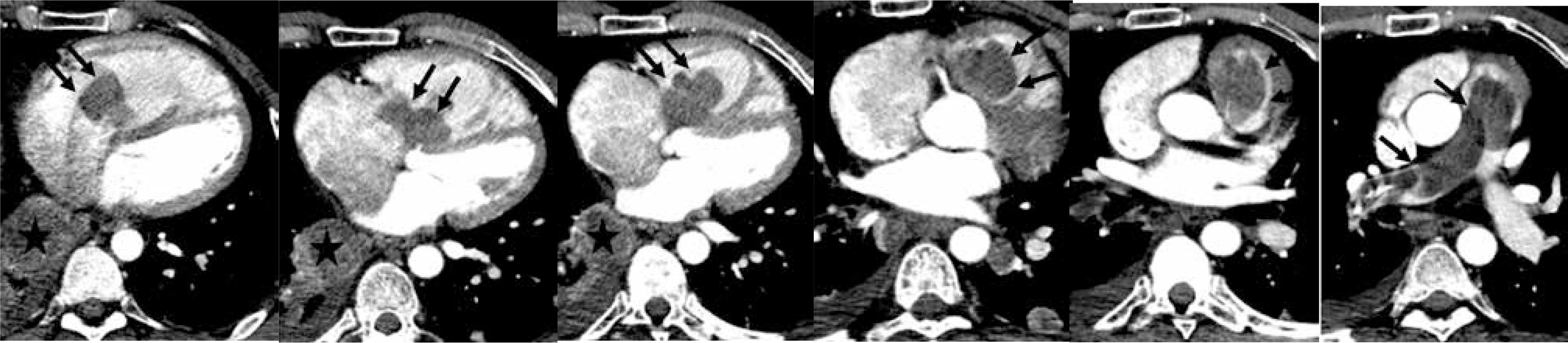
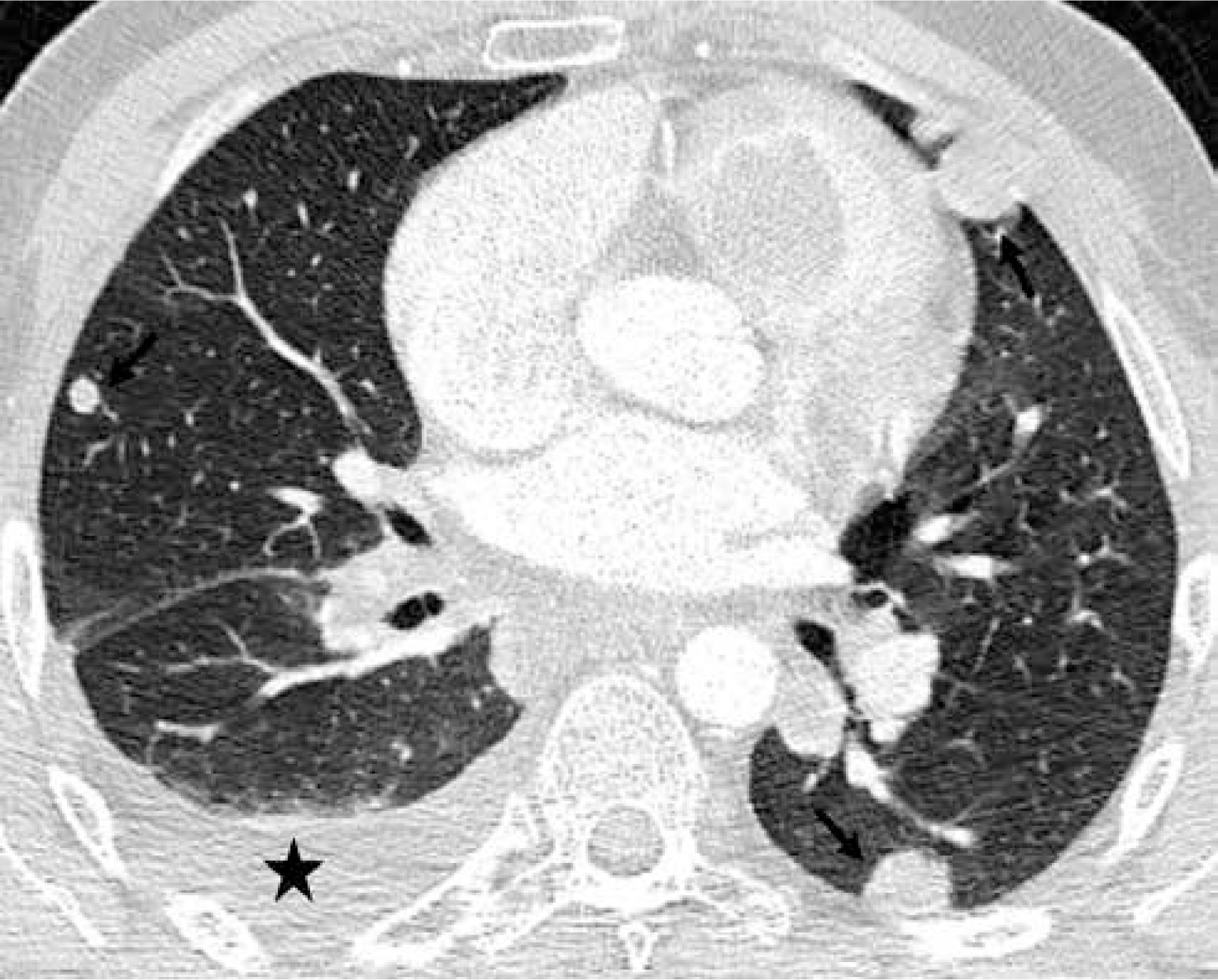
Figure 2
Axial computed tomography image show a few metastatic lung nodules (arrows) and a small right pleural effusion (asterisk)
To further investigate the nature of these lung lesions, a CT-guided biopsy of one of the metastatic nodules was performed. However, despite the technical success of the biopsy, the findings were inconclusive regarding the precise characterization of the tumor. This is not uncommon in cases of synovial sarcoma, where definitive diagnosis often relies on histopathological examination of the primary tumor. After a thorough discussion of the risks and benefits, and with informed consent, the patient underwent a complete surgical resection of the primary tumor, which was localized within the pulmonary vasculature.
Histopathological examination of the resected tumor revealed a biphasic synovial sarcoma, featuring both epithelial and spindle cell components. This histological subtype, though rare, is known for its aggressive nature and poorer prognosis compared to the monophasic variant. The patient was subsequently referred to the oncology department for adjuvant chemo-radiotherapy. Despite receiving appropriate treatment, the patient died 1 year later due to progressive metastatic disease, underlining the aggressive course of cardiac synovial sarcoma.
Primary tumors of the heart, including both benign and malignant types, are exceedingly rare, with an incidence of less than 0.1% in population studies [1]. The differential diagnosis of cardiac masses predominantly includes benign tumors such as myxomas, and less commonly, malignant tumors such as angiosarcomas, rhabdomyosarcomas, malignant mesotheliomas, and fibrosarcomas [1]. Synovial sarcoma of the heart is exceptionally rare, representing less than 0.1% of all synovial sarcomas [2]. These tumors are more likely to affect the right side of the heart than the left, with nearly twice the incidence in the right chambers [3]. Histologically, synovial sarcoma can exhibit two patterns: a monophasic spindle cell pattern or a biphasic pattern, the latter of which includes both glandular and spindle cell components [4].
The clinical presentation of cardiac synovial sarcoma is non-specific, often resulting in delayed diagnosis. Symptoms commonly include shortness of breath, chest pain, dyspnea, and, in advanced cases, signs of heart failure or embolic events. In this patient, the combination of shortness of breath, chest pain, and facial swelling pointed towards an obstructive process within the heart or pulmonary vasculature. Metastasis in synovial sarcoma, though uncommon, has been described in the literature [3], and to our knowledge, this is only the second reported case of lung metastasis from primary cardiac synovial sarcoma, likely caused by tumor emboli [5].
Diagnosis of cardiac synovial sarcoma is challenging and often begins with transthoracic echocardiography, which can detect cardiac masses but may not provide detailed information on the tumor’s characteristics or extent [6]. In this case, echocardiography was crucial for identifying the mass obstructing the right side of the heart, but further investigation with CT imaging provided more comprehensive details about the tumor’s size, location, and its metastatic spread. Magnetic resonance imaging (MRI) can also be valuable in assessing tumor extent and invasion of surrounding structures.
Complete surgical resection of the tumor, combined with adjuvant chemo-radiotherapy, remains the cornerstone of treatment for synovial sarcoma. However, the prognosis for cardiac synovial sarcoma remains poor, with the majority of patients succumbing to local recurrence or metastasis within a year [3]. In this case, despite the aggressive surgical and oncological management, the patient’s disease progressed rapidly, reflecting the aggressive nature of this malignancy. The rarity of cardiac synovial sarcoma, along with its non-specific symptoms, highlights the need for a high index of suspicion in patients presenting with unexplained cardiorespiratory symptoms.









