





Intravenous fluid administration is a vital component in the resuscitation of critically ill patients [1]. Previously the clinical practice guiding the choice of fluid used in resuscitation has been predominantly governed by the opinion of the treating physician [2]. However, over the past decade there have been a variety of publications on this matter that can assist in guiding the treating physician [3–6]. In 2012, two landmark studies were published against the use of hydroxyethyl starches (HES) [3, 4]. The 6s study group found that when comparing resuscitation using HES versus resuscitation using acetated Rin-gers in patients with severe sepsis, those who were resuscitated with HES had an increased risk of death and were more likely to require renal replacement therapy [3]. Similarly, the CHEST study group found that when comparing HES use versus saline in intensive care patients, those resuscitated with HES were more likely to require renal replacement therapy [4]. During 2017 and 2018, two new studies then brought further advancement in the choice of fluids. SALT-ED and SMART were published reviewing the use of balanced crystalloids versus saline in the non-critically ill and critically ill respectively [5, 6]. Both found some benefit in the use of balanced crystalloids over saline [5, 6]. These studies have therefore led many to believe that balanced crystalloids are the most cost-effective and safer resuscitation fluid when compared to colloids or normal saline [1, 3–6]. A balanced fluid has previously been defined as one whose strong ion difference is at least 24 meq L-1 and whose chloride level is no more than 110 mmol L-1, e.g. lactated Ringers, PlasmaLyte [7].
Despite this available research, actual integration into clinical practice is often delayed [8]. With the growing amount of medical research available to healthcare professionals the research-practice gap has become more apparent [8]. When studied, findings show that it can take even more than a decade for research to be implemented into clinical practice, and so despite the above evidence being available to clinicians, we are unsure how this has translated into clinical practice [8].
The aim of our study was therefore to determine whether evolving international evidence has impacted resuscitative fluid practices in the Emergency Department (ED) and the Intensive Care Unit (ICU) in a tertiary hospital in South Africa.
METHODS
The study design was two-fold: a cross-sectional physician survey and a retrospective longitudinal observational study of the pharmacy fluid purchase records. The study took place at a tertiary academic hospital in Johannesburg, South Africa. Ethics clearance was obtained from the Human Research Ethics Committee (Medical) at the University of the Witwatersrand (M190869). The requirement for written informed consent to partake in the study survey was waived by the ethics committee.
Cross-sectional physician survey
A prospective, anonymous survey was circulated amongst consultants, registrars and medical officers with four years’ work experience reviewing resuscitative fluid choices in four clinical scenarios over two different time periods, their opinion on whether their choices had changed and possible reasons for the change. The four different clinical scenarios were: hypovolaemic shock, haemorrhagic shock, septic shock and shock of unknown origin. Physicians were asked their current resuscitative fluid choice and what they would have chosen 4 years prior.
The departments surveyed were the general ICU and the Medical Emergency Unit (MEU), the Surgical Emergency Unit (SEU) and the Trauma Emergency Unit (TEU), which together formed the combined ED. The ICU is a multi-disciplinary ICU accepting patients from all the emergency units included in the study.
Retrospective longitudinal observational study: fluid purchase records
Data were extracted from the pharmacy department’s purchase database from November 2014 until November 2018 for the ED and the ICU.
The following periods were used:
2015: 1 November 2014 – 31 October 2015; 2017: 1 November 2016 – 31 October 2017; 2018: 1 November 2017 – 31 October 2018,
2016: 1 November 2015 – 31 October 2016 was removed due to missing data.
The following fluids were chosen for review: 500 mL of starch-based colloid (Voluven, Fresenius Kabi, South Africa), 500 mL of gelatine-based colloid (Gelofusine, B Braun, South Africa), 1000 mL of 0.9% sodium chloride 1000 mL (sodium chloride 0.9%, Adcock Ingram, South Africa) (NS), 1000 mL of lactated Ringers (Ringer-Lactate Adcocare, Adcock Ingram, South Africa) (RL), 1000 mL of PlasmaLyte (SABAX Plasmalyte B, Adcock Ingram, South Africa) (PlasmB).
In our setting the administration of 20% albumin is a specialist led decision requiring motivation and seldom prescribed outside of the ICU. Given these conditions we opted to exclude albumin from our study.
Fluid amounts for crystalloids refer to litre bags and those for colloids refer to half litre bags.
All comparisons were between 2015 and 2018 except for cost, where the most recent period (2018) was compared with the average of the earlier pe-riods (2015/2017). All costs are noted in South African Rand in 1000s and taken to the first decimal place.
Outcomes
Statistical analysis
All percentages and proportions were compared using the chi square test. When necessary, percentages were taken to the second decimal place to ensure statistical completeness. The estimated number of doctors eligible to take the survey was 110. For a 95% confidence interval, with a 5% margin of error, ideally 86 surveys were to be completed.
RESULTS
81 doctors completed the survey: 61 from the ED and 20 from the ICU. 69 met the inclusion criteria, 51 from the ED and 18 from the ICU. The reasons for exclusion in all cases were doctors that had less than four years’ work experience.
Primary outcome: Cross-sectional physician survey
Figure 1 describes the resuscitative fluid choices doctors made over the different time periods in the different hypothetical scenarios.
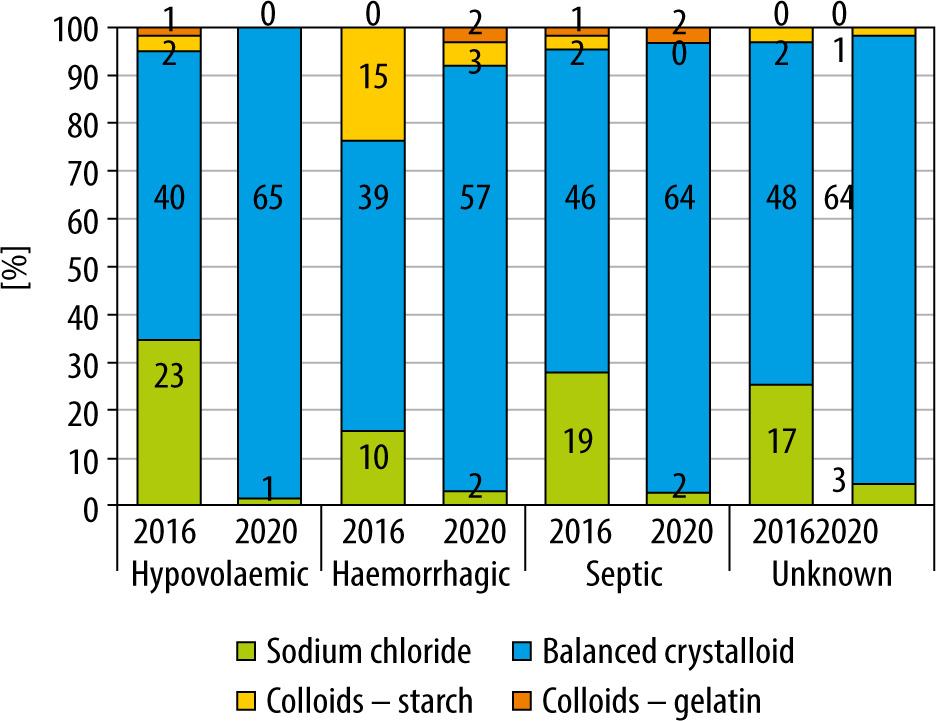
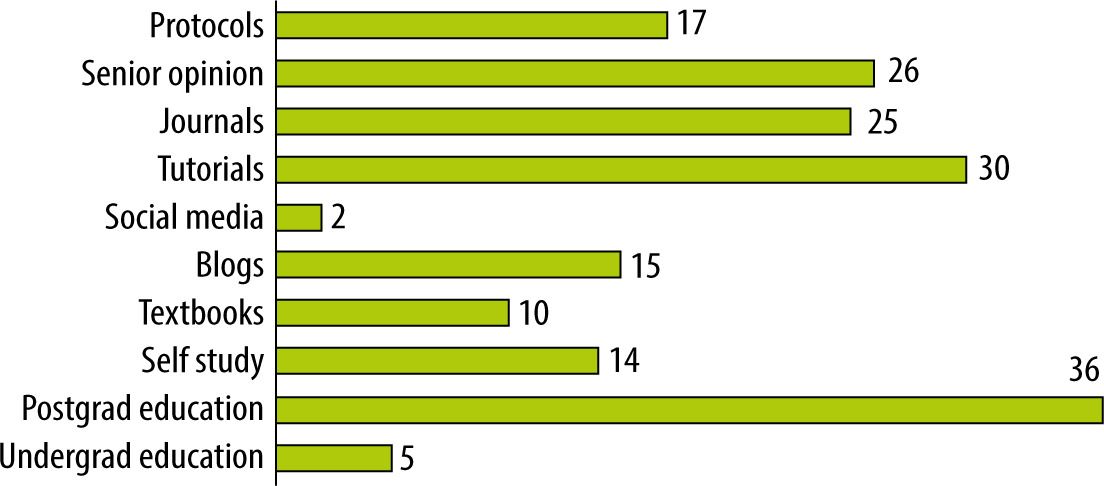
In 2020 a doctor was 8.3 times more likely to choose a balanced crystalloid for resuscitation regardless of the clinical scenario over any other fluid (CI: 5.0–13.8). 55% of doctors surveyed agreed that their resuscitation fluid of choice had changed for a variety of reasons as seen in Figure 2.
Primary outcome: retrospective longitudinal observational study
Table 1 presents the amount and costs of fluids purchased by the ED and the ICU, while Figure 3 presents the proportions of fluids purchased by both departments.
TABLE 1
Resuscitative fluid bags (Rand costs in 1000s) purchased by Emergency Department (ED) and the Intensive Care Unit (ICU)
FIGURE 3
Proportion of resuscitative fluids purchased by the Emergency Department (ED) and the Intensive Care Unit (ICU)
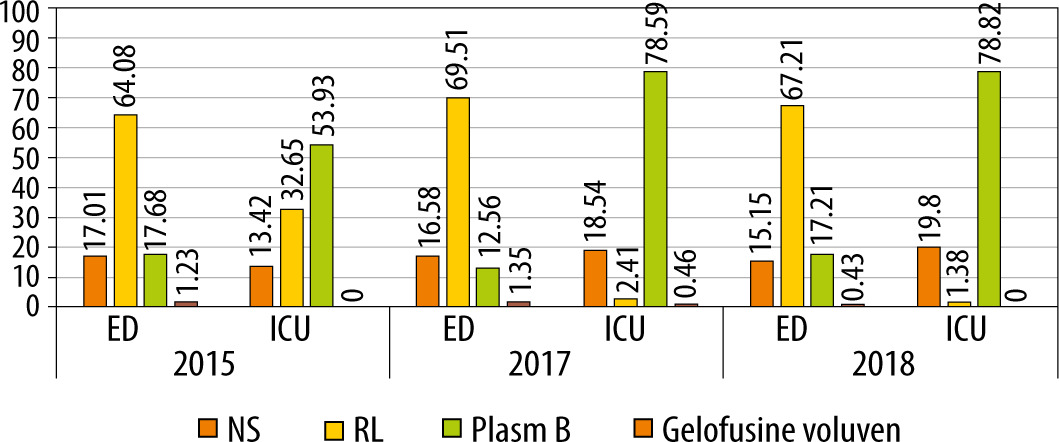
Table 2 compares the annual spend on resuscitative fluids by the ED and the ICU from 2018 to the average of the earlier two periods.
Secondary outcomes
When comparing the proportion of colloid and crystalloid orders in the ED, there was a statistically significant reduction in colloid orders from 368 units in 2015 to 140 units in 2018 (P < 0.0001, χ coefficient 121.1). The ICU had no colloid orders for the same period.
When comparing the proportion of unbalanced and balanced crystalloid to total crystalloid orders, the baseline level of balanced crystalloids was already 83% in the ED in 2015. The percentage increased to 85% in 2018. Normal saline levels dropped from 17% to 15% (P < 0.0001, χ coefficient 45.78). Lactated Ringers was the main balanced crystalloid ordered by the ED in 2015 and 2018 with levels staying mostly constant throughout the two periods (P = 0.0005, χ coefficient 11.89).
In the ICU however, the proportion of normal saline was observed to increase from 13% in 2015 to 20% in 2018 (P < 0.0001, χ coefficient 218.2). When reviewing the balanced crystalloids, PlasmaLyte was already the favoured ICU balanced crystalloid in 2015 at 62%, which rose to 98% in 2018 (P < 0.0001, χ coefficient 5530).
DISCUSSION
The main finding of our survey is that a doctor was 8 times more likely to choose a balanced crystalloid for resuscitation in 2020 compared to four years prior, irrespective of the clinical scenario faced. This is following almost a decade of emerging research in balanced fluids [5, 6, 9]. In all patient scenarios, the use of saline was markedly reduced by 2020, with the most notable change found in the hypovolaemic shock scenario. More than 30% of doctors would have chosen to resuscitate a hypovolaemic shocked patient with saline in 2016, while less than 2% would still make that choice in 2020. Resuscitation with colloids was already an unpopular choice in the 2016 scenario. The largest use of colloids at that time was in the scenario of haemorrhagic shock, where just over 20% of doctors would have chosen to resuscitate with a colloid. By 2020 however, less than 8% of doctors would still make the same choice.
In 2016, an international study was published in which doctors were surveyed on their fluid choices [10, 11]. A BMJ article surveyed emergency medicine physicians and intensive care physicians on their fluid choices in a septic shock patient [10]. As found in our survey, crystalloids were the most popular choice overall. 53.1% chose saline often/always as their first line of fluid, while lactated Ringers was chosen by 60.5% [10]. In comparison, in our septic shock scenario in 2016, just over 70% of doctors chose to resuscitate with a balanced crystalloid while 25% chose to use saline. This possibly indicates a possible more rapid uptake of balanced crystalloid use locally compared to the countries in the BMJ survey (Canada, UK, Scandinavia, Saudi Arabia). Possible reasons could be that our study took place at a single tertiary centre while they had multiple international centres. With regards to the utilisation of a starch-based colloid in septic shock, 3% of our cohort chose this option compared to only 1% in the BMJ group [10].
We noted that education played a major role in the change of fluid choices from unbalanced crystalloids and colloids to balanced crystalloid, with almost all doctors (96%) citing post-graduate teaching and/or tutorials as their reason for change. This highlights the importance of ongoing practical education in the medical field. Conversely, undergraduate teaching was one of the least common reasons for change. Kristensen et al. [8] found when reviewing the experience of healthcare professionals on implementing research into clinical practice that the healthcare professionals experienced no formalised procedures or established workflows in the implementation of research. The actual implementation of research was experienced to be at random as senior physicians “passed it on” to junior doctors [8]. This may account for the findings in our study with post-graduate teaching and tutorials forming the majority reason for change.
The use of clinical guidelines is described as an important method in implementing research into clinical practice [11]. In our study the use of protocols was ranked 5th behind post-graduate teaching, tutorials, senior opinion, and journal articles. This may indicate that there is an opportunity to implement medical research through the greater use of integration into clinical guidelines.
Changes in fluid utilisation may be represented by what fluids we are purchasing for resuscitation. From our pharmacy purchase order data, we found that balanced crystalloids were by far the most popular fluid purchased. We can see that already from 2015 the majority type of fluid purchased was a balanced crystalloid in both the combined ED (82%) and the ICU (87%), reflecting the survey findings above. In the combined ED, lactated Ringers was the favoured balanced crystalloid purchased, while in the ICU it was PlasmaLyte. Among balanced fluids the benefit of one buffer over another (bicarbonate and lactate) has not been studied. A possible reason for the differing utilisation rates between the ED and ICU could be the higher cost of PlasmaLyte. A comparison of the exact composition of the balanced crystalloids used in our study can be found under Appendix A. Notably, they have very similar concentrations of sodium, chloride and potassium. Subtle difference do exist between the two. Lactated Ringers contains calcium whereas PlasmaLyte contains magnesium. The pH of the lactated Ringers used is lower than that of PlasmaLyte at 6.5 vs. 7.4, although the calculated strong ion difference (SID) of these fluids is, for practical purposes, the same (25.8 vs. 25.5). However, lactate is a strong ion and anion, and therefore if it accumulates it will have an effect on the patient’s metabolic state and the strong ion difference will drop to below zero [12, 13]. Patients in whom this accumulation could occur include those suffering from severe liver failure, septic shock, treatment of septic shock with adrenaline and shock with ischaemic hepatitis [13–15]. If the SID of fluid is less than that of plasma then that will cause a drop in pH which will be proportional to the SID and the volume administered [12].
It is also clear that by 2015 the colloid use in the ICU had already declined, with no gelatine-based colloids ordered throughout the study period and only one order of starch-based colloid in 2017, forming less than half a percent of the total fluids ordered. This suggests that the critical care physicians were already following the recommendation, published by the European Medical Agency in 2013, that hydroxyethyl starches not be used in critically ill patients due to growing safety concerns [16]. In comparison, there were more colloids purchased by the combined ED although in declining amounts, with only 1.23% of fluids ordered in 2015. This could possibly be explained by use in the acute trauma patient subset. A local study published out of Cape Town found that there was improved lactate clearance in patients suffering from penetrating trauma when resuscitated with hydroxyethyl starch compared to normal saline [17]. This may account for the persistent utilisation of the colloids in the ED, although by 2018 the proportion of colloids purchased had fallen to less than 1% following the trend of international research [3, 4].
The amount of normal saline purchased by the ICU was observed to increase over the study period under review. This goes against international data showing increased harm with normal saline infusion versus balanced crystalloid infusion in the critically ill as well as the findings in our survey [6]. After investigation, it was found that due to the lack of commercial dialysate availability, normal saline had been used as part of a dialysate in the unit, and therefore increased utilisation may be linked to use during renal replacement therapy of patients and not as an intravenous therapy.
South Africa is currently classed as a middle-income country with just over half the population living below the poverty line [18]. Therefore, cost-effective spending is an important consideration in the South African health sector. In the annual cost comparison of fluid spend from the ED, the annual amounts stayed mostly stable despite an increase in crystalloid purchase. This is most likely due to the declining amounts of colloids purchased as the cost per unit of colloid is much higher than that of the crystalloids. In the ICU, however, the increased purchase of PlasmaLyte over time was responsible for a marked increase in annual spend despite the lack of colloid orders, as the cost of PlasmaLyte is almost three times that of lactated Ringers.
We did not adjust colloid cost for bag size in our study data. There is wide variation in the quoted effect of colloid to cause intravascular expansion when compared to a crystalloid, ranging from 1.3 to 1.12 [2, 3]. Regardless of the actual number, in all texts it is believed that less colloid is required to cause the same clinical effect when compared to a crystalloid [1–3]. For this reason, and for simplicity, we did not adjust absolute cost, and we may have therefore underestimated the cost of colloid use.
LIMITATIONS
Despite multiple attempts to gather data there were only 69 surveys received that met the inclusion criteria, meeting the 95% confidence interval with less than an 8% margin of error. The number of doctors working less than 4 years in the departments was underestimated and therefore the number of doctors eligible to take the survey was over-estimated. Additionally, once the COVID-19 pandemic gained traction in South Africa, all Academic Meetings by the departments involved were moved to an online platform, which was not accounted for in the initial study design.
Additionally, there were surveys in which the participants chose more than one answer when only one was required. For analysis, those questions were excluded, although other correctly answered questions in the survey were still analysed, therefore reflecting the different total tallies in the scenario’s questions.
Purchase data were used as a surrogate for actual fluid utilisation and may not correlate, although previous research shows that purchase data may mirror international utilisation trends [19].
Although patient profiles would be very useful, we were unable to comment on specific clinical characteristics as our study only evaluated the pharmaceutical purchase records. Due to the way in which the fluids were ordered for the combined ED, we were unable to review the separate amounts of fluids by each ED subsection and therefore were unable to make correlations with the type of patients seen.
As mentioned previously, the use of intravenous albumin is rarely prescribed outside of the ICU and therefore was excluded from our study, and we were unable to comment on the change in albumin utilization.
CONCLUSIONS
Our study showed that doctors working in a tertiary hospital in South Africa are following the trend of current evidence by using a balanced crystalloid as their resuscitation fluid of choice. Due to the research-practice gap, variations in the uptake of balanced crystalloid utilisation occur globally. Changes in fluid utilisation may have significant cost implications which need consideration.