








Introduction
Cervical esophagogastric anastomosis is the most important step in minimally invasive McKeown esophagectomy [1], but the incidence of anastomotic leakage is relatively high (6–26%) [2]. Anastomotic leakage can increase perioperative mortality and affect the postoperative quality of life and long-term survival [3, 4].There are many causes of anastomotic leakage, among which anastomotic technology includes anastomotic mode, anastomotic tension, transition path of tube-stomach, thoracic inlet width, etc. [5]. Therefore, it is necessary to improve the anastomotic mode, reduce the tension of the esophagus and stomach wall during anastomosis, and reduce the tears of the mucosa and muscle layer, so as to reduce the incidence of anastomotic leakage. At present, anastomotic devices are widely used in clinical practice. The operation methods of using the devices in the process of anastomosis are not uniform, and each has its own advantages and disadvantages.
Aim
The purpose of this retrospective study was to investigate the usefulness of the reversely connecting circular stapler technique for reducing anastomotic tension and injury of the esophageal and gastric wall during anastomosis, preventing anastomotic leakage in minimally invasive McKeown esophagectomy.
Material and methods
General data
Patient characteristics and surgical data were retrospectively analyzed. A total of 133 patients who underwent McKeown esophagectomy from January 2021 to December 2021 in the Department of Thoracic Surgery were collected and divided into the observation group (connecting the circular stapler in reverse order) and the control group (connecting the circular stapler in conventional order). There were 83 cases in the observation group and 50 cases in the control group. There was no significant difference in general clinical data between the two groups (p > 0.05) (Table I). This study was approved by the Ethics Committee of our hospital.
Table I
Comparison of general clinical data between the two groups
Surgical procedure
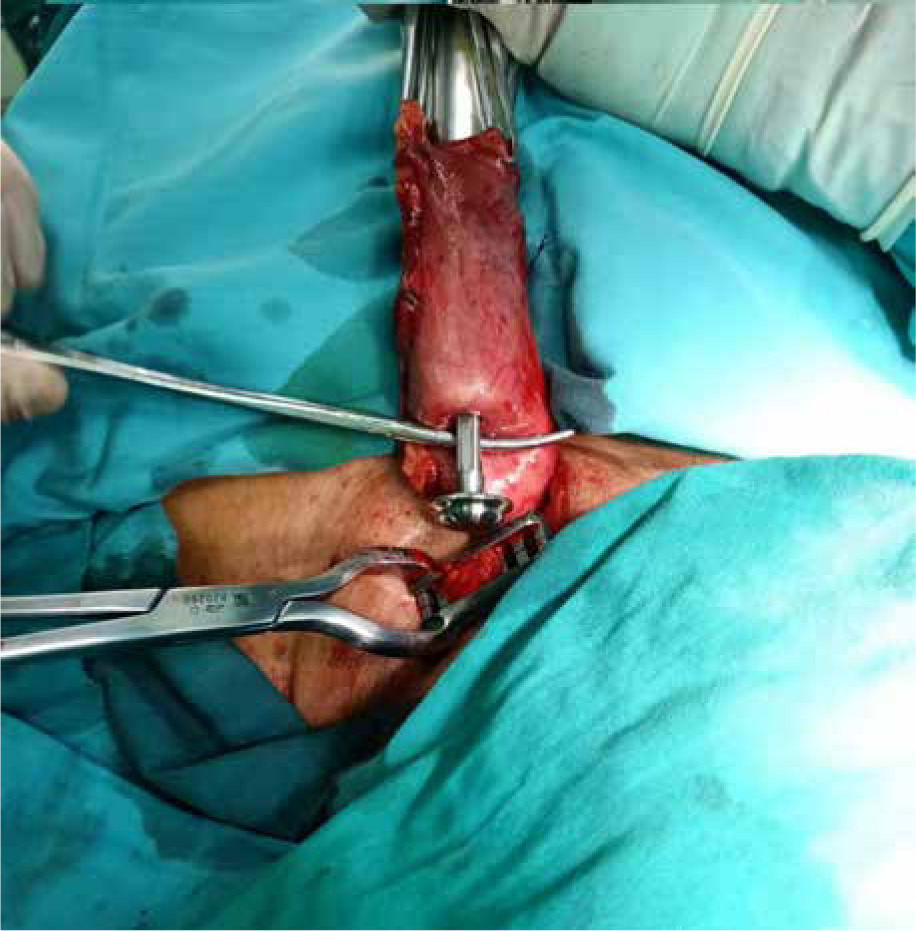
The general procedure of the operation was to dissociate the esophagus through the right thorax by the video-assisted thoracoscope, dissociate the stomach by the laparoscope, shape the stomach into a tube, and dissect the corresponding regional lymph nodes. Finally, esophagogastric anastomosis was performed on the left neck. Technical operation of reversely connecting the circular stapler: The cervical esophagus was carefully separated to avoid injury to the recurrent laryngeal nerve. The broken esophagus was sewn with purse strings and prearranged with purse strings. The tubular stomach was pulled approximately 4 to 6 cm outside the cervical incision (Photo 1). An incision of about 2 cm in diameter was made at the top of the tubular stomach, and the stapler body was inserted. At the scheduled anastomosis site, the full thickness of the gastric wall was cut in a microhole, and the central rod of the stapler body was fully perforated from the tubular stomach (Photo 2). The casing of the anvil head was connected exactly with the central rod of the stapler body (Photo 3). Then the central rod was withdrawn into the body of the stapler and retracted into the tubular stomach together with the anvil head cannula, exposing the cannula about 1.5 cm outside the stomach wall (Photo 4). The anvil head was placed in the broken end of the esophagus, and the purse string line was tightened and knotted (Photo 5). The central rod was further withdrawn so that the esophageal wall and gastric wall were closely combined, and the safety anastomosis label was clearly revealed (Photo 6). The front end of the stapler and the tubular stomach were fixed to maintain the gastric wall in a tension-free state to complete the esophagogastric anastomosis (Photo 7). Finally, the tubular stomach was closed about 1.5 cm from the anastomosis with a linear suture device, and the broken end was sutured with absorbable suture and embedded in the seromuscular layer. Full-thickness or seromuscular layer suture of the anastomosis was no longer performed.
Photo 1
Preset esophageal purse-string suture. The tubular stomach was pulled approximately 4 to 6 cm outside the cervical incision


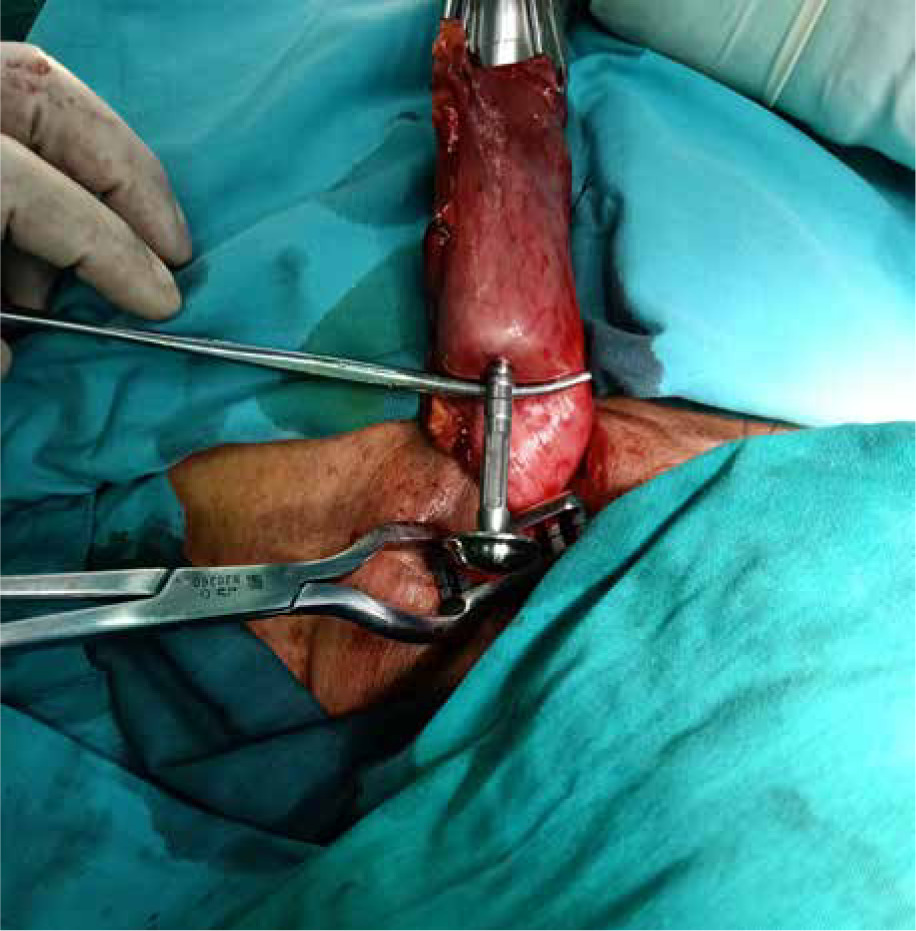
Photo 4
The central rod of the stapler body was withdrawn into tubular stomach, exposing the cannula about 1.5 cm outside the stomach wall



Operation process of conventional order connecting stapler: Firstly, the nail anvil was placed in the broken end of the esophagus in the cervical region, and the purse string was tightened. Secondly, the tubular stomach was pulled out through the cervical incision. An incision of about 2 cm in diameter was made at the top of the tubular stomach, and the stapler body was inserted. At the planned anastomosis site, the full thickness of the gastric wall was cut in a microhole, and the central rod of the stapler body was fully perforated from the tubular stomach. Thirdly, the central rod was connected with the anvil head cannula to complete the esophagogastric anastomosis. Finally, a linear cutting suture device was used to close the opening at the tip of the tubular stomach, and the broken end was sutured by the muscular and serosa layer. For those with poor anastomotic tissue fit, dehiscence of the esophageal muscle layer, or hematoma in the gastric wall, the absorbable suture was used for reinforcement and suture.
On the 5th to 7th postoperative day, esophageal angiography was performed, and cervical incision was performed for patients with anastomotic leakage or tubular gastric leakage. The juice diet was prescribed for patients without leakage before discharge, and those without discomfort were discharged.
Results
The median anastomotic time of the observation group and control group was 11 (7–25) min and 17.5 (14–21) min, respectively, and the difference was statistically significant (p < 0.001). The postoperative hospital stay in the two groups was 10 (7–35) days and 11 (9–82) days, respectively, and the difference was statistically significant (p < 0.001). There were 2 (2.4%) cases and 10 (20%) cases of anastomotic leakage in the two groups, respectively, and the difference was statistically significant (p = 0.002). There were 2 (2.4%) cases and 8 (16%) cases of postoperative hoarseness in the two groups, respectively, and the difference was statistically significant (p = 0.011). There were 6 (7.2%) cases and 10 (20%) cases of postoperative pulmonary infection in the two groups, respectively, and the difference was statistically significant (p = 0.028). There was 1 (1.2%) case and 6 (12%) cases of postoperative chest infection in the two groups, respectively, and the difference was statistically significant (p = 0.011). There was no perioperative death in the two groups (Table II).
Table II
Comparison of surgery-related indicators between the two groups
Discussion
Esophageal cancer has a high incidence and mortality in China, and surgery is still the main treatment [6]. With the socioeconomic level elevation and lifestyle modification, the population of esophageal cancer patients with high body mass index (BMI) values has increased in the past decades. High BMI is associated with prolonged operative time and increased blood loss. It also increases the incidence of anastomotic leakage [7]. With the application of thoracoscopy and robot-assisted techniques in minimally invasive McKeown resection of esophageal cancer, the incidence of trauma and cardiopulmonary complications caused by surgery has gradually decreased, but the incidence of anastomotic leakage is still high. Therefore, improving the anastomotic technique to reduce the incidence of anastomotic leakage is in demand and a difficult topic in thoracic surgery at home and abroad.
The three most widely used anastomotic techniques for esophagogastric anastomosis after esophagectomy are manual anastomosis, circular anastomosis, and linear anastomosis [8]. Manual anastomosis is the most classic surgical method, which has the advantages of flexible operation and low cost. However, it is greatly influenced by the anastomotic experience and suture technique of the surgeon, and the operation time is relatively long. Due to uneven needle spacing and ligation intensity, the blood microcirculation around the anastomosis is damaged, and there is still controversy in the prevention and reduction of anastomotic leakage. A nomogram prediction model study found that manual anastomosis was a high-risk factor for increasing anastomotic leakage of cervical esophagogastrostomy [9]. Another retrospective study found that esophagogastric anastomotic leakage was 14.67% in the manual anastomosis group and 5.33% in the stapler anastomosis group [10]. The semi-mechanical anastomosis is performed by suturing the posterior wall of the tubular stomach and the posterior wall of the esophageal stump with a linear suture device and then suturing the anterior wall of the tubular stomach and esophagus with manual suture or a linear suture device [11]. To some extent, the technical difficulty of manual anastomosis has been reduced [12]. However, the anastomosis requires a long and tumor-free esophagus, so this method is not suitable for resection of esophageal cancer at the thoracic entrance. Relevant studies have shown that this method has not reduced the incidence of anastomotic leakage [13]. Tan et al. [14] stated that triangular cervical anastomosis was a safe and effective method with an incidence of anastomotic leakage of 3.9%. However, the residual esophagus in the cervical region was required to be more than 3 cm, so the method is also not suitable for esophageal cancer at the thoracic entrance. Some studies have named this method T-anastomosis [15]. The incidence of anastomotic leakage was similar between circular anastomosis and triangular anastomosis [16]. In this study, the incidence of anastomotic leakage was 2.4% with the reverse connecting circular stapler technique, which was not statistically significant compared to 3.9% (3/77) in triangular anastomosis. However, the anastomotic time of 11 min was shorter than the triangular anastomosis time of 18.0 ±3.9 min, and the difference was statistically significant (p < 0.05).
With the widespread use of the tubular stomach in esophageal cancer surgery, it is very important to maintain good blood flow to the gastric wall during surgery to reduce anastomotic leakage. The use of a circular stapler for esophagogastric anastomosis has the advantages of reducing the difficulty of operation, shortening the anastomosis time, keeping the anastomosis of esophageal and gastric mucosa neat, and reducing the chance of infection around the anastomosis, which is conducive to the healing of the anastomosis [17]. However, in the clinical operation of the conventional anastomotic stapler method, due to the small cervical incision and relatively deep anatomical position of the esophagus, especially for esophageal cancer near the thoracic entrance, the residual esophagus is relatively short, and the range of motion is limited after the nail head is placed in advance. When connecting the body of the stapler and the anvil head, the linear distance between the esophageal stump and the intended anastomosis of the tubular stomach was 5 cm to 7 cm (Photo 8). In this process, the tubular stomach is subjected to excessive traction, which could easily cause gastric wall tear at the puncture site of the central rod. Especially when the length of tubular stomach is exposed shortly, the anastomotic effect of the posterior wall is often not ideal. Due to the small space of the cervical operation field, it is not easy to suture and repair. In clinical practice, we found that the posterior wall of the anastomosis had a slightly higher probability of leakage than the anterior wall, causing mediastinal or thoracic infection. Excessive stretching can also cause vasospasm and thrombosis in the gastric wall around the anastomosis, resulting in poor blood supply to local tissues, and eventually increasing the incidence of anastomotic leakage [18].

Therefore, it is necessary to improve the method of using the circular stapler to reduce the tissue tension in the anastomosis, prevent tears, and reduce the incidence of anastomotic leakage and gastric leakage caused by gastric wall necrosis. A previous study showed that the incidence of anastomotic leakage was increased by the ulcer of the stomach wall [19]. Chu et al. [20] improved the use of the circular stapler with the head of the nail anvil placed in the esophagus through the cervical incision and the stapler body placed in the stomach through the chest incision, which is completed through the two incisions of the cervical and chest. Although this method reduces the strain of the gastric wall and esophageal wall to a certain extent, it is not applicable in minimally invasive McKeown. Liang et al. [21] adopted a similar reverse piercing method, the specific operation method, where the hammer anvil casing head was introduced into the stomach cavity from the posterior wall of the tubular gastric, then the anvil head was placed into the residual esophageal cavity and the purse string was ligated, and the stapler host and the nail anvil head were merged in the stomach cavity for anastomosis. This method can reduce the tension to some extent, but the manipulation of the anvil head is poor, the visual field is narrow, the connection is difficult, and the operation field can easily be polluted.
Therefore, we performed the cervical esophagogastrostomy with an inverted junction stapler. The central rod of the stapler host was threaded from the tubular stomach to directly connect the nail anvil head, which reduced the probability of contamination of the operation field. The part of the central rod is turned back into the stapler host, which shortens the distance between the broken end of the esophagus and the tube stomach during the connection process, reduces the traction on the esophagus and gastric wall, prevents tearing, and effectively protects the blood supply of the gastric wall. Then the nail anvil head was placed into the residual esophageal cavity, and the purse string was ligated. Especially for the short residual esophagus, the nail head is inserted at the end, which can shorten the prolonged stress of the mucosa and protect the good blood supply of the esophagus. The incidence of anastomotic leakage after using this method was significantly lower than that of the conventional order connecting stapler group. In conclusion, this technique has strong controllability, no tension, and reduced contamination and anastomotic leakage.
Regarding perioperative complications, compared with the conventional order connecting stapler group, the inverse order connecting stapler method does not need the long cervical esophagus to be dissociated. This method not only protects the esophageal blood supply and benefits the healing of anastomosis, but also protects the recurrent laryngeal nerve in the tracheoesophageal groove and reduces the occurrence of hoarseness and complications such as lung and chest infection.
This study had some limitations. In addition to the anastomotic method, the occurrence of anastomotic leakage is also affected by postoperative nutritional support and other factors. No statistical analysis was conducted on nutrition-related indexes in this paper. Furthermore, since it is a retrospective study, there may have been selection bias in the patients enrolled.
Conclusions
The reversely connecting circular stapler technique could reduce the incidence of anastomotic leakage and tissue tension of the tubular stomach during the anastomosis process and shorten the anastomotic time. The technique is simple to perform and easy to learn. Therefore, it is useful for the prevention of anastomotic leakage.