
Coronary artery dissection (CAD) is a common phenomenon following balloon dilatation in percutaneous coronary intervention (PCI) [1]. While most CAD can be managed safely, it is challenging to manage CAD accompanying longitudinal hematoma. Except for using a cutting balloon to make a re-entry [2], full-cover stenting until the end of hematoma is a standard strategy, because an uncovered hematoma would cause ischemia [3]. Although the development of the guide-extension catheter made full-cover stenting easy in most cases [4], it is technically impossible to perform full-cover stenting when a longitudinal hematoma extends to the far distal part of the coronary artery.
A-72-year-old man with effort angina underwent PCI to the stent distal lesion of the left anterior descending artery (LAD) (Figure 1 A). He received a 2nd generation drug-eluting stent (DES) (2.5 × 18 mm) to the LAD 3 years ago. In PCI, intravascular ultrasound (IVUS) revealed that the target was around the distal edge of the previous stent. We performed pre-dilatation using 2.0 × 15 mm ScoreFlex NC (Orbusneich, Hong Kong, China) (Figure 1 B), and then inflated the 2.0 × 15 mm Sequent Please Neo (B. Braun, Melsungen, Germany) with 6 atm. Suddenly, the patient complained of chest pain with ST-segment elevation in leads V2-6. Angiography showed slow flow in the distal part of the LAD. IVUS revealed CAD (Figure 1 C) accompanying longitudinal hematoma (Figure 1 E). Because the longitudinal hematoma extended to the far distal part of the LAD, we abandoned the full-cover stenting strategy, and decided to apply a stent to cover the entry point of the CAD. We deployed a 2.0 × 26 mm Resolute Onyx stent (Medtronic, Dublin, Ireland) to make an overlap with the previous stent (Figure 1 F). Since the injection of contrast medium would exacerbate dissection, stent implantation was performed without contrast medium. After stent placement, the ST elevation gradually resolved, and the chest pain also improved. IVUS after stent implantation confirmed the expansion of the deployed stent and the uncovered hematoma in the distal segment of the LAD. After watchful waiting for more than 15 min in the catheter laboratory, we closed the PCI without final angiography. We confirmed no elevation of creatine kinase or creatine kinase muscle brain during the following days. The patient was discharged on day 6 without any complications. One month after the PCI, angiography showed excellent coronary flow (Figure 1 G).
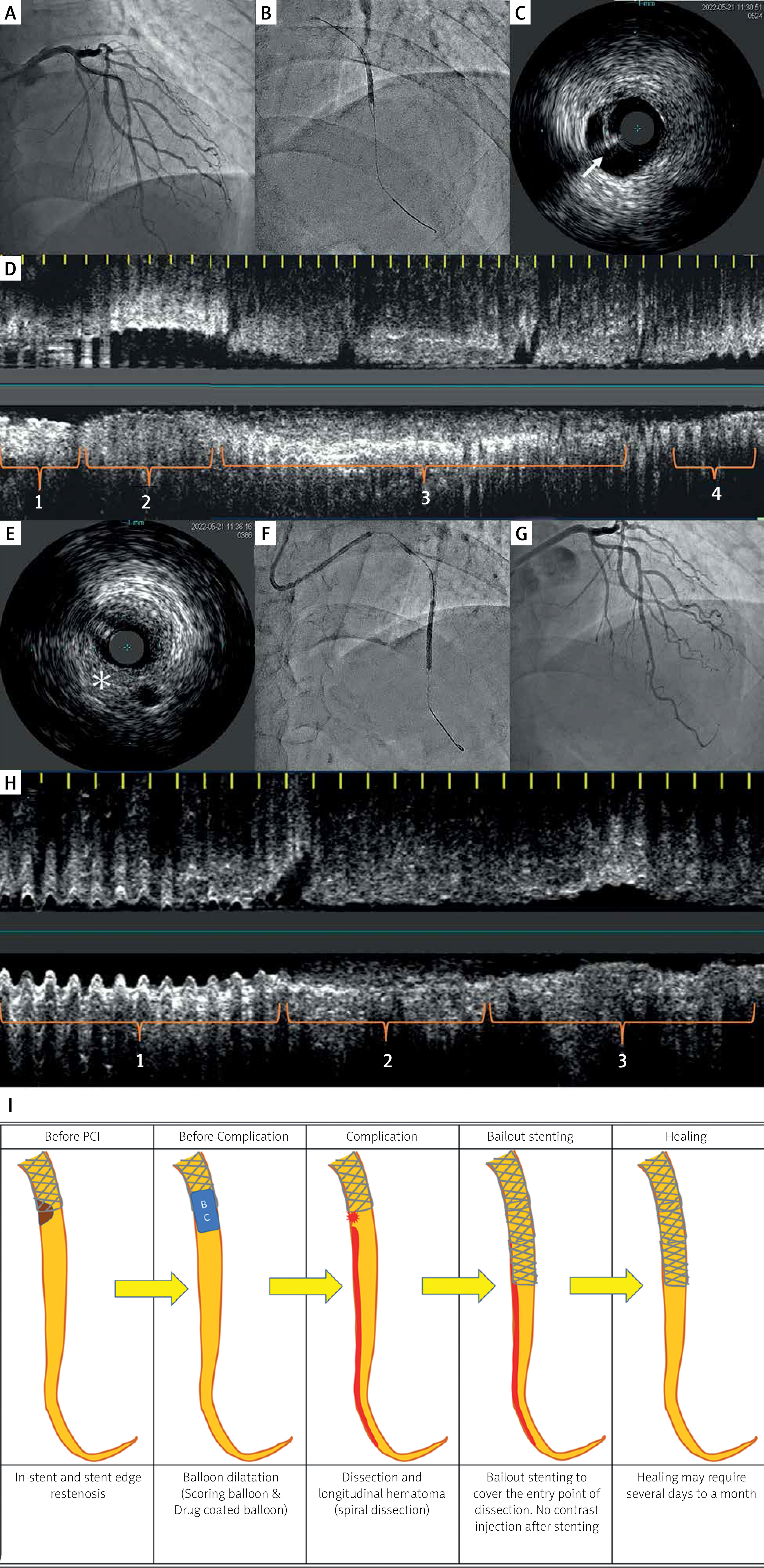
Figure 1
A – Coronary angiography before PCI. B – Balloon dilatation using 2.0 × 15 mm ScoreFlex NC. C – IVUS shows CAD (white arrow) near previous stent edge. D – Longitudinal IVUS just after CAD. 1 – Part of previous stent. 2 – Part of CAD. 3 – Part of longitudinal hematoma. 4 – Part of healthy vessel. E – IVUS shows hematoma (*) at the distal segment of the LAD. F – A 2.0 × 26 mm Resolute Onyx to cover the entry of the CAD. G – One month after the PCI, angiography showed excellent coronary flow. H – Longitudinal IVUS after the additional stent placement. 1 – Part of additional stent. 2 – Part of residual hematoma. 3 – Part of healthy vessel. I – Summary illustrations of the present case
Our bailout strategy for CAD accompanying longitudinal hematoma was entry-cover stenting without following contrast injections (Figure 1 F). The theoretical background to our bailout strategy is that the residual hematoma would diminish spontaneously in several days to a month if the entry site of the CAD was closed by a stent [5]. Although our reason for additional stenting was to cover the CAD entry site, we used a relatively long (26-mm) stent, because the CAD entry site was not clearly identified. Furthermore, ischemia would not exacerbate after entry-cover stenting unless we injected contrast media after stenting. In the comparison of full-cover stenting until the end of hematoma, our bailout strategy has the following advantages. First, the risk of side branch compromise would be lower in the entry-cover stenting than in the full-cover stenting. Second, it would be easier to bring a stent to the target lesion in the entry-cover stenting than in the full-cover stenting. On the other hand, our bailout strategy requires IVUS and watchful waiting. We also need to accept the risk of skipping final angiography (i.e. we may miss minor vessel perforation by guidewires). Moreover, if the entry-cover stenting could not restore coronary flow at the longitudinal hematoma, the bailout options are very limited. Therefore, if the operators could find an appropriate distal margin, initial stenting of the distal margin would be a safer approach to prevent downstream dissection propagation. However, if the operators could not find an appropriate distal margin, entry-cover stenting is a reasonable option.
In conclusion, entry-cover stenting without following contrast injections can be a bailout strategy for CAD accompanying longitudinal hematoma, especially when full-cover stenting is technically difficult.







