
Coronary artery anomalies are found in approximately 0.2% to 1.6% of patients who undergo coronary angiography, with the double right coronary artery (RCA) arising from two separate ostia in the right sinus of Valsalva being one of the rarest types [1–4]. We present a case of a patient with double RCA and acute inferolateral wall myocardial infarction due to occlusion in one of the two RCAs, which was successfully managed with primary percutaneous coronary intervention (PCI).
A 65-year-old male patient with a history of smoking and hyperlipidemia was admitted to the Cardiology Department due to chest pain. Electrocardiography revealed an elevated ST-segment in leads aVF and III and ST-T depression in leads I, aVL, and V2-V6. Echocardiography revealed akinesia of the inferior and inferolateral walls of the left ventricle, with a left ventricular ejection fraction (LVEF) reduction to approximately 45%.
The initial contrast injection revealed a critical stenosis in the middle segment of RCA 2 (Figure 1 A). RCA 1 originated from a separated ostium and, giving rise to the sinoatrial nodal artery, became visible after a slight adjustment of the diagnostic catheter position during the next contrast injection (Figure 1 B). Thrombotic occlusion of the distal RCA 1 with thrombolysis in myocardial infarction (TIMI) Flow Grade 0 was observed. The origin and course of the left coronary arteries were typical. An intermediate stenosis of the left anterior descending artery was found.
Figure 1
Baseline coronary angiography of the right coronary artery (RCA) in the left anterior oblique showing A – RCA 2 sub-occluded in the middle segment, giving one ventricular branch (acute marginal), B – total occlusion of the distal RCA 1. Post-percutaneous coronary intervention angiograms of C – RCA 1 dividing distally into posterior descending and posterolateral branches; D – atypical doubled RCA originating from separate ostia
PDA – posterior descending artery, PLA – posterolateral artery, RCA – right coronary artery, RVB – right ventricular branch.
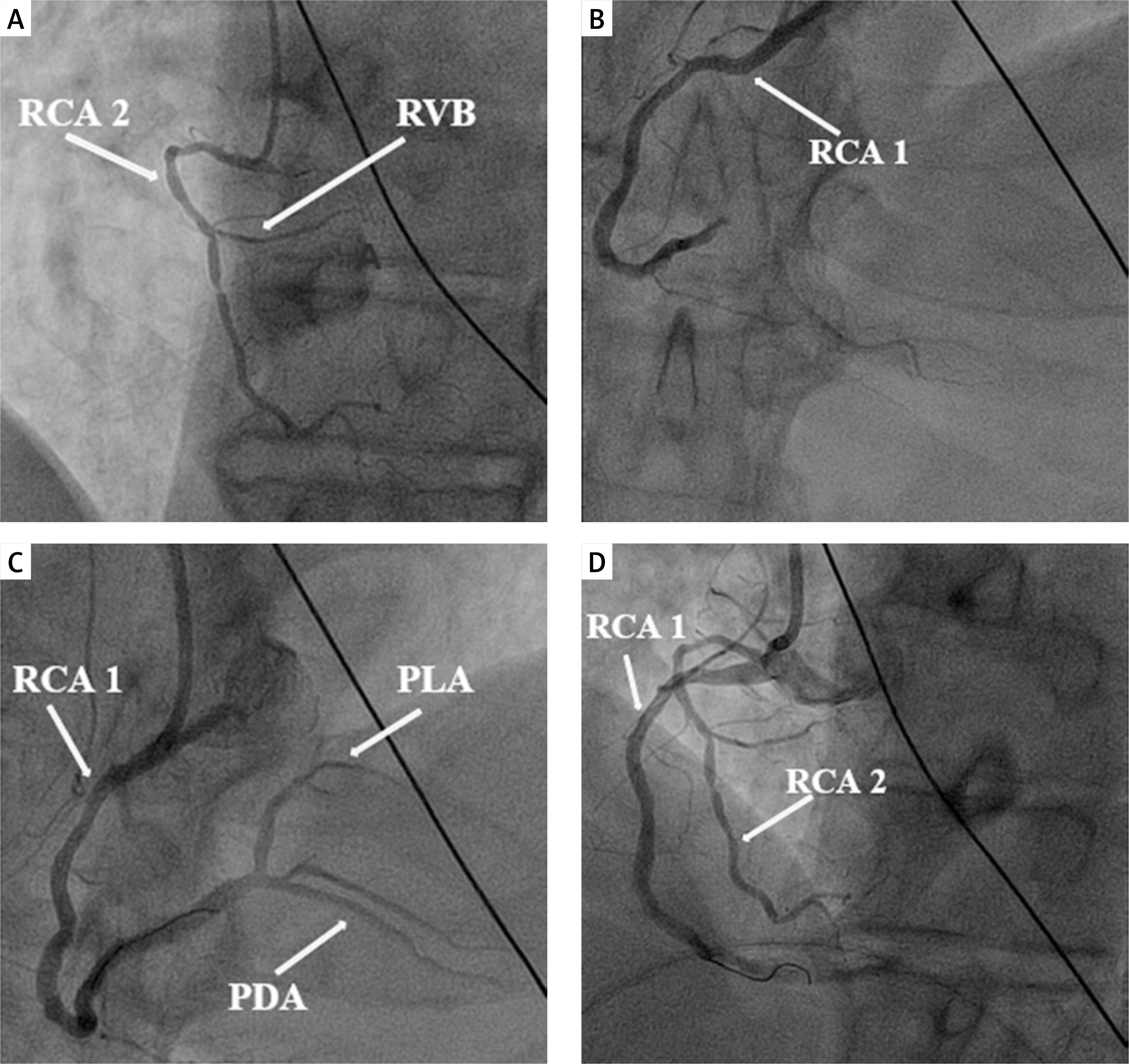
Primary PCI was performed on the RCA 1 culprit lesion. Therefore, the guiding catheter Launcher 7Fr JR 4.0 (Medtronic, USA, Minneapolis) was introduced, and the Versaturn-F workhorse guidewire (Abbott, USA, Santa Clara) was advanced through the RCA occlusion. Aspiration thrombectomy with RX Capturer (iVascular, Spain, Barcelona) was performed with restoration of TIMI 3 flow. Subsequently, after predilatation, the everolimus-eluting stent Synergy 3.0 × 38 mm 20 atm (Boston Scientific Corporation, USA, Marlborough) was successfully deployed to the lesion and postdilated with the non-compliant balloon Emerge 3.75 × 30 mm 18 atm (Boston Scientific Corporation, USA, Marlborough) with a good angiographic result (Figure 1 C). A follow-up coronary angiogram with a catheter withdrawn to the sinus of Valsalva demonstrated two separate RCAs originating from different ostia (Figure 1 D).
PCI successfully resolved the ST-segment elevations and provided symptomatic relief. The post-interventional course was uneventful, with a notable improvement in LVEF to 60% and no recurrence of symptoms. Dual antiplatelet therapy, consisting of aspirin (75 mg) and ticagrelor (90 mg twice daily), was initiated. The patient was scheduled for a staged procedure, including revascularization of RCA 2 and functional assessment of the LAD, and discharged without complications.
Double RCA is a very rare congenital anomaly of the coronary arteries. Most reported cases describe a double RCA originating from a single ostium. However, there are a few documented instances where a double RCA arises from two separate ostia in the right sinus of Valsalva [4]. The exact incidence of this anomaly is not well established. The main problem in diagnosis is that another ostium might be missed on selective coronary angiography. Coronary interventionists must be aware of this to prevent misinterpretation [5]. When the angiographic image is inconclusive and does not correspond to the results of non-invasive tests, the possibility of an anatomical anomaly, such as right coronary artery duplication, should be considered.







