
Anomalous right coronary artery from the pulmonary artery (ARCAPA) is an exceedingly rare congenital heart defect where the right coronary artery arises from the pulmonary artery. It occurs in approximately 0.002% of the general population [1], with its description mainly limited to case reports. Despite its rarity, this diagnosis is still clinically significant because it is associated with additional congenital heart anomalies in 25–30% of cases, and it can have serious clinical consequences, including myocardial infarction and sudden death, even in asymptomatic patients. The reported associated anomalies include aortopulmonary window (APW), atrial and ventricular septal defects (ASD and VSD), coarctation of the aorta (CoA), tetralogy of Fallot (TOF), bicuspid aortic valve (BAV), and patent ductus arteriosus (PDA) [2–4].
A 5-month-old infant (5.4 kg) with heart murmur was referred to our cardiac center for further evaluation. He was delivered at 39 weeks of gestation with a birth weight of 2.1 kg. Transthoracic echocardiography (TTE) was performed after birth and revealed a small patent foramen ovale (PFO) and PDA. The patient then was discharged home on digoxin and spironolactone.
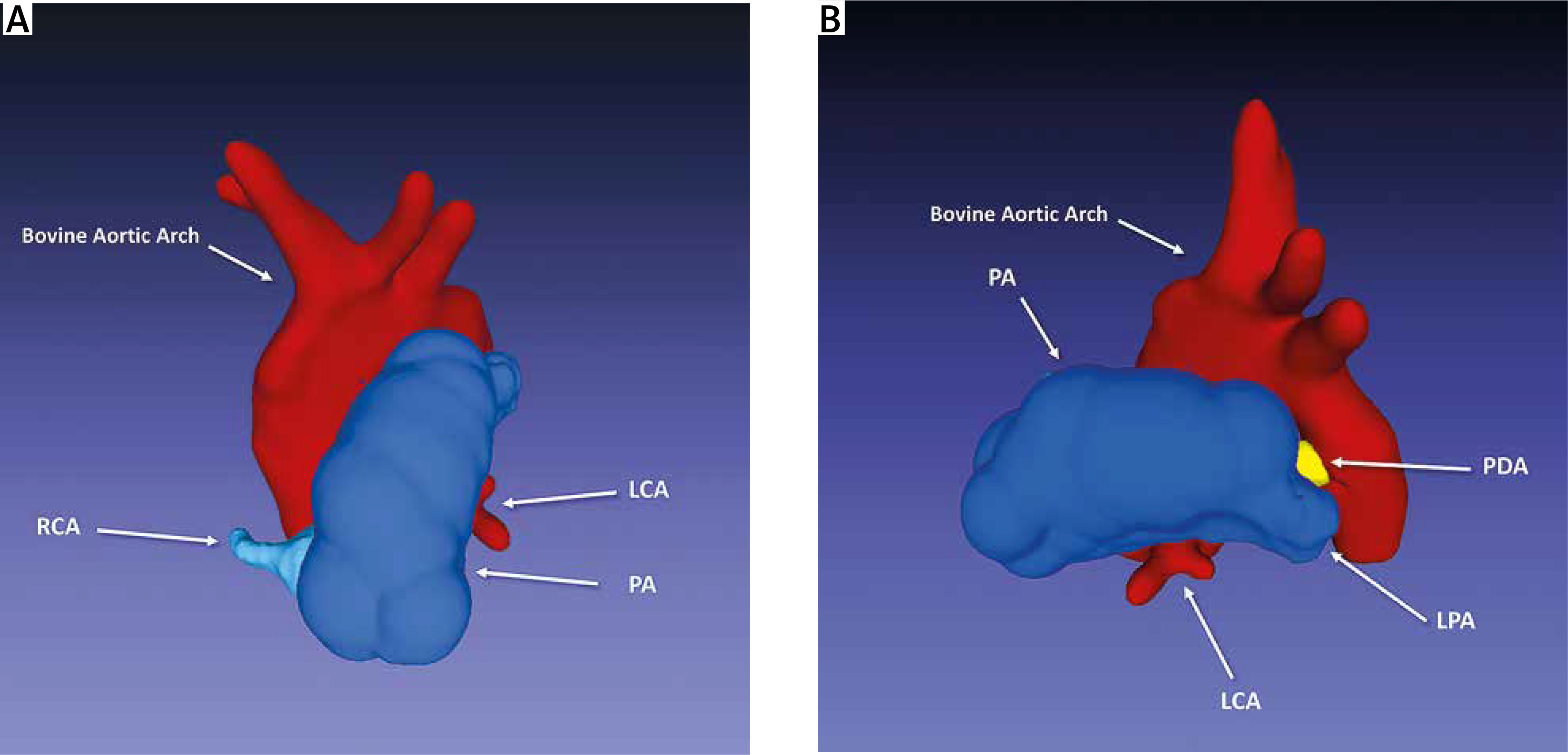
At the age of 5 months, he was admitted to our center for a PDA assessment. On physical examination, a continuous murmur was found. A chest X-ray revealed cardiomegaly. The electrocardiogram showed a normal sinus rhythm with signs of left ventricular hypertrophy. TTE established the diagnosis of PDA (4 mm) with left-to-right shunt, small PFO, and mild left ventricular dilation with preserved systolic function. The patient had cardiac catheterization for PDA assessment, which revealed an unexpected finding: an apparent ARCAPA originating from the pulmonary artery and a PDA measuring 4 × 4 mm (Figures 1 A, B). Moreover, computed tomography confirmed and showed the right coronary artery (RCA) arising from the right anterior sinus of pulmonary artery, bovine aortic arch, and a PDA of 3.5 mm in diameter and 2 mm in length (Figures 2 A, B).
Figure 1
A – Lateral view of angiogram demonstrates filling of the left coronary artery and no filling of the right coronary artery (RCA). The patent ductus arteriosus (PDA) can also be seen. B – Posterior-anterior angiogram showing RCA arising from the right anterior aspect of the main pulmonary artery with the usual course through the right atrioventricular groove (arrowheads)
LCA – left main coronary artery, PA – pulmonary artery, LAD – left anterior descending artery, LCx – left circumflex artery.
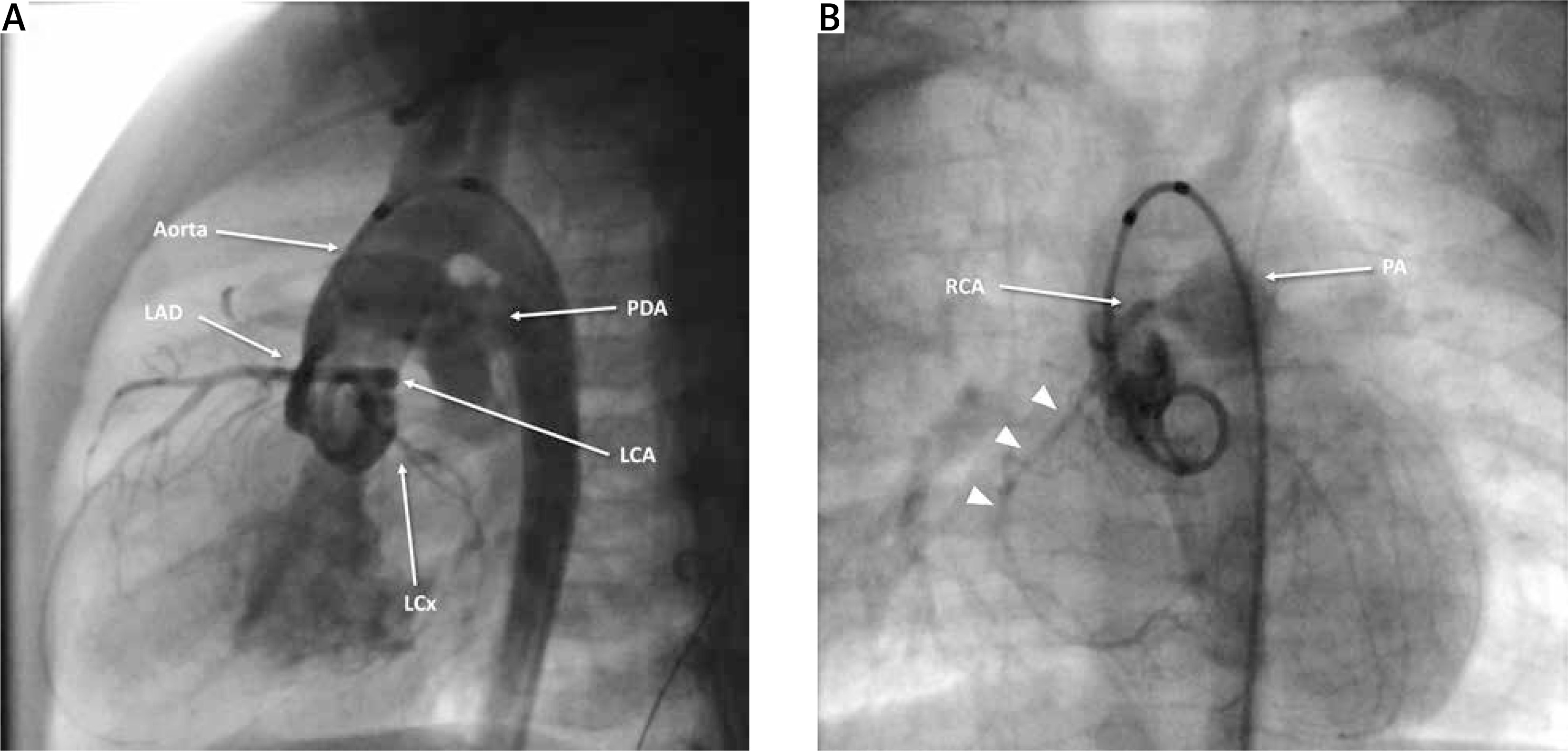
Figure 2
3D reconstruction model. A – Anterior view showing the anomalous origin of the right coronary artery from the pulmonary artery (ARCAPA), and the bovine aortic arch can also be seen. B – Lateral view showing the patent ductus arteriosus (PDA) (yellow) and normal origin of left main coronary artery (LCA)
LPA – left pulmonary artery, PA – pulmonary artery, RCA – right coronary artery.
The patient was discussed within a multidisciplinary heart team, and was subsequently referred for surgery. After median sternotomy, subtotal thymectomy was performed, and the ARCAPA was identified. The PDA was clipped, and cardiopulmonary bypass (CPB) was instituted using aortobicaval cannulation. Del Nido cardioplegic solution was administered into the aorta and directly via the coronary ostium of the RCA. After pulmonary artery transection, the RCA was harvested and then directly reimplanted into the aorta using a trap-door technique. The main pulmonary artery was reconstructed with autologous pericardium. The patient was weaned off CPB on inotropic support without incident.
The postoperative course was uneventful, and the patient was discharged 15 days later. At 4 years of follow-up, the patient is doing well with good ventricular function, no residual shunt, and normal coronary flow.
ARCAPA is a rare congenital cardiac anomaly that occurs in most cases in isolation. It can, however, be associated with other congenital heart defects, most commonly an APW (10.8%), followed by VSD (6.3%) and ASD (4.9%) [3]. Additional associations include TOF, BAV, PDA, and CoA. ARCAPA associated with patent ductus arteriosus is a rare entity, with just 7 (3.1%) cases of 223 reported in a literature review since 1950 by Guenther et al. [3]. ARCAPA is frequently diagnosed incidentally [1, 3]. The clinical presentation of patients with ARCAPA was found to be quite variable, and the patients may be completely asymptomatic or may present with murmur, angina, dyspnea, heart failure, or sudden cardiac death [3, 5].
Unlike patients with an anomalous left coronary artery from the pulmonary artery (ALCAPA), patients with ARCAPA typically present later in life if no associated congenital heart defect is present. This is because the right ventricle has a lower oxygen demand than the left ventricle, and ventricular ischemia is less common in ARCAPA than in ALCAPA [4].
The presence of a significant left-to-right shunt, such as an APW, PDA, or VSD, in association with an anomalous coronary artery maintains high pulmonary artery pressure and antegrade delivery of oxygenated blood, allowing coronary artery flow through the anomalous coronary artery from the pulmonary artery to be maintained and myocardial ischemia to be less likely to develop, which may mask the diagnosis. Furthermore, these patients’ clinical presentations predominantly display symptoms of a left-to-right shunt via the APW, PDA, or VSD [4].
Various surgical techniques have been described for treating ARCAPA, including simple ligation, different types of bypass grafting, subclavian artery graft, intrapulmonary baffle (Takeuchi technique), and the most commonly employed method, direct coronary reimplantation into the aorta [1, 6]. At our center, we prefer to establish a dual coronary artery supply through direct coronary reimplantation with a trap-door technique.
In conclusion, the association of ARCAPA and PDA is a rare congenital cardiac anomaly. This case highlights the importance of considering congenital coronary anomalies in children presenting with significant left-to-right shunts. Surgical correction involving direct reimplantation of the anomalous coronary artery offers excellent outcomes. Regular follow-up is necessary to monitor for any late complications.









