
Degenerative aortic valve stenosis (AS) is the most frequent reason for referral to hospital for valvular heart disease. Despite the advent and widespread availability of transcatheter aortic valve implantation (TAVI) in the last fifteen years, the European Society of Cardiology (ESC) valvular disease survey II demonstrated that 20% of patients with a class I recommendation for valve replacement according to international guidelines actually do not undergo the procedure [1]. As a consequence, a portion of patients with symptomatic AS, typically with high surgical risk, frailty, haemodynamic instability, multiple comorbidities, and old age, are treated with medical therapy and maybe balloon aortic valvuloplasty (BAV) [2].
Notably, 3% to 20% of patients enrolled in TAVI registries suffer from concomitant moderate-to-severe mitral regurgitation (MR) [3, 4]. A meta-analysis including eight studies, with more than 8 000 patients, demonstrated that MR severely impacts overall 30-day and 1-year mortality (odds ratio (OR) = 1.49, 95% CI: 1.16–1.92; hazard ratio (HR) = 1.32, 95% CI: 1.12–1.55, respectively) [5]. As for the aetiology, degenerative MR seems to be associated with increased risk of 2-year cardiovascular death (adjusted HR = 2.21, 95% CI: 1.4–3.49, p = 0.001) compared to functional MR (adjusted HR = 1.13, 95% CI: 0.59–2.18, p = 0.707) [6].
The Study to Improve Outcomes in Aortic Stenosis (IMPULSE) showed that grade III or IV MR was more frequent in symptomatic than asymptomatic patients with severe AS (11.6% vs. 7.1%; p = 0.008), and particularly in those who were denied valve replacement (17.5% vs. 9.1%; p < 0.001) [7]. Indeed, MR is one of the comorbidities sometimes affecting the indication for TAVI or surgical valve replacement (SAVR). A large registry evaluated the role of BAV as a bridge-to-decision in selected patients and showed a post-procedural reduction of moderate-to-severe MR prevalence from 16.3% at baseline to 11.5%. After a second heart team assessment, 70.5% of patients with MR reduction finally became eligible for SAVR/TAVI [8].
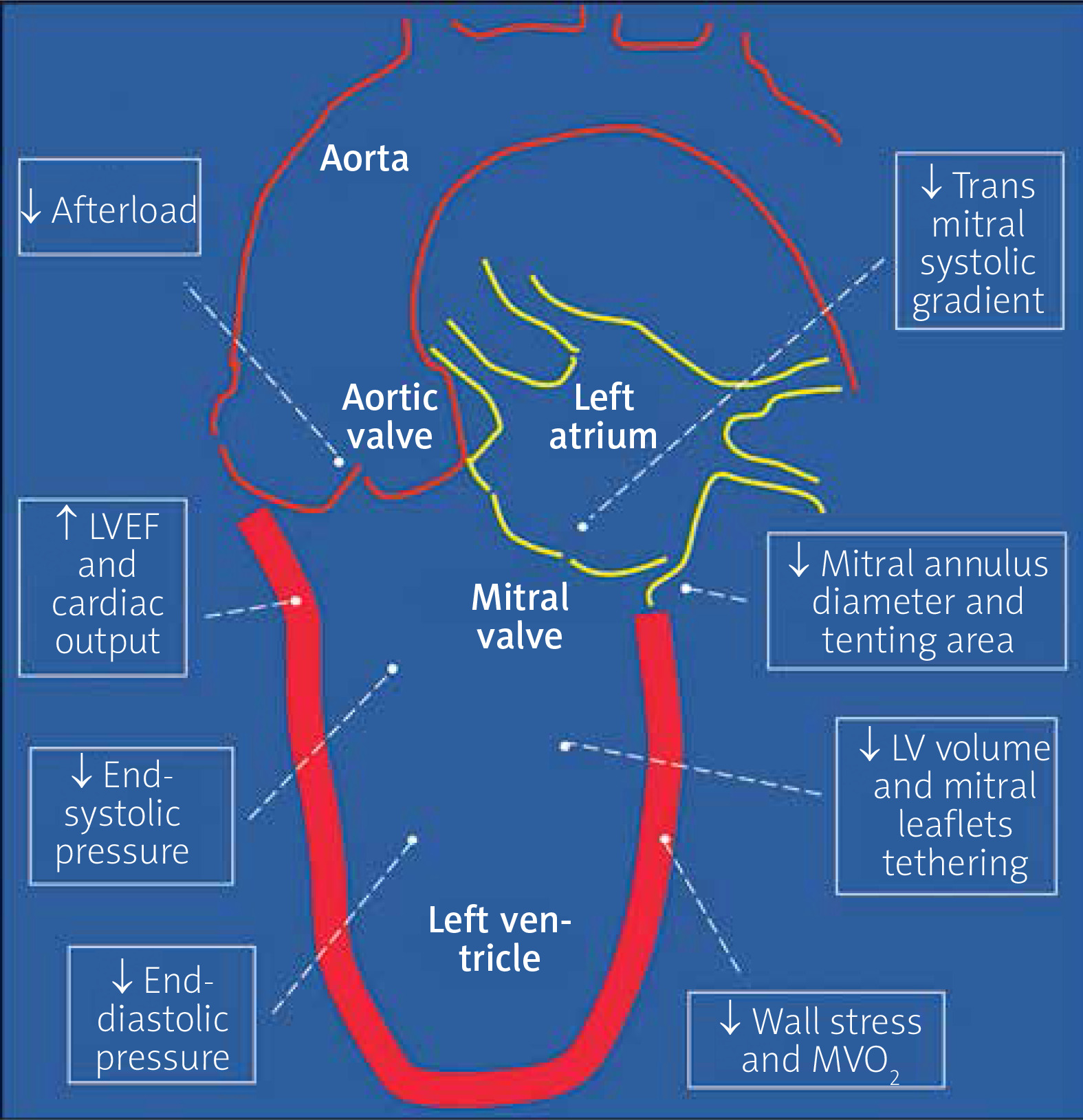
In this issue of the journal, Kleczynski et al. illustrated the results of a retrospective analysis of 271 patients with high-gradient AS undergoing BAV from two high-volume centres, assessing separately the echographic outcome of those with (n = 85, 21.2%) and without (n = 186, 78.8%) moderate-to-severe MR. In the former group, several echo parameters significantly improved from baseline to both 30-day and 6-month follow-up, including left ventricle (LV) end-diastolic and end-systolic diameter, left ventricle ejection fraction (LVEF), mean transaortic gradient, aortic valve area and, notably, mitral regurgitation jet area and percentage ratio between MR and left atrium area. Predictors of MR persisting at mid-term were degenerative MR and changes of end-systolic diameter, LVEF, and MR jet area between baseline and 30-day evaluation. The potential beneficial effect of BAV in AS patients with concomitant MR is provided by the reduction of LV afterload, which may lead to cascading haemodynamic effects such as a reduction of LV filling pressure, transmitral systolic gradient, and reverse remodelling of the LV along with improved mitral valve geometry (Figure 1) [9–11]. This is in line with the results of Masaki et al. showing that the haemodynamic changes are favourable irrespective of MR aetiology, but the reduction of LV volume seems to confer a greater advantage in type I and IIIb according to Carpentier’s classification [12]. Therefore, since BAV may exert a favourable effect mainly in functional MR, the echographic evaluation of mitral valve anatomy and mechanics is of paramount importance. A second observational study found that almost half of the patients with severe AS and coexistent MR had an improvement of the latter after BAV. Only left atrial dimension (OR = 3.37; p = 0.006), LV end-diastolic dimension (OR = 2.7; p = 0.04), and mean transaortic gradient (OR = 1.04; p = 0.05), but not LVEF or functional MR, correlated with MR reduction [13].
Figure 1
Potential positive haemodynamic and structural changes that may be observed after reducing the left-ventricle afterload excess in patients with severe aortic valve stenosis
LVEF – left ventricle ejection fraction, LV – left ventricle, MVO2 – myocardial oxygen consumption.
In the present study the procedural success rate was high (94.6%), as expected considering it was defined as a 30% reduction of the mean transvalvular gradient. Furthermore, the long-lasting haemodynamic advantage of BAV at 6 months is a tangible marker of procedural efficacy in this subset of patients. As in the registries reported above, there is a limitation due to the absence of data from patients who died (likely the most frail and sick) and those who underwent TAVI/aortic valve replacement (AVR) (likely with the least burden of comorbidity). A second limitation may be related to the risk of MR overestimation using the colour Doppler jet area estimation in severe AS, due to an increased trans-mitral systolic gradient. The issue could be overcome by means of three-dimensional echocardiographic study of the vena contracta and proximal isovelocity surface area (PISA), which is supposed to be less afterload dependent [11].
BAV is the first technique that a trainee interventional cardiologist must acquire when approaching structural procedures. The technique retraces many key steps of TAVI, such as the management of medium-bore vascular accesses, aortic valve crossing, extra-supportive wire positioning within the LV, rapid pacing through a temporary pacemaker or supportive wire, haemodynamic evaluations of the results, preliminary study of the aortic annulus size and proper angiographic projections. Studies comparing a bridge-to-TAVI strategy over a direct-TAVI brought conflicting results. To date, we cannot recommend BAV in every high-risk patient, irrespective of coexistent MR, to lower the procedural risk of TAVI or AVR [2]. In view of current evidence and recommendations, some authors suggest that BAV should be performed after patient evaluation in the heart team. On the other hand, observational data teach us that the waiting time for TAVI is burdened by significant risk of death and heart failure hospitalization [14]. Since prolonged waiting for TAVI is a common problem across Western countries, despite not being supported by specific evidence, BAV may contribute to a reduction of morbidity before valve replacement in high-risk patients.
Besides being part of the TAVI procedure when pre- or post-dilatation is needed, in current practice, according to international recommendations, BAV is usually performed in patients at high surgical risk, with haemodynamic instability, reduced LVEF, moderate-to-severe MR, cognitive impairment, frailty, and severe comorbidities such as lung disease, peripheral vasculopathy, chronic kidney disease, hip fracture, and cancer [9, 15]. However, the overall complication rate has diminished over time in the last decades, thanks to operator experience, technical improvements, and use of smaller vascular sheaths. Indeed, BAV remains a useful treatment option for patients transiently or definitively excluded from surgical and transcatheter valve replacement, as demonstrated by several studies which reported an increased number of procedures performed worldwide [2]. To quote an American movie from the 1970s: when the going gets tough, the tough get going.







