
Cystic echinococcosis or hydatid cyst is a parasitic, zoonotic infectious disease caused by the larval stage of tapeworms of the species Echinococcus granulosus. Dogs are the definitive host of this tapeworm, while sheep, cattle, goats, and pigs are intermediate hosts. Humans are accidental host and infections in humans may cause harmful, slowly enlarging cysts in the liver, lungs, and other organs that may grow unnoticed and complicate later [1]. But Aspergillus superimposed on a hydatid cyst is quite a rare occurrence and recently few cases have been reported in the medical literature.
This is a case of an 18-year-old immunocompetent male patient who presented initially with three hydatid cystic lesions in hepatic, mediastinal and left sided pulmonary regions 3 months previously with a history of pet dog exposure. He had no prior history of fever, weight loss, or indications of immunodeficiency such as recurring infections. There was no history of a similar sickness in the family. Due to prominent abdominal complaints, laparoscopic hepatic cyst drainage with omentoplasty was performed. He was prescribed albendazole in a therapeutic dose due to absence of pulmonary symptoms. But, after 1 month he developed central chest pain and coughing with episodes of recurrent hemoptysis. Physical, hematological and biochemical examination revealed that the patient’s overall parameters were within the normal range with no signs of immunocompromised status. Three cystic lesions in the liver, lung, and mediastinum were found on the contrast-enhanced computed tomography scan (CT) scan, along with floating membranes in the lung lesion and perilesional edema in the liver. These lesions are likely hydatid cysts in various stages (Figures 1 A, B, E). On the left pulmonary side, there was a cystic lesion with floating membranes in the apical and lateral basal segments of the left lower lobe (Figures 1 B, C). There was also a mediastinal cyst of 4.59 × 4.02 cm size near the trachea and right main stem bronchus (Figure 1 D). Episodes of hemoptysis were increasing despite medical management, so urgent thoracic surgical intervention was planned. The patient underwent a midline sternotomy which revealed a mediastinal cyst and left lower lobe lung hydatid cyst adhering to the chest wall. Mediastinal cyst excision with left lower lobe hydatid cyst excision and cavity capitonnage were carried out with due care to avoid spillage. Gross examination showed multiple pearly white membranous structures, likely daughter cysts, from both cavities. The excised specimen was sent for histopathological examination, which revealed unusual features suggestive of hydatid cyst with aspergillosis in both. Microscopic examination of multiple sections revealed a cluster of acellular, lamellated hydatid membrane (Figure 2 A) with acute angle branching septate fungal hyphae suggestive of Aspergillus with focal areas of necrosis (Figure 2 B). The postoperative course was uneventful. Postoperatively the patient is totally symptom free and doing well on twice daily dosing of albendazole 400 mg and itraconazole tablets 100 mg for the last 1 month.
Figure 1
Computed tomography scan images. A – Coronal view showing mediastinal cyst (white arrow head), liver cyst (white cross), lung hydatid (white asterisk) with floating membranes. B – Coronal view showing mediastinal cyst (white arrow head) with hydatid cyst in left lung (white asterisk). C – Axial view showing left lung hydatid cyst with floating mass (white asterisk). D – Axial view showing mediastinal cyst of size 4.02 cm × 4.59 cm (white arrow head). E – Axial view showing hydatid cyst in liver (white cross)
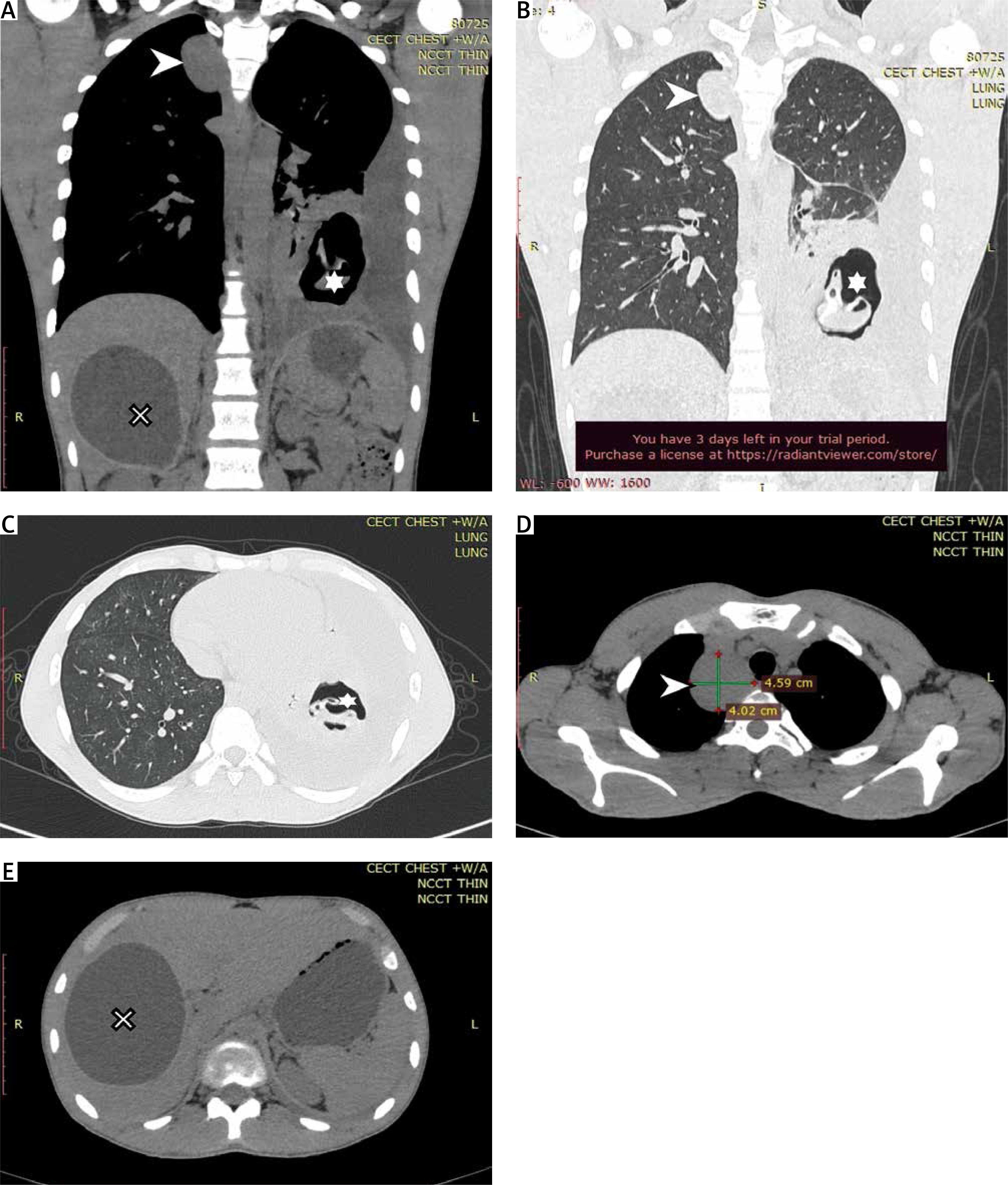
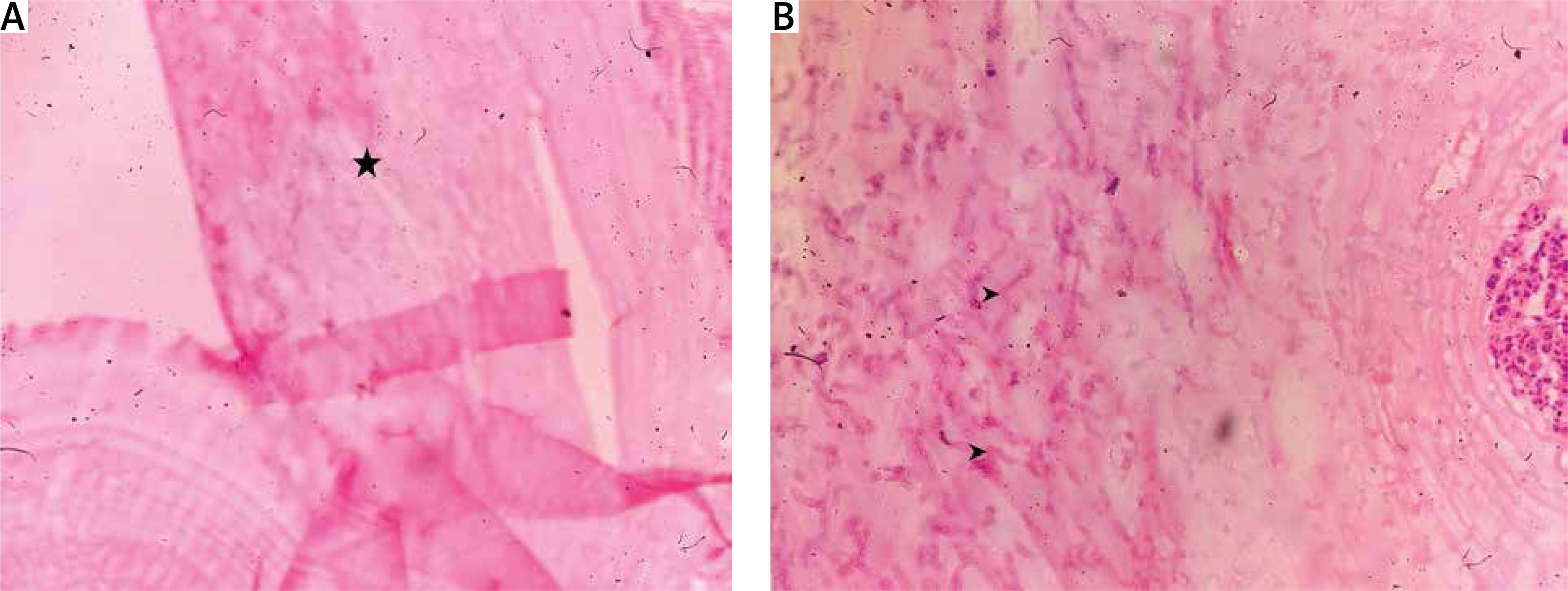
Figure 2
Histopathological examination images of cyst showing: A – acellular laminated membranes of hydatid (black asterisk) H + E stain 20×, B – infiltration of acute angled branched, septate fungal hyphae consistent with Aspergillum (black arrow heads) H + E 40×
Hydatid cyst causes serious lung and liver disease with a worldwide geographical distribution. In theory, this parasitic infection is preventable and treatable, but in impoverished regions of the world such as Asia, the Mediterranean region, South America, and Africa, this is still a serious yet neglected health hazard. Due to global immigration, patients can present in other geographical regions also. When it comes to hydatid illness, humans serve as the intermediate host, becoming infected after consuming tapeworm eggs. Animals including cats, dogs, and sheep are frequent sources [1]. The majority of Echinococcus granulosis larvae are filtered out of the lungs and liver, which function as sieves and are hence the most common sites of the illness. Chest X-ray, CT scan, and serological testing are used in the diagnosis and confirmation of pulmonary hydatid cyst. Cysts can vary in size and number, and symptoms will show up when they become large or rupture, which could cause fever, acute hypersensitivity reaction, coughing, chest pain, shortness of breath, and blood in sputum. Surgery is the established mainstay treatment for hydatid cyst disease with oral antihelminthics postoperatively [2].
Infection with the saprophytic fungus Aspergillus is typically observed in immunocompromised patients. Immune deficiencies, structural abnormalities, and pre-existing cavitary lesions, such as those caused by tuberculosis, sarcoidosis, bronchiectasis, abscess, and neoplasms, are the main predisposing factors for this infection. Aspergillosis (non-invasive aspergilloma), allergy bronchopulmonary aspergillosis, chronic pulmonary aspergillosis, and invasive pulmonary aspergillosis can all develop as a result of Aspergillus colonization in these situations. According to the location, a variety of microorganisms may superinfect hydatid and other cysts, with Aspergillus being rarely reported in hydatid cysts [3]. Aspergillosis and cystic echinococcosis share nearly the same symptoms and crescent signs on a chest CT scan. Hydatid disease and aspergilloma can also be detected discretely by radiological imaging, but due to the rarity of this condition, it is unclear if radiological approaches will be effective in diagnosing the co-infection. Based on their unique cytomorphologic properties, hydatid disease and aspergillosis can both be definitively diagnosed via cytology. In the same manner, serological tests can provide supportive evidence for both infections, with varying results, but done only when coexistence is suspected [4]. The coexistence of Aspergillus in hydatid cyst is an unusual finding that is prone to being overlooked because the clinical and radiological symptoms of both illnesses overlap and may obscure one another’s presence. Histopathological analysis is required for the confirmation of the diagnosis of hydatid disease with aspergillosis [5]. Gross, naked eye examination of cystic contents usually confirms the diagnosis of hydatid disease but there is definite importance of thorough microscopic examination of excised hydatid cysts and their contents. In the case of co-infection with Aspergillus fumigatus, there are high chances of incomplete treatment due to missing the complete diagnosis owing to its rarity. Identification of double pathology can help establishing the line of treatment that reduces post-operative complications and later dissemination [6, 7]. The true mechanisms involved in this co-infection will be revealed as the number of known cases is now accumulating, and this will finally help establish the best diagnostic and treatment options.
In conclusion, the patients previously reported mostly had other coexisting diseases or were immunocompromised. Surprisingly, in our case the histological study revealed this double presence of pathogens in two cavities at different sites in an immunocompetent patient, despite no predisposing factor. In the above case both intrathoracic hydatid cysts were co-infected with aspergillosis, causing rapid clinical deterioration, later with successful management due to the accurate diagnosis.









