
Summary
Recent data suggest the limited role of diabetes mellitus as a key factor for the optimal decision-making of revascularization strategies. It has been shown that diabetes has no significant interaction effect with coronary artery bypass grafting (CABG) and percutaneous coronary intervention (PCI) in establishing long-term clinical outcomes in the SYNTAX, EXCEL and BEST trials. Due to the lack of an interaction effect between surgery and PCI in the SYNTAX trial, presence of diabetes was excluded from the SYNTAX score II. In the present study, we aimed to compare all-cause 4-year mortality from a real world multi-center population after revascularization for complex coronary artery disease (CAD) in diabetics. The results of the present study can be summarized as follows: 1) PCI could be a reasonable option in diabetics with a low SYNTAX (0–22) score. 2) The general perception of diabetes and left main CAD as a crucial decision-maker favoring CABG over PCI for complex CAD should be replaced with individualized risk assessment which includes the SYNTAX score and SYNTAX score II.
Introduction
Over the past few decades, diabetes mellitus (DM) has been commonly perceived as a crucial decision-maker favoring coronary artery bypass grafting (CABG) surgery over percutaneous coronary intervention (PCI) for complex, i.e. three-vessel, or significant left main coronary artery disease (CAD). This is based on the results of a historical BARI trial showing a survival benefit in diabetics after CABG compared with PCI (5-year survival: 81% for CABG vs. 66% for PCI; p = 0.003) [1]. It was further supported by reports of the FREEDOM trial, which has a 7.5 years follow-up revealing that CABG is associated with lower all-cause mortality rather than with PCI in diabetic patients with multi-vessel CAD (n = 1900; 83% three-vessel CAD; 18.3% in the CABG group vs. 24.3% in the PCI group; p = 0.01) [2]. However, recent randomized trials comparing CABG and PCI with newer generation drug-eluting stents (DES) and advanced medical therapy (opposite to plain-old balloon angioplasty in the BARI trial and first-generation DES in the FREEDOM trial) have shown fewer advantages of CABG over PCI, especially for left main CAD, making the decision-making process more challenging than ever before [3, 4].
Patients in need of myocardial revascularization should be carefully evaluated [5]. This includes assessment of key factors for predicting future events such as age, kidney function, left ventricular ejection fraction and anatomical complexity of CAD assessed by anatomical SYNTAX score. In the SYNTAX, FREEDOM and BEST trials [6], diabetes mellitus (DM) was an independent predictor of major adverse cardiovascular events (MACE) after either CABG or PCI. However, the most important aspect of specific characteristics for clinical decision-making is the interaction effect because it drives decision-making between CABG and PCI [7]. If a significant interaction is present, the clinical factor aids in choosing the approach, either CABG or PCI, which is most likely to provide the best outcome. The findings of SYNTAX, EXCEL and BEST trials showed no interaction of DM with CABG and PCI and suggest the limited role of DM as a key factor for the optimal decision-making of revascularization strategies [6]. Due to the lack of an interaction effect between CABG and PCI in the SYNTAX trial, DM was not included in the SYNTAX score II [8].
In patients with DM, the current guidelines [5] recommend CABG over PCI in patients with a SYNTAX score ≥ 23.
Aim
In the present study, we aimed to compare the all-cause 4-year mortality from a real world multi-center population after revascularization for complex CAD in diabetics.
Material and methods
Study population
Patients from the Wilhelminenspital, Vienna, Austria and the University Clinical Centre of the Republic of Srpska, Banja Luka, Bosnia and Herzegovina who were treated with PCI with second generation DES or referred to other institutions for CABG between January 1, 2008, and December 31, 2010 were identified through the review of the hospital electronic medical records. Consequently, elective patients with significant left main and/or three-vessel CAD (≥ 50% diameter stenosis) without major hemodynamic instability were included in the study (Figure 1). The research protocol was approved by the respective local ethics committees. The PROUST study is a multi-center project and was a part of a PhD thesis [9, 10].
Figure 1
Study flow chart
WS – Wilhelminenspital, UCC RS – University Clinical Centre of the Republic of Srpska, VD – vessel disease, STEMI – ST-segment myocardial infarction, CABG – coronary artery bypass grafting, PCI – percutaneous coronary intervention, ULMCA – unprotected left main coronary artery.
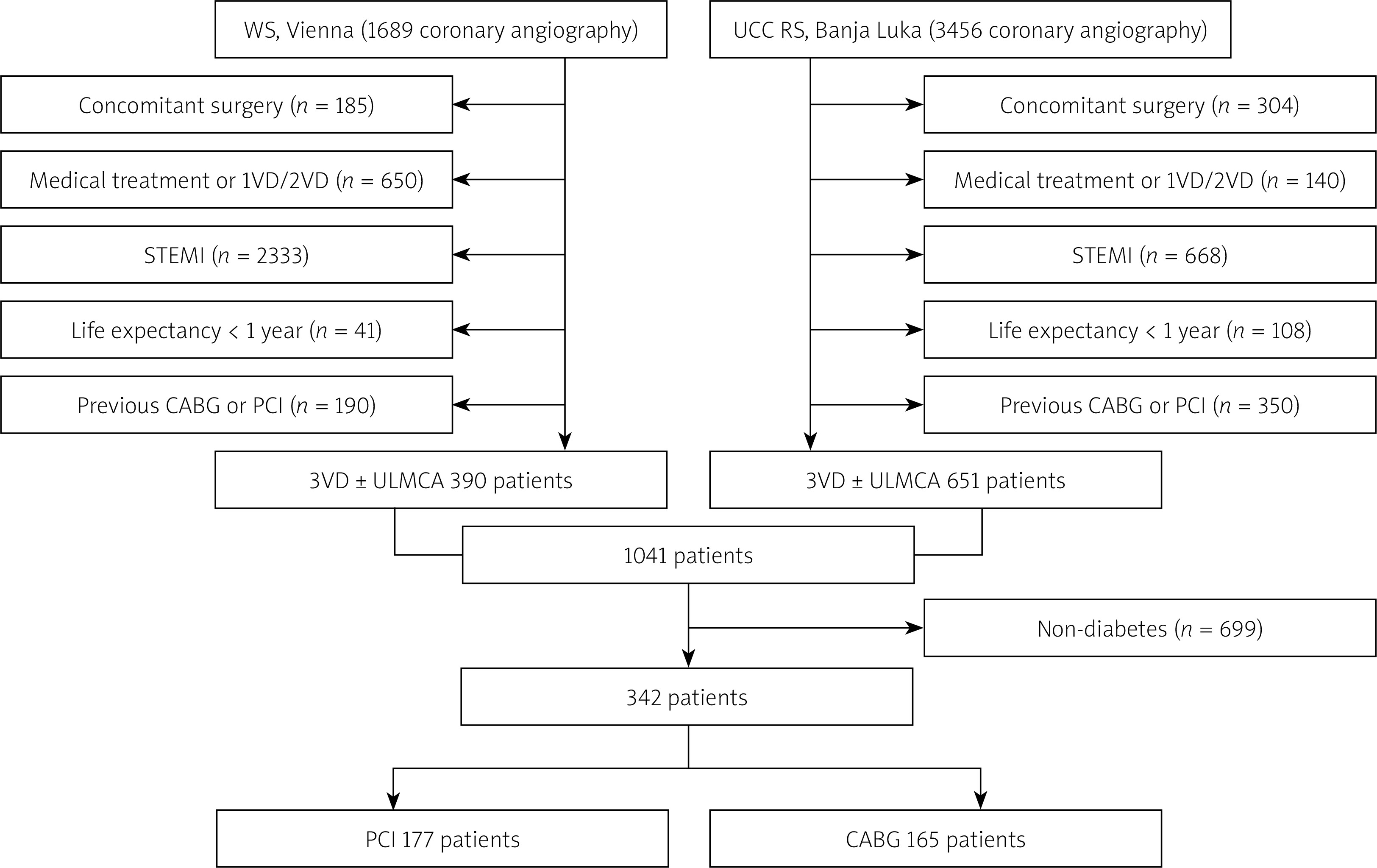
Patients were not included in the study if they presented with ST segment elevation myocardial infarction, underwent previous PCI or CABG, had terminal illnesses with projected life expectancy less than 1 year, were in need of concomitant cardiac surgery, or if they had one-vessel or two-vessel disease. Moreover, patients without indications for myocardial revascularization were excluded from the study. All-cause mortality was ascertained from mortality registries from Austria and Bosnia and Herzegovina and/or by telephone contacts. Twenty-six patients were lost to follow-up, representing 2.5% of the total patient cohort.
Baseline characteristics
For the purpose of the study, the following variables were collected and entered into a dedicated database: two anatomical variables (the SYNTAX score and presence of left main CAD), age, estimated glomerular filtration rate, left ventricular systolic function, gender, presence of chronic obstructive pulmonary disease, peripheral vascular disease, presence of type 2 DM, history of dyslipidemia, history of arterial hypertension, smoking history, familiar history of CAD as well as history of heart failure, myocardial infarction and stroke.
The SYNTAX score was estimated by summation of each separate lesion (defined as 50% diameter stenosis in vessel larger than 1.5 mm) from an online calculator (www.syntaxscore.com). Glomerular filtration rate was calculated using the Cockcroft-Gault formula [11]. Left ventricular systolic function was assessed by transthoracic echocardiography. Chronic obstructive pulmonary disease was defined as the long-term use of bronchodilators or steroids for lung disease (EuroSCORE definition [12]). Peripheral vascular disease was defined as one or more of the following: claudication, carotid occlusion or > 50% diameter stenosis, amputation for arterial disease and/or previous or planned intervention on the abdominal aorta, limb arteries or carotids (Arterial Revascularisation Therapies Study Part I definition [13]).
Statistical analysis
Data were available in at least 95% of the included patients. Categorical variables were presented as numbers and percentages and compared using the c2 test. Continuous variables were expressed as mean with standard deviation (SD) or median with interquartile range (IQR) and compared using Student’s t test or the Mann-Whitney U test according to the data distribution and number of groups. The Kolmogorov-Smirnov test and visual assessment were used to assess the normality of distribution of all continuous variables. Kaplan-Meier analysis was used to assess outcomes after CABG or PCI, and Cox-based adjustment was performed involving the following covariates: age, gender, SYNTAX scores as well as presence of left main CAD and insulin treatment. Independent predictors of all-cause mortality were identified by univariate and multivariate regression analysis. For the purpose of subgroup analysis, Cox regression analysis was used. Interaction effect of diabetes was defined as the hazard ratio of mortality associated with presence of type 2 DM among patients undergoing PCI, divided by the hazard ratio for the same characteristic, i.e. presence of diabetes among patients undergoing CABG. All statistical analyses were performed using IBM SPSS Statistics, version 25.0 (New York, USA).
Results
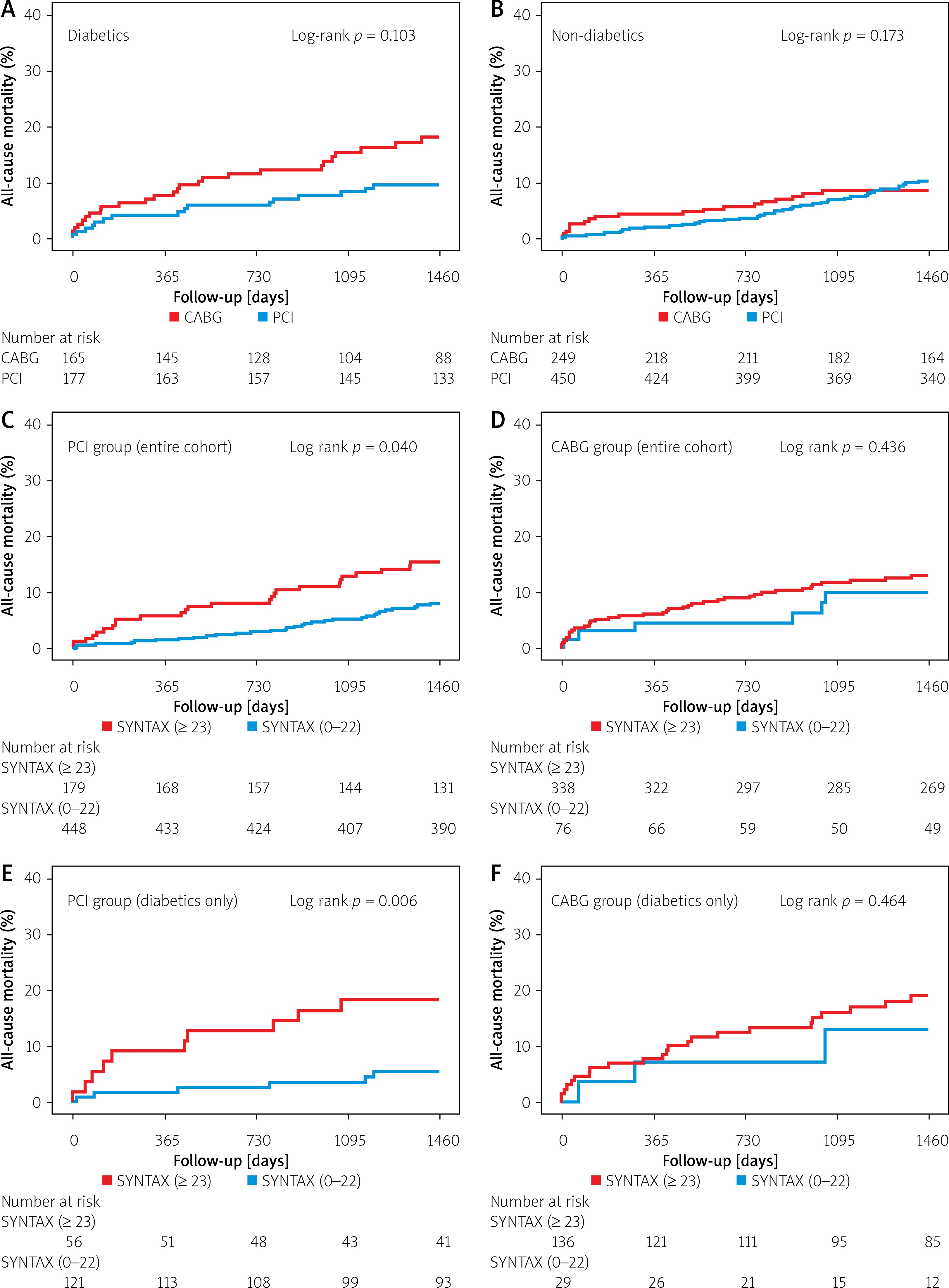
A total of 1041 patients were included in this study (Figure 1). There were 342 diabetic patients, of whom 177 patients underwent PCI and 165 patients were referred for CABG. The cumulative incidence rates of all-cause death were different between diabetics treated with PCI or CABG at 4 years (16/177, 9.0% vs. 26/165, 15.8%, respectively, log-rank p = 0.03, Figure 2 A). This difference was not evident in non-diabetics (PCI: 41/450, 9.1% vs. CABG: 19/249, 7.6%, log-rank p = 0.173, Figure 2 B). Diabetics in whom CABG was performed were significantly older (64.69 ±8.8 vs. 62.6 ±9.4, p = 0.03), more often on insulin treatment (88/165, 53.3% vs. 25/177, 15.3%, p = 0.01), had more complex anatomical characteristics, i.e. higher SYNTAX scores (32.5 IQR (15) vs. 18.0 IQR (15), p < 0.01) and with left main stenosis (70/165, 42.4% vs. 7/177, 4.0%, p < 0.01), compared to diabetics treated with PCI (Table I). However, after adjustment of factors that differed between the groups, a difference in all-cause mortality was not observed (adjusted p = 0.10).
Table I
Baseline characteristics of diabetics treated with CABG or PCI. Categorical variables are presented as numbers and percentages and are compared using the χ2 test. Continuous variables are expressed as mean ± standard deviation (SD) or median with interquartile range (IQR) and are compared using Student’s t-test or the Mann-Whitney U test
Figure 2
Kaplan-Meier analysis. The cumulative incidence rates of all-cause death between diabetics (A) and non-diabetics (B) treated with PCI or CABG at 4 years. Patients treated with PCI showed lower all-cause mortality in the low SYNTAX group compared with the intermediate-high SYNTAX group (C). SYNTAX score was not associated with higher all-cause death in the CABG group (D). In diabetics, there was a higher incidence of all-cause mortality in PCI patients with intermediate-high (≥ 23) SYNTAX scores compared with those with low (0–22) SYNTAX scores (E). Diabetics who underwent CABG showed similar mortality rates irrespective of the SYNTAX scores (F)
Patients with or without DM treated with PCI (n = 627) showed similar mortality rates at 4 years (16/177, 9.0% vs. 41/450, 9.1%, log-rank p = 0.927), whereas diabetics who underwent CABG died more frequently than non-diabetics who underwent CABG (26/165, 15.8% vs. 19/249, 7.6%, log-rank p = 0.008).
Out of 177 diabetics who were treated with PCI, 108 (61.0%) are from Bosnia and Herzegovina. No mortality difference was found between low- and high-income countries (Bosnia: 9/108, 8.3% vs. Austria: 7/69, 10.1%, log-rank p = 0.919). Similarly, diabetics who underwent CABG from Bosnia and Herzegovina died no more often than their comparators from Austria (15/103, 14.6% vs. 11/62, 17.7%, log-rank p = 0.832, respectively).
When SYNTAX score II recommendation was taken into account (Table I), inappropriate PCI (performed in patients with CABG only recommendation) was associated with significantly higher mortality at 4 years (9/60, 15.0% vs. appropriate PCI: 7/117, 6.0%, log-rank p = 0.046, number-needed-to-treat = 11).
In the entire cohort, patients treated with PCI showed lower all-cause mortality in the low SYNTAX group compared with intermediate-high SYNTAX group (31/448, 6.9% vs. 26/179, 14.5%, log-rank p = 0.040, Figure 2 C). On the other hand, SYNTAX was not associated with higher all-cause death in the CABG group (low SYNTAX (0–22): 6/76, 7.9% vs. intermediate-high SYNTAX (≥ 23): 39/338, 11.5%, log-rank p = 0.436, Figure 2 D). In diabetics, there was a higher incidence of all-cause mortality in PCI patients with intermediate-high (≥ 23) SYNTAX scores compared with those with low (0–22) SYNTAX scores (10/56, 17.9% vs. 6/121, 5.0%, respectively, log-rank p = 0.006, Figure 2 E). In contrast, diabetics who underwent CABG showed similar mortality rates irrespective of the SYNTAX scores (SYNTAX 0–22: 3/29, 10.3%; SYNTAX ≥ 23: 23/136, 11.9%, log-rank p = 0.464, Figure 2 F). In non-diabetics, mortality following PCI with low (0–22) SYNTAX scores did not reach significance (although numerically higher) from mortality following PCI with intermediate-high (≥ 23) SYNTAX scores (25/327, 7.6% vs. 16/123, 13.0%, respectively, log-rank p = 0.097). In CABG patients without DM, mortality was not associated with SYNTAX scores (SYNTAX 0–22: 3/47, 6.4%; SYNTAX ≥ 23: 16/202, 7.9%, log-rank p = 0.793).
In the multivariate Cox regression analysis, left ventricular ejection fraction was identified as an independent predictor of all-cause mortality in the entire cohort, while age was independently associated with death in the PCI group. Multiple predictors were found in the CABG group (Table II). In the subgroup analysis (Table III), there was no interaction according to presence or absence of left main CAD (pinteraction = 0.120) as well as according to diabetes status (pinteraction = 0.377). Otherwise, female vs. male and ≥ 23 vs. 0–22 SYNTAX scores were differentiators between PCI and CABG with a pinteraction < 0.01.
Table II
Univariate and multivariable Cox regression analysis of overall survival in the entire cohort, PCI and CABG group
Table III
Hazard ratios for all-cause mortality in the PCI group, compared with the CABG group, in the selected subgroup of patients
Discussion
The results of the present study can be summarized as follows: 1. Cautious selection of revascularization method (PCI over CABG) in a selected patient population (outside of clinical trials) can lead to lower mortality over a period of 4 years; 2. In patients with complex CAD, including those with DM, the SYNTAX score is a helpful tool in guiding decision-making; 3. DM by itself appears not to be a good differentiator in guiding decision-making between PCI and CABG.
High mortality rates in patients with DM were observed in angiographic studies, which demonstrated that diabetes was associated with a greater atherosclerotic burden and an increased number of lipid-rich plaques, which were prone to rupture [14]. Recently, the 10-year follow-up of the SYNTAX trial became available [15], revealing that 34.2% of diabetics following PCI and 32.1% of diabetics following CABG did not survive (p = 0.56). Similarly, in the recent meta-analysis from 11 randomized trials comparing CABG versus PCI, high mortality was found in diabetics with multi-vessel CAD over a mean follow-up of 3.8 years (15.5% after PCI vs. 10.0% after CABG; p = 0.0004) [16]. Interestingly, in our study all-cause mortality after CABG was higher when compared with PCI (15.8% vs. 9.0%, p = 0.03, respectively), which can be explained by older age and more comorbidities. If the effect on mortality by the treatment selection by an experienced cardiologist in discussion with the patient was canceled by adjustment (Cox) then any mortality difference disappeared (p = 0.103). The incidence of all-cause mortality in diabetics following PCI (9%) was lower than in the meta-analysis [16], similar to the 7-year mortality rates in the BARI trial [17] where randomized patients assigned to PCI had higher mortality rates than registry patients selected for PCI (19.1% vs. 13.9%, p = 0.01) – this difference was not significant after adjustment (p = 0.16). In an analysis of over 16,000 patients with diabetes and complex CAD, PCI with second generation DES was associated with lower death when compared with CABG [18]. Furthermore, in a meta-analysis of BEST, EXCEL and NOBLE trials comparing PCI with CABG using newer DES, MACE was lower with PCI when compared with CABG at 30 days [19]. Over long-term follow-up, there was no difference in outcomes between the two groups [19]. This is in concordance with our results where cautious selection of revascularization method (PCI over CABG) in a selected patient population (outside of clinical trials) can lead to lower mortality over a period of 4 years.
In the CABG stratum of BARI-2D (n = 763), there was no difference in mortality between CABG and medical therapy (p = 0.33) at 5-year follow-up [20]. On the other hand, CABG was superior to PCI in FREEDOM for mortality at 7.5-year follow-up [2]. The discordant results are either due to enrollment of patients with more extensive CAD in FREEDOM who potentially benefitted from CABG (mean SYNTAX: 26.2 ±8.4) or due to more stent-related adverse events in the PCI group with the use of first generation DES. Recent data consistently show reduction in mortality (driven by decreases in stent thrombosis) with newer DES when compared with early generation DES or bare metal stents [21–23]. In a meta-analysis, the mortality gap narrowed to statistical non-significance when the comparator was newer generation DES [24].
In patients with DM, compared with those without DM, the anatomic complexity of CAD tends to be more expressed, which can be explained by the progressive form of atherosclerosis associated with increased mortality [15]. More complex CAD, i.e. higher SYNTAX scores (which also contain the sum of points assigned to the empirically estimated difficulties just to perform PCI, but not CABG), is related to more complex PCI and, consequently, more adverse events. Therefore, CABG is considered to be the preferred revascularization method for diabetic patients with complex CAD, i.e. SYNTAX ≥ 23. This is based on the results of the 5-year follow-up (and confirmed at 10-year follow-up) of the SYNTAX trial which showed no differences in the composite safety endpoint of all-cause death, stroke, and myocardial infarction, but the need for repeat revascularization (p < 0.001) was more frequent in patients treated with PCI than in those who underwent CABG [15]. Our analysis, which was initiated by the investigator and comes from the everyday routine practice, shows that careful patient selection led to lower mortality following PCI, even if diabetes is a comorbidity. We showed that, similarly to the SYNTAX trial [15], PCI in patients (and the subgroup of diabetics) with intermediate-high (≥ 23) SYNTAX scores is related to higher mortality than PCI in those with low (0–22) SYNTAX scores. However, mortality following PCI in intermediate-high (≥ 23) SYNTAX scores was not different from mortality following CABG (PCI: 26/179, 14.5% vs. CABG: 39/338, 11.5%, p = 0.388 and PCI + diabetes: 10/56, 17.9% vs. CABG + diabetes: 23/136, 11.9%, p = 0.193).
The selection of PCI or CABG should depend on the risk–benefit ratio of each revascularization strategy, balancing periprocedural adverse events as well as long-term benefit for mortality or serious clinical outcomes. Although DM was found to be an independent predictor of all-cause mortality following CABG (Table II), it was not a good differentiator between PCI and CABG as expressed by the interaction effect (Table III). Our results corroborate the 10-year follow-up of the SYNTAX trial (pinteraction = 0.66) [15], the BEST trial (pinteraction = 0.77) [25], as well as a meta-analysis of BEST, EXCEL and NOBLE trials where no interaction between diabetes status and type of myocardial revascularization was found [19]. We found that female gender is a predictor of poor outcome following CABG (pinteraction = 0.07), which is in concordance with previous trials [26] and in discordance with the SYNTAX score II where CABG was considered as a better option in females [7]. Interestingly enough, female gender was not a differentiator in the FREEDOM trial [2]. Despite the difference in impact of gender, non-compliance with SYNTAX score II was associated with a poor outcome following PCI, which is in concordance with recently published data [9, 27, 28].
Recently, presence of DM was identified as an independent predictor for the primary endpoint in patients with left main CAD following both CABG and PCI [3]. In EXCEL, no interaction between diabetes status and revascularization type for primary endpoint (pinteraction = 0.82) and any secondary endpoints could be observed [3]. This is supported by the recent pooled analysis [16] in which patients with left main CAD and DM showed no difference in 5-year all-cause mortality (10.5% vs. 10.7% after PCI and CABG respectively; p = 0.52). We found no interaction according to presence or absence of left main CAD (pinteraction = 0.12).
The present study has several limitations as well as advantages: (1) the relatively low number of patients – however, our patients are from multi-center everyday routine practice; (2) data collection, especially in surgical centers, was suboptimal, e.g. we were not able to sample data for surgical complications – however, long-term mortality data are available for almost all patients; (3) the period of enrollment was between 2008 and 2010 with 4-year follow-up – the longer follow-up was intended, but almost impossible due to migrations in Bosnia and Herzegovina; however, the majority of studies have 4-year follow-up, and the findings of this study are updated by the last analysis of FREEDOM, where it was found that 45% of patients had the same outcome after PCI and CABG (30); (4) since this was not a randomized study, it could not deal with possible confounders which may guide clinicians in the decision-making process, such as bleeding risk, frailty, socioeconomic reasons or patients’ preference; (5) patients were treated with second generation DES; however no data on type of bypass graft were available but left internal mammary artery to left anterior descending artery is to be assumed; (6) patients are from the pre-SGLT-2 inhibitor and GLP-1 agonist and ARNI era.
Conclusions
Although CABG ensures less repeat revascularization than PCI, we showed that PCI could be a reasonable option in diabetics with a low SYNTAX (0–22) score. Furthermore, the general perception of diabetes and left main CAD as crucial decision-makers favoring CABG over PCI for complex CAD should be replaced with individualized risk assessment (including SYNTAX score and SYNTAX score II), discussion of potential late benefits following CABG, potential completeness of revascularization with PCI, patients’ adherence to the medical therapy and, most importantly, patients’ preference.







