
Introduction
Cancer of the head and neck is an umbrella term encompassing cancerous lesions developing in and around the oral cavity, pharynx, larynx, paranasal sinuses, nasal cavity, and salivary glands. With non-communicable diseases accounting for about 63% of all deaths in India, cancer is the primary cause of around 9% of them [1].
Notable approaches to the therapeutic modalities for the treatment of cancer involve surgery, chemotherapy, radiotherapy, targeted therapy, and immunotherapy [2]. Radiation therapy (also known as radiotherapy) is a cancer treatment that uses high doses of radiation to kill cancer cells, limit the development and spread of malignant tumours, and shrink benign tumours.
While focussing on controlling the existing cancerous lesion must be the priority, constricted access to psychotherapy during standard cancer treatment results in unforeseen anxiety and other psychological issues. The diagnosis and therapy seem to have a negative influence on the patient’s quality of life (QOL) as well as that of their caregivers; hence, a secondary focus on their mental health should be the need of the hour [3].
Patients diagnosed with head and neck cancer (HNC) are often subjected to an array of unprecedented challenges, which have seldom been scrutinized in other cancers, such as prolonged restrictions in their capacity to breathe, speak, and swallow, considerable deformity, and an alleviated risk of death [4]. These difficulties have a significant impact on the psychological well-being of patients. Head and neck cancer patients have significant rates of emotional distress, with heightened depression and anxiety symptoms prevalent at all stages of the disease [5]. What is of significance is that as well as the patient, also the caregiver’s psychosocial health is at risk during the treatment periods, which may produce a rift in their personal and professional commitments, causing their level of stress to be higher than usual.
Cortisol is a glucocorticoid hormone that is widely recognised as one of the body’s primary stress hormones [6]. Cortisol levels have been linked to a variety of psychological conditions, including anxiety and depression [7, 8]. Salivary cortisol estimation is one of the most widely employed methods by doctors to estimate the stress levels in people [8].
Upon a thorough literature review, seldom have the caregivers been given a thought, and hence this study is the first of its kind conducted in the Indian population, to create awareness among healthcare workers and authorities about the distress and anxiety affecting caregivers. The result of this study can be utilised for effective management of stress among the caregivers and thereby provide better care for the patients. It will, in fact, provide assistance to the healthcare professionals to extend the support to the caregivers accordingly. Improvements in caregiver’s QOL may have a direct impact on patient’s QOL. Therefore, this study aims to assess the cortisol levels, the burden, and the QOL of the caregivers of HNC patients undergoing radiotherapy.
Material and methods
The current study was a prospective cohort study among 28 caregivers of patients undergoing radiotherapy for HNC attending a tertiary care hospital in Mangalore, Karnataka. Data were collected for the study from 30 August to 4 November 2021. Before initiating the study, official permission was obtained from the concerned authorities. Ethical clearance was obtained from the institutional Ethics Committee (YEC2/896). Informed consent was obtained from the eligible study participants followed by saliva collection and a pre-validated questionnaire. The Caregiver Quality of Life Index-Cancer (CQOLC) scale was distributed among the participants to assess their QOL on the 1st, 14th, and 21st day of radiotherapy [9].
The principal investigator assessed the eligible participants who were selected for the study using the simple random sampling method. All of the salivary samples of the selected participants were collected on day 1, day 14, and on day 21 of the radiotherapy sessions. Regarding the patients’ details, the mean patient age was 51.9 ±15 years, 54% of them were males, and 46% were females. They had been diagnosed with HNC, including oral cavity (46%), oropharynx (39%), and larynx/hypopharynx (14%). Sixty-four per cent of the patients had a stage 1 diagnosis, and 36% had a stage 2 diagnosis. Squamous cell carcinoma was the most common type of cancer in this study (72%) with all of them undergoing radiotherapy. No participants had a history of prior surgery. All participants received radical therapy. The radiation dosage was 2 Gy per fraction, 5 fractions per week, for a maximum of 30–33 fractions.
Simultaneously, a pretested validated questionnaire (CQOLC) with 35 questions, which were measured on a 5-point Likert-type scale (from 0 “not at all” to 4 “very much”), was given to be filled out by the participants. In addition to a total score achieved by summing up 35 (range from 0–140 for the overall scale), there were 4 subscales: burden (10 items), disruptiveness (7 items), posi-tive adaptation (7 items), and financial concerns (3 items).
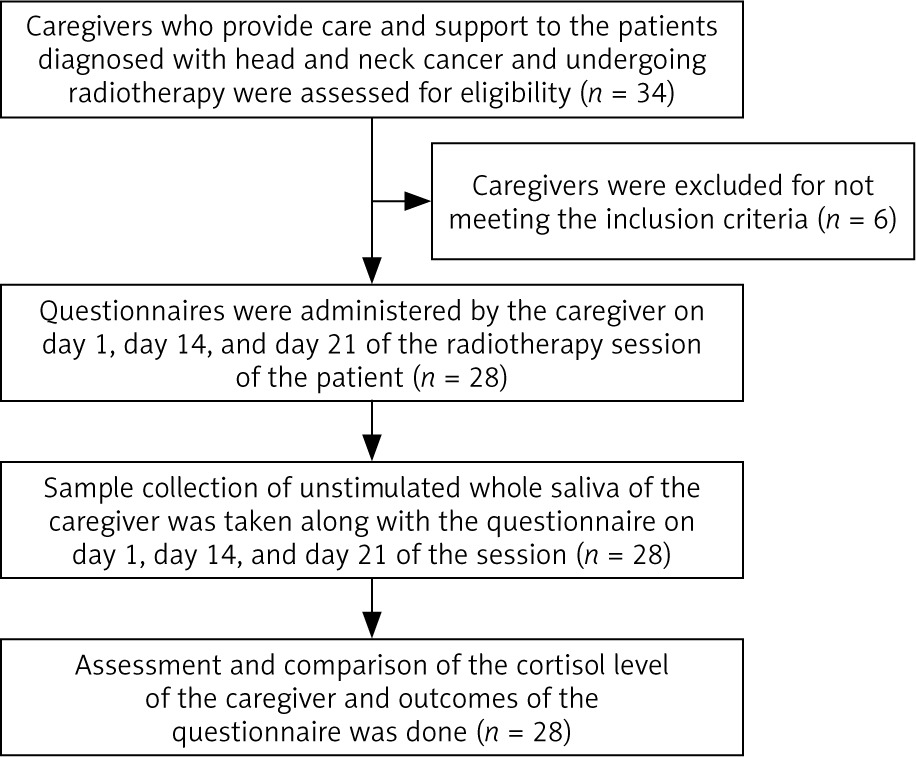
The total possible score was 140, with lower scores representing better QOL. The composite measurement scale questioned the caregivers’ condition throughout the previous 7 days. Enrolment of participants is shown in Figure 1. Internal consistency was determined by Cronbach’s α. The internal consistency in this study was 0.88, which can be considered as good. The participants were given written instructions beforehand regarding the saliva collection and were instructed not to eat or drink for at least an hour prior to the sample collection. Five ml of unstimulated saliva was collected from the participant (caregiver), 1 hour prior to the initiation of the radiotherapy session of the cancer patient, in a sterile test tube under sterile conditions. The collected sample was then labelled and coded to avoid any bias and to keep it anonymous (except for the principal investigator), and then was immediately sent for analysis of the salivary cortisol levels using an ELISA kit (Diagnostics Biochem Canada Inc.), which is the gold standard for analysis. The samples collected were stored at –20°C at the Institutional Research Centre laboratory within half an hour of collection. The analysis was done according to the manufacturer’s instructions.
Inclusion and exclusion criteria
Inclusion criteria were an individual with age 15 years or more, who is a spouse, family member, close relative, or friend of the patient diagnosed with HNC and undergoing radiotherapy, providing care and support throughout the entire duration of their radiotherapy session, and individuals not diagnosed with any systemic diseases and not on any medication.
Individuals with mental and physical disability, who were not willing to provide informed consent, with anxiety disorders and who were on anti-anxiety medication, alcoholics, and smokers were excluded from the study.
Statistical analysis
Data were analysed using the statistical package SPSS 22.0 (SPSS Inc., Chicago, IL) and the level of significance was set at p < 0.05. Normality of the data was assessed using Shapiro-Wilk test. The U Mann-Whitney test and Kruskal-Wallis test were used to assess the difference between the groups, followed by Dunn’s post hoc analysis.
Results
Twenty-eight caregivers of patients undergoing radiotherapy for HNC attending a tertiary care hospital in Mangalore, Karnataka were enrolled in the study. 36% of the participants were males and 64% were females. The majority of the participants belonged to the age group 31–60 years, while there were 5 participants of the age group 10–30 years, and 3 participants belonging to the age group ≥ 61 years. Most of the females were housewives (61%) whereas among the males, 18% were farmers and one participant was a student. Demographic data of the participants were collected (Table 1).
Table 1
Socio-demographic characters of the participants
| Factor | n | Total (%) | |
|---|---|---|---|
| Age | 10–30 years | 5 | 18 |
| 31–60 years | 20 | 71 | |
| ≥ 61 years | 3 | 11 | |
| Gender | Male | 10 | 36 |
| Female | 18 | 64 | |
| Occupation | Farmer | 5 | 18 |
| Clerk | 2 | 7 | |
| Student | 1 | 4 | |
| Businessman/woman | 1 | 4 | |
| Daily wager | 2 | 6 | |
| Housewife | 17 | 61 | |
| Total | 28 | 100 |
Table 2 shows the mean cortisol levels of the participants (n = 28): the cortisol level (ng/ml) on day 1 was 23.67 ±13.80, on day 14 it was 21.62 ±11.35, and on day 21 it was 24.35 ±11.16, with a p-value of 0.68. There is no statistical significance in the levels of cortisol over the calculated time. P < 0.05 was considered as statistically significant.
Table 2
Mean cortisol level of the participants (N = 28)
| Sl. No | Day | Cortisol level [ng/ml] Mean ±SD | p-value |
|---|---|---|---|
| 1 | Day 1 | 23.67 ±13.80 | 0.68 |
| 2 | Day 14 | 21.62 ±11.35 | |
| 3 | Day 21 | 24.35 ±11.16 |
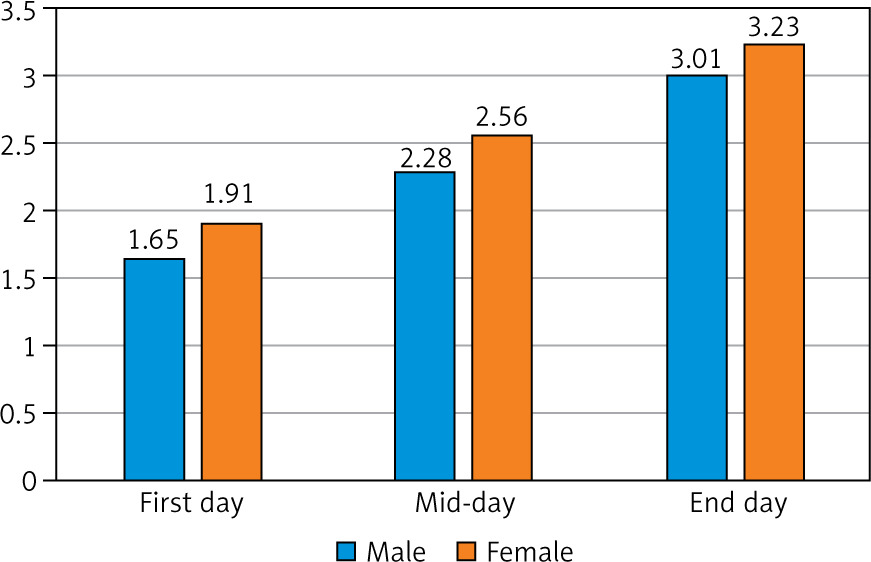
On day 1 (first day of radiotherapy session), the QOL score among males (n = 10) was found to be 1.65 ±0.16 ng/ml, and among females (n = 18) it was 1.91 ±0.24 ng/ml, with a p-value of 0.005. On day 14 (middle day of the radiotherapy session) the QOL among males was 2.28 ±0.43 ng/ml, and 2.56 ±0.33 ng/ml among females, with a p-value of 0.06. On day 21 (last day of the radiotherapy session) the QOL of life among males was 3.01 ±0.47 ng/ml, and 3.23 ±0.51 ng/ml among females, with a p-value of 0.27. The quality of life of the participants decreased in both genders. A comparison of the QOL of participants based on gender is shown in Table 3. A comparison of participants based on their age is shown in Table 4.
Table 3
Comparison of the quality of life of participants based on gender
Table 4
Comparison of mean cortisol level with age of the participants
| Sl. No | Day | Cortisol level [ng/ml] Mean ±SD | p-value | |
|---|---|---|---|---|
| < 40 years (n = 11) | > 40 years (n = 17) | |||
| 1 | Day 1 | 26.53 ±18.93 | 21.82 ±9.41 | 0.38 |
| 2 | Day 14 | 25.34 ±14.94 | 19.06 ±7.56 | 0.14 |
| 3 | Day 21 | 25.36 ±09.39 | 23.65 ±12.84 | 0.71 |
Table 5 shows the overall QOL of the participants during the period of their radiotherapy session. On day 1 the QOL score was 1.97 ±0.28 while on day 14 and day 21 it was 2.53 ±0.31 and 3.15 ±0.26, respectively, with a p-value of 0.0001. Post hoc Dunn test shows the statistical significance (Fig. 2).
Discussion
Caring for a cancer patient is an essential duty that significantly contributes to the patient’s recovery. Being a caregiver has its own myriad of challenges. The majority of people are unprepared for this role. Adjusting to the changes requires time and patience.
In our study, the impact of socio-demographic context among the caregivers of patients undergoing radiation for HNC, on the cortisol level and QOL, was studied. In the present study, 64% of the participants were female. Most of the females were housewives, and one participant was a student. The age of the participants does not show any statistical significance with the cortisol level. A normal level of salivary cortisol is 25.5–68.2 ng/ml, and only the student among all the female participants showed high levels of cortisol in all 3 visits; the rest of the female participants had normal cortisol levels. It could be related to the anxiety felt when confronted with a new or threatening situation with an unknown conclusion. Because the data were gathered during the COVID-19 era, changes in social networks as a result of the COVID-19 crisis may have a direct impact on people’s mental health. It could be a factor in the student participant’s elevated cortisol levels. It is in line with the study conducted by Kawachi et al. [10], and Ryan et al. [11], which shows that the changes in social networking caused increased stress levels and decreased mental health in students. Caregiving is often a long-term challenge; the emotional impact of taking care of the patient alone at a younger age of life also seems challenging for the student participants.
A study conducted by Kirshbaum et al. [12] showed that mean cortisol responses were 1.5–2-fold higher in men compared to women, which is contradictory with the current study. It could be because of cognitive and/or emotional responses to upsetting psychosocial events, which can affect cortisol secretion regardless of gender.
Study conducted by Cauter et al. [13] concluded that during aging, there appeared to be a progressive decline in the inhibition of cortisol secretion in both men and women, which is contradictory to the current study. There is no association found between the cortisol level and age of the participant. Lack of sleep, poor nutrition, high blood pressure, and stress can affect the cortisol level, regardless of the caregiver’s age.
The current study shows no statistical significance in the salivary cortisol levels over the calculated time. One explanation for this could be related to the shifts in the caregiver’s psychological coping and expectations, with early active coping and later loss of expectations of being able to cope successfully [14]. Dysregulation of circadian rhythm during chronic stress is also one of the reasons for this result [15].
A study conducted by Badr et al. [16] assessed the patient’s and caregiver’s distress over the course of their radiotherapy using a 6-week assessment of physical symptoms (MDASI-HN) and distress (NCCN distress thermometer), and they concluded that the patient’s and caregiver’s distress increased steadily over the course of the treatment, making it consistent with the results obtained in the present study, in which the QOL of the caregivers decreased drastically over the course of their radiotherapy session.
The current study found that the male caregivers of cancer patients had more impaired QOL than the females. This finding is in contrast to those of other studies that reported lower QOL among women due to their traditional gender role [17]. In India, women are typically responsible for taking care of the family, while males are expected to provide for the family. As a result, it appears that some men (e.g. sons or husbands) may face additional role strain when forced to balance both their home and work worlds in order to care for a cancer-stricken relative [18].
The results of the current study create an awareness among the healthcare workers and authorities about the mental state of the caregivers of cancer patients. An assessment of caregiver stress might aid in identifying caregivers who require further assistance. Supportive care for caregivers to promote QOL should be investigated with the goal of lessening the burden of caregiving while taking into account other QOL correlates.
Strength of the study
This study is the first of its kind to be conducted among the Indian population, to create awareness among the healthcare workers and authorities about the distress and anxiety affecting caregivers. The saliva samples for the study were collected at a relatively uniform time in the morning, taking into consideration the circadian rhythmic variation in the cortisol levels in the saliva.
Limitations of the study
Our study has certain limitations of relying on self-reported medical conditions and therefore is subjected to bias. The duration of the study was short, and it had a small sample size. Also, the study participants were selected from the inpatient department only; caregivers of outpatients were not included in the study. This can be considered as a major drawback of the study. A longitudinal study with a larger population in multiple settings/centres is recommended to understand more about the biopsychosocial impact of the caregivers.
Conclusions
Cancer has an impact not only on the patients, but also their families. The caregivers of HNC patients are under a great deal of stress and burden while caring for a loved one. The burden and QOL shows a gradual decrease over the calculated period, indicating the distress caused by radiotherapy sessions to the caregivers. The distress caused should be aptly taken into consideration and enable the caregivers/families to have counselling sessions. Also, ideally, managing the time spent with the patient and adopting the virtue of sharing responsibilities should be considered.






