
Introduction
Nasopharyngeal carcinoma (NPC) is a squamous cell carcinoma arising from the epithelium of the nasopharynx [1]. Rare in most parts of the world, this malignant disease is highly prevalent in South China, Southeast Asia, North-Africa, and the Arctic region [2]. The aetiology of NPC is unique and multifactorial, involving a complex interaction between Epstein-Barr virus (EBV) infection and environmental, genetic, and epigenetic factors [3].
Scientific evidence has shown that oxidative stress plays a major role in cancer initiation, development, and progression, and is a key factor in cancer resistance to various therapeutic approaches [4]. Oxidative stress results from an imbalance between reactive oxygen species (ROS) production in cells and the ability of the antioxidant system to detoxify these reactive products [5]. Recently, different studies reported that, depending on the concentration, ROS can influence cancer evolution in opposing ways; they can initiate tumourigenesis and support proliferation of cancer cells or cause cell death [6].
Inadequate levels of ROS and their reactive derivatives can damage cellular lipids, proteins, or nucleic acids, thus inhibiting signal transduction pathways, altering normal cellular functions and leading to chronic diseases and cancer [7]. Oxidative stress can be assessed directly by measuring ROS levels, or indirectly by analysing the products of oxidative damage that these radicals cause to the cell’s lipids, proteins, and nucleic acids, which are more accessible due to their longer half-life and their ability to diffuse from their place of origin [8].
Malondialdehyde (MDA) is the principal product of polyunsaturated fatty acid peroxidation. This highly mutagenic product can innate genotoxicity and consequently cancer initiation and development [9]. Malondialdehyde is one of the most studied end-products of lipid peroxidation (LPx) and has been suggested as an oxidative stress biomarker in numerous malignancies, including NPC [10]. In NPC, the main challenge for clinicians is to identify reliable and sensitive biomarkers that may be used for disease diagnosis and prognosis. In this field, the current study was designed to assess serum levels of MDA as a biomarker of LPx in patients with NPC before and after chemo-radiotherapy (CRT), as well as to determine its potential relevance as a biomarker in disease diagnosis and prognosis. For this purpose, we investigated its association with NPC patients’ clinical characteristics, EBV DNA load, and 4-years survival outcomes.
Material and methods
Patients and controls
Between January 2017 and February 2019, 112 untreated patients with histologically confirmed NPC were recruited from Casablanca’s Mohammed IV Centre for the Treatment of Cancer. Forty-one healthy age- and gender-matched individuals, with no personal history of cancer or other chronic disease, were used as controls. Face-to-face interviews were conducted with all participants to collect socio-economic data, such us age, sex, family history of cancer, tobacco habits, alcohol consumption, and childhood habitat. Clinical data, including histological type, clinical stage, and patient’s survival, were obtained from respective medical records. The study protocol was approved by the Ethics Committee of Ibn Rochd Hospital of Casablanca, Morocco in November 2017. Because this was a prospective study, written informed consent was obtained from each patient at recruitment. The study was carried out in accordance with all relevant guidelines.
Patients’ follow-up
Recruited patients were followed until February 2021 or until loss to follow-up or death. Blood sampling was performed at recruitment and after treatment achievement (±3 months). Patients were treated by concurrent CRT with or without neoadjuvant chemotherapy depending on their disease stage. Accordingly, patients were given a median dose of 50 Gy in the nasopharyngeal tumour area and 66 Gy in the involved lymph nodes. A daily fraction of 2 Gy was delivered 5 times per week, and the treatment was completed within 5 to 7 weeks.
Overall survival (OS) was defined as the interval from the date of diagnosis to the last follow-up or date of death from any cause. Locoregional recurrence-free survival (LRRFS) was defined as the interval from the date of diagnosis to the first evidence of radiological or histological loco-regional recurrence, death from any cause, or last follow-up. Distant metastasis-free survival (DMFS) was defined as the interval from the date of diagnosis to the first evidence of radiological distant metastatic lesion, death from any cause, or last follow-up. Progression-free survival (PFS) was defined as the time from the diagnosis to progression of disease, death, or last follow-up (whichever occurred first).
Blood sampling
Whole blood of NPC patients and healthy controls was collected by venipuncture into an appropriate collection tube. Plasma and serum were recovered and conserved at –80°C until use.
Epstein-Barr virus DNA quantification
DNA extraction and circulating EBV DNA quantification were performed as previously described [11]. Briefly, 200 µl of plasma was used to extract DNA using a QIAamp DNA Mini Kit (Qiagen, France). Real-time quantitative polymerase chain reaction was used to assess circulating EBV DNA, and results were expressed as International Unit/ml (IU/ml).
Measurement of malondialdehyde levels
Total protein content quantification was performed by Bradford method using bovine serum albumin as a standard (Bradford, 1976). Malondialdehyde status was evaluated using the method of Samokyszyn and Marnett, based on the release of colour complex due to the reaction between thiobarbituric acid (TBA) and MDA [12]. Briefly, 100 µl of serum was added to 10% trichloroacetic and 0.67% of TBA. The mix was heated for 30 min at 100°C in a dry bath incubator, cooled on ice, and then centrifuged for 10 min at 8000 g. Thereafter, the supernatant was used to evaluate spectrophotometrically MDA/TBA complex at 532 nm. Serum MDA levels were expressed in µmol/ml/µg of protein (p).
Statistical analysis
Descriptive statistics were calculated and presented as numbers, percentages, and means±standard deviation (M ±SD). The χ2 test was used to compare characteristics of NPC patient and controls groups. The Mann-Whitney U test was used to compare serum MDA levels between groups. For survival comparison, patients were divided by median levels of MDA before treatment in cancer patient groups; OS, LRRFS, DMFS, and PFS curves of MDA groups were plotted with the Kaplan-Meier method and compared with the log-rank test. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 22.0 for Windows. An association was considered significant at a p-value less than 0.05.
Results
The baseline characteristics of the study population are shown in Table 1. Overall, 59% (66/112) were males and 41% (46/112) were females, with a sex ratio of 1.43. Most patients were above the age of 30 years (74.1%), 16% of cases were smokers (18/112), and 12.5% were alcohol consumers (14/112). Histopathological distribution was performed according to the WHO classification and showed a predominance of type 3, found in 94.6% of cases (106/112).
Table 1
The baseline characteristics of nasopharyngeal carcinoma patients included in the present study
Clinical staging, performed according to the American Joint Committee on Cancer tumour-node-metastasis (TNM) classification system, showed a predominance of T3–T4 class, found in 75.8% of cases (85/112), and N2–N3 class, found in 66.9% of patients (75/112). Moreover, 33% patients were diagnosed with distant metastasis (37/112) and 88.4% with III–IV UICC stages (99/112).
The comparison of characteristics of patients and controls (age, gender) using the χ2 test, showed no significant differences in age and gender frequencies between the NPC patients and control groups (p > 0.05) (Supplementary Table 1).
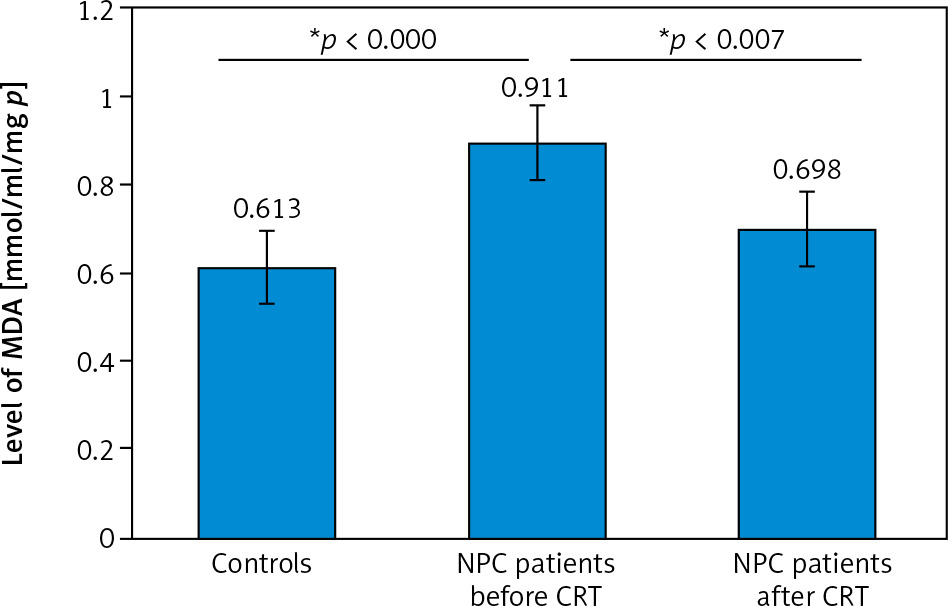
Malondialdehyde levels in the serum of NPC patients before and after CRT, as well as in the control group, are reported in Figure 1. The mean MDA level of NPC patients at recruitment was 0.911 µmol/ml/mg, which was significantly higher than the mean MDA level found in the control group (0.613 µmol/ml/mg, p = 0.000). After CRT, the mean MDA level dropped significantly to 0.698 mol/ml/mg of protein (p = 0.007). It is also worth noting that there was a statistically significant difference between MDA levels in patients after CRT and healthy controls (p = 0.16).
Fig. 1
Variation of malondialdehyde levels in the serum of nasopharyngeal carcinoma patients before and after chemo-radiotherapy and in the control group
CRT – chemo-radiotherapy
*Statistically significant threshold was set at p < 0.05 determined by Mann-Whitney U test.
Assessment of the association between MDA status and, NPC patients’ characteristics and clinical features are reported in Tables 2 and 3, respectively. Our data did not show any significant association between MDA level and patients’ characteristics such as age, gender, cigarette smoking, or alcohol consumption (p > 0.05).
Table 2
Variation of serum malondialdehyde levels according to age, gender, cigarette smoking, and alcohol consumption status of nasopharyngeal carcinoma patients
Table 3
Variation of serum malondialdehyde levels according to tumour-node-metastasis classification, stage of disease, and Epstein-Barr virus DNA load of patients with nasopharyngeal carcinoma
Regarding clinical features, a highly significant association was found between MDA status and disease stage, with MDA levels being higher at advanced disease stages III–IV (0.966 µmol/ml/mg) as compared to earlier stages I–II (0.492 µmol/ml/mg) (p = 0.001). Furthermore, borderline significance was shown between MDA status and tumour grade (p = 0.09). In fact, MDA levels were slightly higher in NPC patients with high tumour grades T3–4 (0.954 µmol/ml/mg) than in those with low tumour grades (0.777 µmol/ml/mg). However, no significant association was obtained between MDA status and lymph node involvement, metastatic status, or EBV DNA load (p > 0.05).
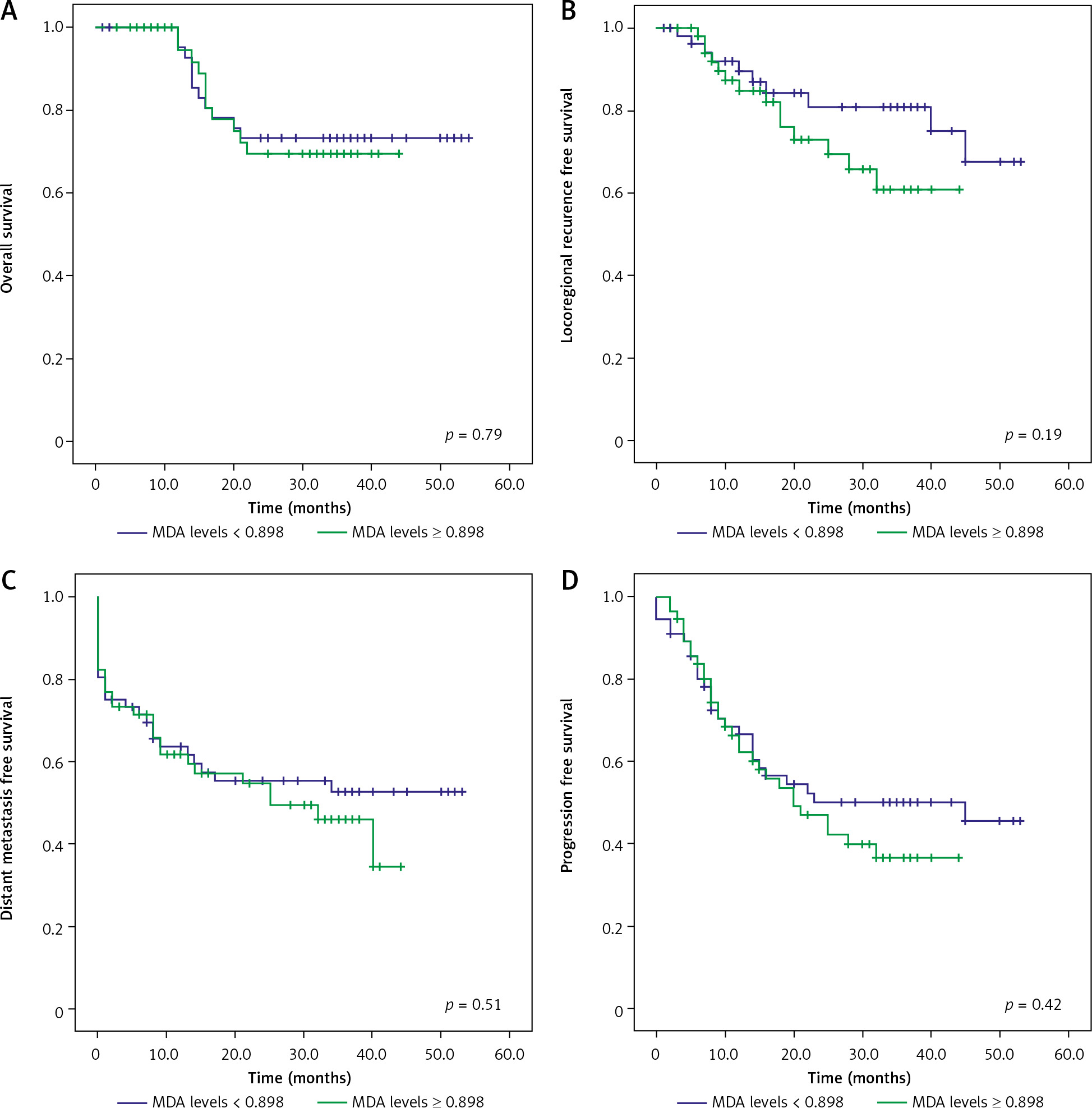
The association between MDA levels and patients’ 4-year survival outcomes, including OS, LRRFS, DMFS, and PFS, was also investigated in this study, and the results are presented in Figure 2. Interestingly, patients with high serum MDA levels at recruitment had lower OS, LRRFS, DMFS, and PFS rates than those with low MDA levels, although this difference was not statistically significant (p > 0.05).
Discussion
Worldwide, extensive research has highlighted the key role of ROS in cancer initiation and progression. Reactive oxygen species levels can be assessed directly or indirectly by measuring MDA levels, a cytotoxic and mutagenic component derived from LPx [9]. There are currently limited data on the association between MDA level and NPC, and to the best of our knowledge, no research has addressed the variation of serum MDA levels in NPC patients before and after treatment. The main finding of the present study was that serum MDA levels in NPC patients were significantly higher before treatment compared to healthy subjects (p < 0.000), and that they decreased significantly following CRT treatment (p = 0.007). These results are in agreement with previously reported studies showing elevated MDA levels in the tissues and serum of NPC patients [10]. Similar results were reported in other cancers including oropharyngeal cancer [13], ocular carcinoma [14], breast cancer [15], and bladder cancer [16], highlighting the interest to consider MDA status as a potential biomarker of cancer development and progression. In fact, scientific evidence has shown that disrupted tissues undergo peroxidation more quickly than healthy ones [17].
Malondialdehyde has also been shown to act as a tumour promoter and co-carcinogen by interacting with cellular DNA and generating MDA deoxyguanosine (M1-dG), a DNA-MDA covalently bonded adduct, resulting in DNA damage and DNA repair interference. Also, by binding to cell membrane proteins, it induces profound changes in their function, permeability, and structural integrity [18].
Several studies have linked aging, hormones, and environmental factors (smoking and alcohol consumption) to both oxidative stress status and risk of cancer [19], so we further investigated the association between patients’ characteristics and serum MDA levels. However, no significant association was found between MDA levels and patients’ variables such as age, gender, cigarette smoking, and alcohol intake. According to Benz and Yau, oxidative stress plays a role in the development of age-related malignancies, although the underlying carcinogenic mechanism of this molecule remains unknown [19]. In this context, other oxidative stress markers should be evaluated to fully elucidate this association, especially in NPC patients from North African countries, where this malignancy affects both children and adults.
Sex hormones might also influence oxidative stress. In fact, previous research has shown that oestrogens in women play a protective role against oxidative stress-related disease by upregulating the expression of antioxidant- associated genes [20]. Several studies reported a strong association between cigarette smoking and alcohol consumption, and MDA status. Nagamma et al., reported that smoking patients with breast cancer have significantly higher levels of oxidative stress and lower levels of antioxidants, compared to non-smoking patients (mean of MDA levels of smoking patients: 5 ±1.2 nmol/ml vs. non-smoking patients: 2.56 ±1.2 nmol/ml) [21]. Similarly, alcohol consumption was linked to increased ROS and decreased total antioxidant activity in cancer patients of all types [22].
Results of the present study clearly showed that patients at advanced clinical stages (III–IV) of NPC had a significantly higher level of LPx in their serum than those at early disease stages (I–II) (0.966 vs. 0.492 µmol/ml/mg, p = 0.001). These results corroborate those of several previous studies that have linked increased oxidative stress to tumour progression in many cancers [15]. Indeed, a significant association between serum MDA levels and colorectal cancer progression was observed [23]. Similarly, a positive correlation was reported between oxidative stress levels and bladder cancer progression [24]. In this field, oxidative stress might modulate the expression of proangiogenic factors, including VEGF and MMP-9, by increasing transcriptional factors binding to their promoter regions, which influences significantly tumour progression [25].
In NPC, the EBV, which is consistently associated with NPC development and progression, was also reported to be implicated in the genesis of ROS and/or activation of ROS-associated signalling pathways [10]. Moreover, it has been established that ROS contributes to the reactivation of the EBV lytic cycle in the early stages of cancer development, through induction of BZLF-1 gene expression [26]. However, despite the established link between ROS and EBV reactivation, and evidence that increased ROS activates EBV lytic cycle in NPC [27], no study has evaluated the correlation between MDA levels and EBV DNA load in NPC patients. In the present study, no significant association between MDA status and EBV DNA load was observed. In contrast to these results, a positive correlation between MDA levels and anti-EBV IgA and VCA antibody titres was reported in a Tunisian study conducted on 21 patients with NPC [10]. This difference could be due to the technical approach and/or the sample size. Further studies are therefore needed to elucidate the link between EBV and oxidative stress in NPC.
The association between serum MDA levels and patients’ outcomes was further assessed to determine whether it could be used to predict the prognosis of NPC. Overall, patients with high serum MDA status were found to have lower OS, LRFS, DMFS, and PFS rates, although the association was not statistically significant (p > 0.05). In contrast, Salzman et al. showed a significant relationship between MDA levels and the recurrence of squamous cell carcinoma of the oral cavity and oropharynx (p > 0.05) [28].
One of the limitations of the present study is that it focused on a single oxidative stress marker: “MDA levels”, and the evaluation of other oxidative stress markers in NPC diagnosis and prognosis would be preferable. Another limitation of the study is that all patients were enrolled and treated in a single medical centre, and the generalizability of the result may be limited. Further large-scale studies are needed to validate our findings.
Conclusions
In conclusion, high serum MDA levels in NPC patients before CRT, as well as their increase with disease stage, accurately reflect the elevated oxidative stress level in NPC, suggesting that the MDA serum level could be a useful biomarker in the diagnosis and progression monitoring of NPC.






