
In this case presentation, we describe a 61-year-old male patient who was admitted to our institute for comprehensive diagnostics to evaluate heart failure. The patient reported symptoms of rapid fatigue with minimal physical exertion, shortness of breath, and an inability to lie flat. These symptoms appeared approximately 4 months earlier. Echocardiography revealed a globally hypokinetic left ventricle with reduced systolic function (LVEF 28%), moderate to severe mitral regurgitation (MR +3/4), and mild to moderate tricuspid regurgitation (TR +1/2).
To evaluate the presence of coronary artery disease, coronary angiography was performed, revealing an anomalous origin of the left coronary artery (LCA) from the right coronary sinus (RCS), with no significant coronary artery disease. Given that the LCA typically originates from the left coronary sinus (LCS) and branches into the left anterior descending (LAD) and circumflex arteries (Cx), while the right coronary artery (RCA) arises from the RCS, coronary computed tomography angiography (CCTA) with electrocardiographic gating was performed to precisely diagnose the anomalous coronary artery origin. It was performed using a Siemens SOMATOM Definition Flash 128-slice Dual-Source CT scanner, in the diastolic phase of the heart. During the scan, 90 ml of Omnipaque contrast agent was administered, followed by 75 ml of saline solution. The multiplanar and three-dimensional images of the coronary arteries did not show significant stenoses. Unlike standard coronary angiography, the CCTA revealed a double anomalous origin of the LAD and the Cx. The LAD and Cx independently originate from the RCS. The LAD originates above the RCA and follows a preaortic, partially intramyocardial course (myocardial bridging), which represents a malignant anomalous course. The Cx originates at the same level as the RCA and follows a retroaortic, non-malignant course, giving rise to a branch that supplies the ramus intermedius (RIM) vascular territory (Figure 1).
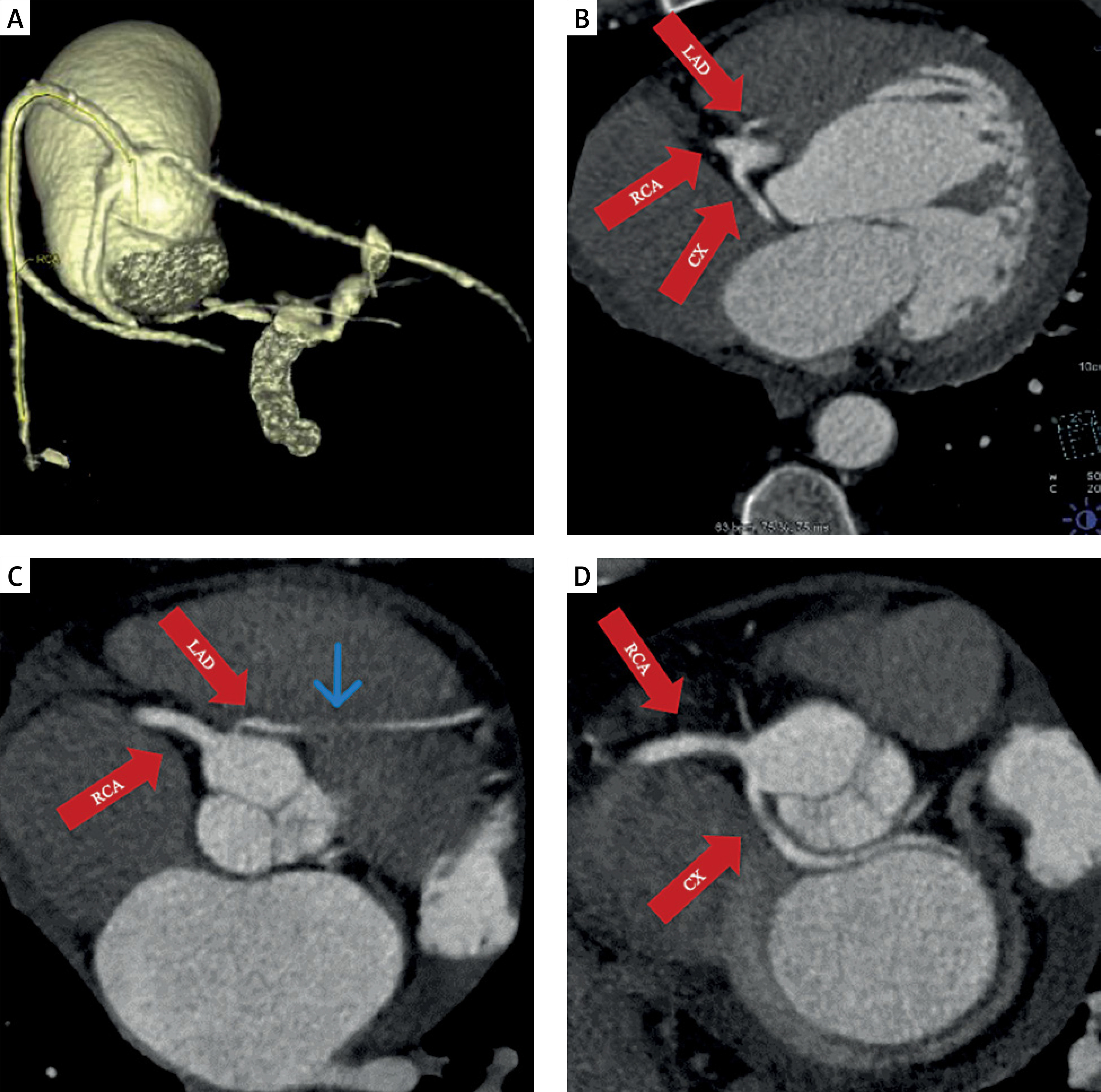
Figure 1
A, B – The separate origin of all three coronary arteries from the right coronary sinus. C – Anomalous origin of the LAD coronary artery, which arises at a sharp angle and courses preaortically (malignant anomalous course) with a partial intramyocardial trajectory (blue arrow). D – Anomalous origin of the Cx, which follows a retroaortic course (non-malignant anomalous course)
Although coronary artery disease was ruled out in our case, due to the malignant course of the LAD artery, the patient was diagnosed with dilated cardiomyopathy (DCM), with the possibility of an ischemic etiology. Various studies have shown that patients with malignant coronary artery courses are at an increased risk of SCD due to myocardial ischemia, which consequently can lead to chronic ishemic DCM [1].
Since the anatomy of the coronary arteries, as well as other cardiac structures, can greatly assist us in the diagnosis of our patients, it is essential to approach it with great attention and precision [2]. Given the less invasive nature of CCTA compared to coronary angiography, as well as greater patient comfort and lower risk of complications, along with the ability to achieve 3D visualization of the coronary arteries, it is important to emphasize the significance of CCTA in the timely diagnosis of coronary anomalies and its role in assessing the need for surgical intervention. Our case is distinguished by the simultaneous occurrence of dual coronary artery anomalies, specifically anomalous origins of the LAD and Cx arteries. Furthermore, the LAD demonstrated a malignant, interarterial course with a muscular bridge, thereby predisposing the patient to a heightened risk of SCD.







