





Sepsis is a leading cause of readmissions and is associated with increased medical costs. The hospital length of stay for readmissions following a sepsis hospitalisation is longer than readmissions following episodes of acute myocardial infarction, heart failure and chronic obstructive pulmonary diasease (COPD) [1].
A quarter of sepsis survivors are readmitted within 30 days, and 48% within 180 days. Furthermore, 25% of sepsis survivors require multiple readmissions within 180 days. The cumulative mortality rate of sepsis survivors attributed to readmissions is 8%, with an estimated cost of over $1.1 billion. Anaemia, cancer, chronic kidney disease (CKD), congestive heart failure (CHF), autoimmune diseases, pulmonary disease, diabetes and nursing home placement are associated with an increased risk of readmission [2, 3].
The most common cause of readmission after a sepsis hospitalisation is infection (69.2%), with 51% being labelled as recurrent/unresolved, especially among those who previously developed hospital-acquired infections or required longer duration of antibiotics and total parenteral nutrition [4].
Readmissions after a sepsis episode are more likely to result in death or transition to hospice care compared to readmissions after non-sepsis hospitalisations [5].
The aim of the study is to describe readmission patterns and mortality among survivors of a sepsis hospitalisation.
Our hypothesis is that among those who survived sepsis, infectious causes of readmissions are associated with increased mortality compared to non-infectious causes. Previous studies compared sepsis survivors to non-sepsis survivors but there is a paucity of data focusing only on sepsis survivors.
METHODS
After obtaining approval from the local Institutional Review Board (Rice Memorial Hospital, Willmar MN, USA) a retrospective cohort study of 147 sepsis survivors was carried out. Written informed consent was waived by the ethics committee since no individual data in any form are disclosed and this is a retrospective study.
These patients were originally admitted to the intensive care unit (ICU) with sepsis between 2012 and 2016 and survived the index hospitalisation. Survivors were followed up after dismissal. If multiple hospitalisations were present, only the first readmission was taken into consideration for study purposes. Readmissions were divided into two main categories: infectious vs. non-infectious.
The primary outcome was mortality rate during the study period. For the cause of death, death certificates were retrieved from the medical records and recorded. Secondary outcomes were: readmissions, and days to first hospitalisation.
Sepsis was defined as documented or suspected infection with two of the following: temperature of less than 36°C or more than 38°C; leukocyte count of less than 4 G L-1 or more than 12 G L-1; respiratory frequency of more than 20 breaths per minute or mechanical ventilation; heart rate of more than 90 beats per minute; or a qSOFA score ≥ 2. Septic shock was defined as the above plus plasma lactate of more than 2 mmoL L-1 (in the absence of hypovolemia) and need of vasopressor infusion to maintain a mean arterial pressure of 65 mm Hg after initial fluid resuscitation [6].
Exclusion criteria were: pregnant patients, patients younger than 18 years, patients without sepsis on index admission, patients not readmitted during the study period.
We collected the following data: demographics, clinical, radiological and laboratory variables at index hospitalisation, days to first readmission, number of readmissions, main cause of admission and readmission, cause of death.
Statistical analyses
Data are presented as mean ± standard deviation if normally distributed and median [25% and 75% ] or range if not. For parametric data, differences in the mean were compared by Student’s t-test. For highly skewed data, the Wilcoxon-Mann-Whitney test was used.
Differences in proportions were assessed by the χ2 or Fisher’s exact test.
Survival curves were generated using the Kaplan- Meier method. Cox proportional hazard models were used for variables with P values < 0.1 in univariate analyses.
P values lower ≤ 0.05 were considered statistically significant. All the analyses were performed using JMP statistical software version 14 (SAS Campus Drive, Cary, NC).
RESULTS
Index hospitalisation
One hundred and forty-seven patients survived the index hospitalisation. Baseline characteristics are described in Table 1.
TABLE 1
Baseline characteristics at index hospitalization among sepsis survivors (N = 147)
* Acute kidney injury defined as abrupt (within 48 h) reduction in kidney function with an absolute increase in serum creatinine of 0.3 mg dL-1 or more (≥ 26.4 μmoL L-1) or a percentage increase in serum creatinine of 50% or more (1.5-fold from baseline) or a reduction in urine output (documented oliguria of < 0.5 mL kg-1 h-1 for > 6 h) or need for renal replacement therapy
Among these patients, pneumonia was the cause of sepsis in 47 patients (31.9%), urinary tract infections in 37 patients (25.2%), cellulitis and peritonitis in 7 and 5 patients respectively (4.72% and 3.4%), cholecystitis in 5 patients (3.4%), Clostridium difficile colitis in 3 patients (2%), endocarditis in 4 patients (2.7%), cholangitis in 4 patients (2.7%).
Other causes of sepsis included catheter infections, bowel ischaemia, bowel perforation, diverticulitis, necrotizing fasciitis, neutropenic fever, osteomyelitis, pelvic inflammatory disease, perirectal abscess, septic arthritis, thrombophlebitis and toxic shock syndrome.
Eighteen patients (12.2%) had non specified sepsis; of these 44 percent had a positive blood culture, 50% had a positive urine culture and 60% had a positive sputum culture.
Readmissions
Over a median follow-up of 565 days (200–953) days, 88 patients (59.8%) were readmitted, 40 with an infectious process (45.4%) and 48 with a non-infectious condition (54.5%) (Table 2A).
TABLE 2A
Characteristics during index hospitalization among sepsis survivors who were later readmitted (N = 88)
Median time to first rehospitalisation for the entire cohort was 89 (19–337) days, although patients admitted with an infectious cause were readmitted sooner: 65.7 (11–201) days vs. 144 (52.3–383) days, P = 0.02.
Median number of readmissions was 2 during the study period [1, 3].
Non-infectious causes of readmission: COPD exacerbation (4 patients, 8.3%), surgical (27 patients, 56.2%), CHF exacerbation (4 patients, 8.3%), cerebrovascular accident (1 patient, 2%), gastrointestinal bleeding (3 patients, 6.2%), acute coronary syndrome/coronary artery disease (CAD) (2 patients, 4.17%), atrial fibrillation (1 patient, 2%), acute kidney injury (1 patient, 2%) and other/not specified (5 patients, 10.4%).
Surgical indications included hip fracture, small bowel obstruction, hernia repair, mitral valve repair, melanoma removal, ischaemic toe amputation, arteriovenous fistula repair, photo-vaporization of the prostate, hydronephrosis with ureteral stent placement and intracorporeal lithotripsy, colonic obstruction.
Infectious causes of readmission : non-specified bacteraemia (2 patients, 5%), enteritis (1 patient, 2.5%), pneumonia (17 patients, 42.5%), neutropenic fever (1 patient, 2.5%), cellulitis (3 patients, 7.5%), urinary tract infection (7 patients, 17.5 %), Clostridium difficile colitis (1 patient, 2.5%), peritonitis (1 patient, 2.5%), intra-abdominal abscess (2 patients, 5%) and non-specified sepsis (5 patients, 12.5%).
Factors associated with increased mortality in patients readmitted
Age, hypertension (HTN) (trend to statistical significance), pulmonary disease (trend) and infectious cause of readmission were associated with increased mortality. In multivariate analyses, age and infectious cause of readmission remained statistically associated with increased mortality (Tables 2B and 3).
TABLE 2B
Factors associated with mortality among sepsis survivors who were readmitted (n = 88)
TABLE 3
Cox proportional hazards model. Factors associated with increased mortality in sepsis survivors
| Factor | HR (95% CI) | P value |
|---|---|---|
| Age | 1.04 (1.01–1.08) | 0.002 |
| Hypertension | 1.40 (0.61–3.22) | 0.41 |
| Infectious cause of readmission | 2 (1.005–4) | 0.04 |
| Pulmonary disease | 1.69 (0.84–3.37) | 0.13 |
For the entire cohort, the most common cause of death was related to pulmonary complications (Table 4).
TABLE 4
Causes of death in sepsis survivors (n = 36)
[i] Cardiac causes: atrial fibrillation, acute congestive heart failure exacerbation, hypertension complications, myocardial infarction, right sided heart failure, massive pulmonary embolism. Pulmonary causes: acute respiratory failure, bronchiolitis organizing pneumonia, acute chronic obstructive pulmonary diasease exacerbation, sarcoidosis, hypoxia. Renal causes: acute kidney injury, hyponatremia, dehydration, end stage renal disease. Infectious: pneumonia, Enterococcus sepsis. Cerebrovascular events: acute ischemic stroke. Cancer: lymphoma, leukaemia. Surgical causes: strangulated hernia, abscess. Liver causes: cirrhosis.
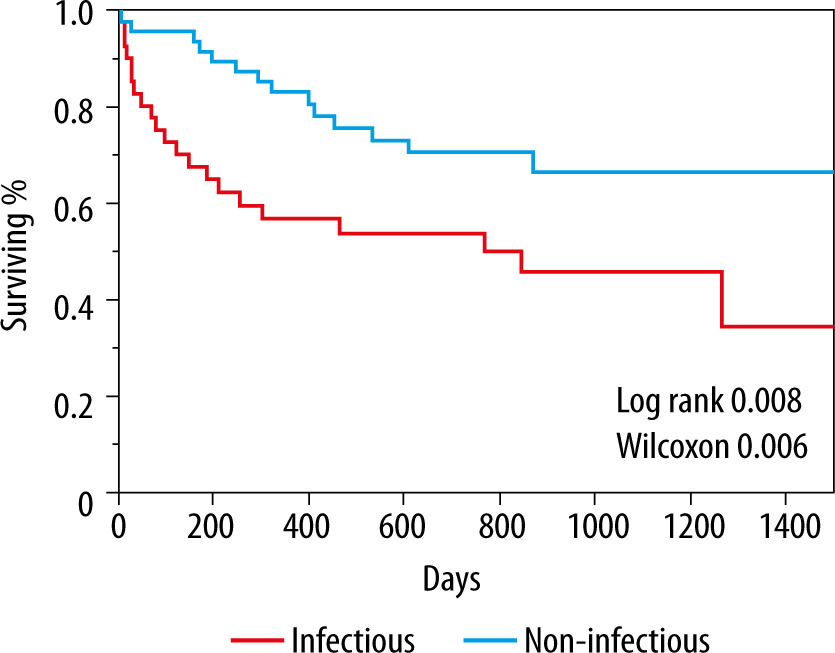
Survival rate was 45% (18/40) in those readmitted with an infectious process vs. 70.8% (34/48) in those readmitted due to a non-infectious cause, P = 0.01 (Figure 1).
DISCUSSION
The incidence of sepsis is increasing, and the short-term mortality is improving, generating more sepsis survivors. In order to further improve survival in this population, understanding the risk factors for adverse outcomes is essential.
Sepsis survivors have a high risk of readmissions and mortality following their hospitalisations, with a reduced life expectancy compared to the rest of the population and to those initially hospitalized with other medical conditions. Among Medicare patients only CHF has a higher 30-day readmission rate [7–9].
The mortality risk in sepsis survivors increases with a higher severity of the index septic episodes. Among 30-day survivors, sepsis reduces the remaining mean life span to 4 years. Sepsis also increases the risk of death for up to 5 years after the septic episode even after comorbidities are accounted for. In our study, although we did not find a statistical significance, there was a nominally higher SOFA score and vasopressor use during the index septic episode in those who were later readmitted with an infectious process. Furthermore, those who died were older and had more HTN and chronic pulmonary disease [10].
Non-infectious complications after sepsis admissions include a higher risk of cardiovascular events compared with matched-population control subjects, mainly due to their underlying medical conditions (CAD, CHF, diabetes, HTN) [11].
Among the non-infectious readmissions, we found a high number of surgical indications that could explain the lower mortality rate in this group, as studies in critically ill patients have shown higher mortality in the medical ICUs compared to surgical ICUs, which is attributed to a higher proportion of sepsis noted in medical patients [12, 13].
Infectious complications after sepsis hospitalisations are common, especially in those with diabetes, CKD, CHF, a higher number of comorbidities, longer index hospitalisation and nursing home placement [14].
In this study, infections caused earlier re-hospitalisations and increased risk of death in sepsis survivors and although more patients were readmitted with non-infectious aetiologies, when taken individually specific infections were still the leading cause of readmissions.
Most of the infectious readmissions were due to pneumonia or urinary tract infections, which mirrored the index hospitalisations. A prior study showed that two thirds of patients readmitted with sepsis within 90 days had infections at the same site of their initial admission. The burden of pneumonia (one of the leading causes of sepsis) cannot be underestimated, with a comparable 30-day all-cause risk-standardized mortality rate to acute myocardial infarction and heart failure [15, 16].
We hypothesize that residual/persistent infections could be related to inadequately treated index septic episodes. Another explanation is that recurrent infections could affect a frailer group of patients, with the overall poor prognosis due to a high burden of chronic medical conditions and older age. In our study, those patients who were readmitted with an infectious process were older and had more diabetes, which are known risk factors for infections [17, 18].
We found that most patients died from pulmonary complications, and this could be related to the high percentage of patients with chronic pulmonary disease and with pneumonia being the most common infectious process.
The strength of the study is the close follow-up of the cohort, since most patients received their medical care and subsequent follow-up in a local healthcare system. This allows for a more detailed description of the events following each hospitalisation.
The novelty of the study is the fact that we were able to compare different types of readmission among sepsis survivors, since most previous studies compared sepsis survivors to non-sepsis survivors. These results should be confirmed in larger studies.
LIMITATIONS
Limitations include being a retrospective single-centre study, a lower acuity case mix compared to bigger urban hospitals, a predominantly Caucasian population, a rural setting and a small number of patients. Regarding the attributed cause of death, several conditions can affect mortality at the same time in a synergistic fashion, so attributing death to only a specific condition might be overly simplistic.