
Infective endocarditis (IE) is a serious, life-threatening disease that can lead to severe damage to the heart valves, which may require surgical treatment [1]. Heart failure as a complication of IE is independently associated with poor survival in the hospital, and surgical treatment is the only effective treatment associated with improved survival [2].
We present the case of a 79-year-old woman with endocarditis of a previously implanted prosthetic valve (Hancock II, 23 mm) who was multimorbid, including chronic kidney disease requiring dialysis, cirrhosis, hypertension, diabetes treated with insulin, and with a history of surgical aortic valve replacement 10 years before the onset of IE. She was admitted in critical condition to the Regional Specialist Hospital in Grudziądz, after the rapid development of heart failure, pulmonary edema, and severe aortic valve dysfunction on the 46th day of intensive antimicrobial treatment with a combination of vancomycin and ceftriaxone in the Department of Cardiology. A double-positive blood culture test confirmed IE, and vegetations were observed in transesophageal echocardiography (Figure 1 A). The patient was excluded from classical surgical aortic valve replacement because of the unacceptably high intraoperative mortality risk (EuroSCORE II = 96.57%). Due to the rapid deterioration of the clinical condition and the previously good condition during conservative treatment, the patient was deemed eligible for transcatheter aortic valve replacement. The procedure was performed via the femoral approach, and a Sapien 20 mm valve was implanted without complications. Postoperatively, a rapid improvement in the patient’s general condition and ejection fraction (from 15% preoperatively to 45% 1 day after the procedure) was observed, with no perivalvular leakage in postoperative transesophageal echocardiography (Figure 1 B). Blood culture tests performed 3 days after the procedure were negative. The symptoms of heart failure resolved postoperatively, and the patient was transferred to the Department of Cardiology for further treatment and discharged after 12 days. At 1-year follow-up, the patient was in an acceptable condition with no new symptoms and no perivalvular leakage. The patient’s written informed consent for publication of this case was obtained.
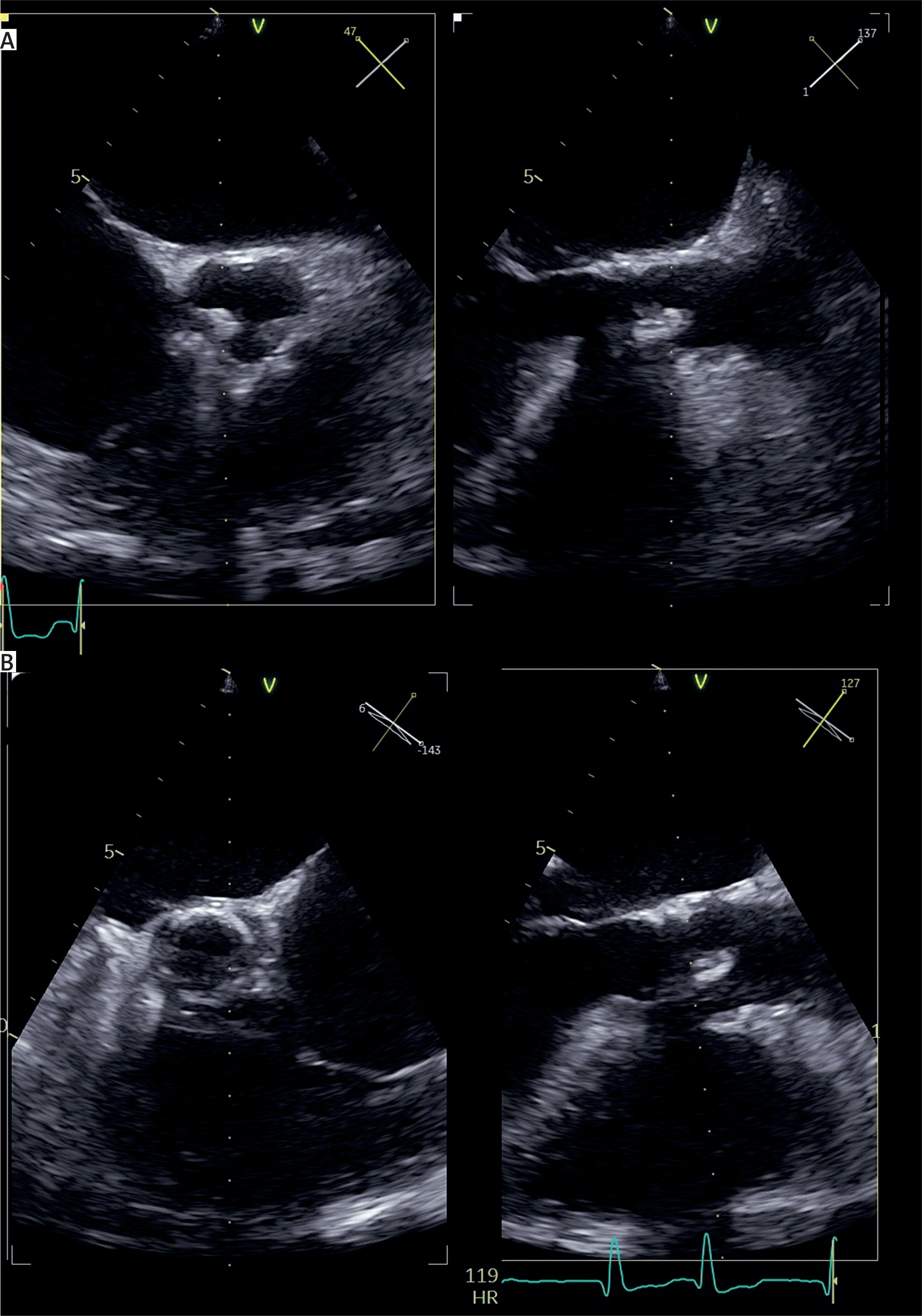
Figure 1
Transesophageal echocardiography. A – preoperative view of the biological prosthesis with visible vegetation. B – Postoperative view after valve-in-valve procedure with visible self-expandable valve
Heart failure is the main indication for urgent surgery in IE. In patients requiring emergency intervention, surgery should not be delayed, as it significantly increases early and 1-year survival in this population [3]. Treatment should be performed despite active endocarditis [4]. There is no evidence for the safety and efficacy of transcatheter aortic valve repair in patients with active endocarditis complicated by heart failure. The treatment of first choice should be surgical aortic valve replacement [1]. However, as in this case, in patients with an unacceptably high intraoperative risk, all treatment options should be considered, and urgent transcatheter aortic valve replacement can be successfully employed as a last resort.









