
Coronary artery bypass grafting using the right and left internal mammary artery (BIMA) is currently the most durable surgical treatment for coronary artery disease [1]. This is due to the use of arterial (rather than venous) material, which has the proven advantage of durability. In addition, avoiding central aortic anastomosis by direct subclavian artery blood supply through the left (LIMA) and right (RIMA) internal mammary arteries, thus aorta manipulation, is associated with lower risk of stroke [2]. Another advantage is no additional wound for graft harvesting (as for the radial artery). Harvesting both internal mammary arteries usually requires access via sternotomy, which is associated with a higher risk of worse wound healing, increased postoperative pain, and longer rehabilitation [3]. The use of the da Vinci robot for coronary artery bypass grafting is a valid and elegant alternative to surgery via sternotomy as it combines the advantages of arterial revascularization using BIMA without opening the sternum [4]. In this letter to the editor, we present the first Polish experience of coronary revascularization using the da Vinci robot based on treatment of significant stenosis in the distal segment of the left main coronary artery.
A 66-year-old patient with coronary artery disease, hypertension and gout was admitted to the Department of Cardiac Surgery of the Central Clinical Hospital of the Ministry of Interior and Administration, Centre of Postgraduate Medical Education in Warsaw for surgical treatment. The patient had recently reported stenocardial symptoms on slight exertion (CCS class II). Coronary angiography revealed a significant lesion in the distal segment of the left coronary artery. Resting echocardiography showed no segmental wall motion abnormalities with ejection fraction estimated at 60% and no significant valvular lesions. The patient was qualified by the local Heart Team for surgical coronary revascularization using the da Vinci robot.
The operation was performed on March 15, 2021. The patient was placed on his back with a small roll under the left scapula. A double-lumen tube was used for intubation and the left lung was deflated. Skin ports for the three robotic arms were placed in the 2nd, 4th and 6th intercostal space on the left side of the chest. The port in the 4th intercostal was used to introduce the endoscope, while the ports in the 2nd and 6th intercostal were used to introduce the robotic tools for mono- and bipolar electrocoagulation and for vascular clips (Figure 1). First, the anterior mediastinum was opened, gaining access to the right pleural cavity. The right internal mammary artery was harvested as a hemi-skeletonized artery with both accompanying veins but not clipped. In the next step, the arms were retracted into the left pleural cavity and the left internal mammary artery was harvested using the same technique (Figure 2). Next, the pericardial fat tissue was removed and heparin 1 mg/kg was administered. The pericardial sac was then visualized and opened longitudinally. The fat peeled of LIMA and RIMA was attached to the opened pericardial sac for prevention of twisting. Finally, the distal portion of the LIMA and RIMA was clipped by a medium clip applier and both arteries were cut off distally. The coronary arteries were located and the sites of the two distal anastomoses identified. The optimal skin incision was also determined by robotic assistance under normal CO2 pressure using standard needle guidance. The robot was completed and the skin ports were removed.
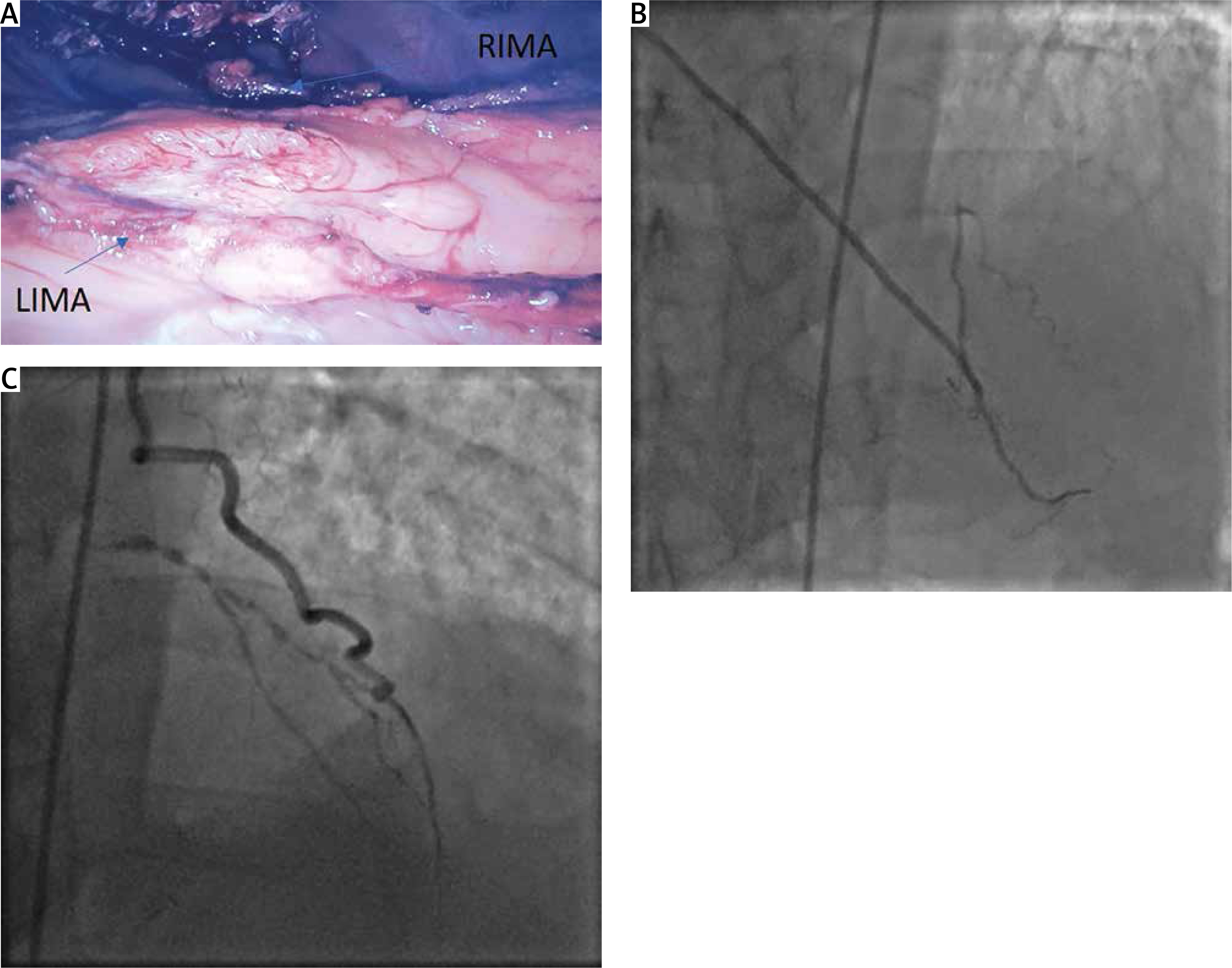
Figure 1
Endoscopic view of the two harvested internal mammary arteries (A); coronary angiography with anastomosis of RIMA to LAD (B) and LIMA to OM (C)

In the second stage of surgery, a left 4 cm anterior minithoracotomy was performed in the 4th intercostal space. The marginal obtuse artery (OM) was exposed using a tissue stabilizer and sutures to stabilize the position of the pericardial sac. LIMA-OM anastomosis was performed using Prolene 8-0 suture. In a next stage, the left anterior descending artery (LAD) was prepared by analogous maneuvers. The RIMA-LAD anastomosis was performed using Prolene 8-0 suture. The anastomosis was covered with pericardial fat. The intercostal space was closed with layered sutures, leaving two drains in the right and left pleural cavities.
The patient was transferred to the intensive care unit after surgery, where he was extubated and mobilized immediately. The total drainage was 250 ml and was removed on postoperative day 1. A follow-up chest X-ray showed no features of emphysema or pleural fluid. The patient’s pain score on the 11-grade NRS scale was a maximum of 3 points. The patient was discharged home 72 hours after the operation. At 1, 3- and 6-month follow-up, the patient had no recurrence of angina and no postoperative wound pain.
The Da Vinci Xi is the latest generation of robot consisting of three parts: surgeon console, patient cart and vision cart. The modules are connected and integrated with each other by optical fiber, which ensures smooth and precise operation. The operator sees the surgical field in 3 dimensions and has 3 or 4 working ports available. During our robotic experience we have significantly reduced the number of instruments, and thus the cost of the procedure. It is possible to perform robotic BIMA harvesting using 5 instruments as a 3D camera with a 30° angle, mono- and bi-polar coagulation, small and medium vascular clips.
The harvested arteries are long and can be used for lateral wall heart grafts [4]. The LIMA is longer than in MIDCAB due to the ideal visualization of the vessels in the 3D camera and their complete retrieval even in difficult anatomy (women or men). The robotic harvesting of both internal mammary arteries itself is possible, although it requires gaining experience with the left internal mammary artery. The closed chest does not disturb the distance between the thoracic arteries and the coronary vessels as in open sternotomy. A small 4 cm thoracotomy is enough for performing both anastomoses due to precise localization of the chest incision during the robotic stage. The operation time with BIMA of approximately 200 minutes is slightly longer, but does not affect the rapid hospital pathway.
In our experience, pain after the robotic surgery is significantly less than after other cardiac surgery. Compared to minimally invasive direct coronary artery bypass (MIDCAB) surgery, patients require lower doses of pain killers (no rib traction during LIMA harvesting). Reduced pain and sternal stability enable rapid patient mobilization. Rapid recovery after robotic surgery is a reported advantage in the literature [5]. The procedure can be performed by most cardiac surgeons, especially by young specialists after relatively fast and intensive training.
In our opinion, robotic BIMA is the very efficient and elegant combination of the well-documented advantage of the totally arterial, anaortic revascularization and minimally invasiveness, and is one of the most underrated cardio-surgical procedures.









